
Abstract
Abstract
Background:
Gastrostomy tube placement is associated with frequent postoperative complications. The aims of this study were to 1) determine the incidence of postoperative gastrostomy complications and 2) determine if patient demographics, comorbidities, or operative technique could predict these complications.
Methods:
A retrospective review was conducted on children who underwent gastrostomy tube placement from June 2006 through August 2009. Patient demographics, comorbidities, operative technique, health care visits, and complications were collected. Data were analyzed by chi-squared analysis (P < 0.05 significant).
Results:
One hundred and fifty-nine patients were evaluated, with the majority of patients <5 years of age (129/159). Ninety-four patients underwent open gastrostomy, 31 laparoscopic gastrostomy, and 34 laparoscopic-assisted gastrostomy. Granulation tissue was the most common postoperative complication, occurring in 58% of patients (93/159). The majority of patients with granulation tissue had full resolution by the fourth postoperative month. Tube dislodgement was the second most common complication, occurring 69 times in 44 of the patients (28%) and resulting in 59 emergency department (ED) visits. Overall, gastrostomy complications resulted in 100 ED and 462 clinic visits. Ninety-three percent (93/100) of ED visits resulted in discharge home from the ED. Gender, age, insurance status, and operative technique were not predictive of complications.
Conclusions:
Granulation tissue and tube dislodgement are the most common complications after gastrostomy placement in children. Gender, age, insurance status, and operative technique were not predictive of complications. Emergency department utilization is high in children with gastrostomy tubes.
Introduction
Methods
The records for all children undergoing gastrostomy tube placement at a stand-alone children's hospital from June 2006 through August 2009 were identified, using ICD-9 procedure codes 43659 (laparoscopic gastrostomy), 43750-51 (open gastrostomy tube placement), 43830-32 (open gastrostomy tube placement neonatal), and 43760-61 (gastrostomy tube change). Deidentified data were retrospectively collected from the charts, including patient demographics, comorbidities, operative technique, and postoperative complications. The number of postoperative health care visits, including those to the clinic and utilization of the emergency room, and telephone calls were also recorded. Early complications were defined as occurring during the initial hospitalization for the procedure. Delayed complications were defined as occurring after discharge from this initial hospital stay. Statistical analysis was performed by using statistical software PASW Statistics 18 (SPSS, Inc., Chicago, IL). Chi-squared analysis was used, as appropriate, with significance determined at P < 0.05.
Operative technique
Open gastrostomies were placed by using a single left-upper quadrant incision, through which the tube was placed and secured in the stomach, using a double purse-string technique to invaginate the gastric wall about the tube. Laparoscopic gastrostomies were performed by using the U-stitch technique described by Aprahamian et al. 4 Laparoscopic-assisted gastrostomy tube placement was performed by using a laparoscope placed through the umbilicus, facilitating grasping of the stomach through a left-upper quadrant incision and then securing it to the fascia.
Results
There were 159 patients that underwent gastrostomy tube placement between June 2006 and August 2009. Demographics are summarized in Table 1. The overall average age was 3.0 years, with a standard error of the mean of 0.4 confidence interval (CI) (2.3–3.6). The age distribution was bimodal (Fig. 1), the first peak with an average age of 12.8 ± 10.6 months and the second peak with an average age of 11.4 ± 3.93 years. Mean follow-up time was 439 ± 309 days.
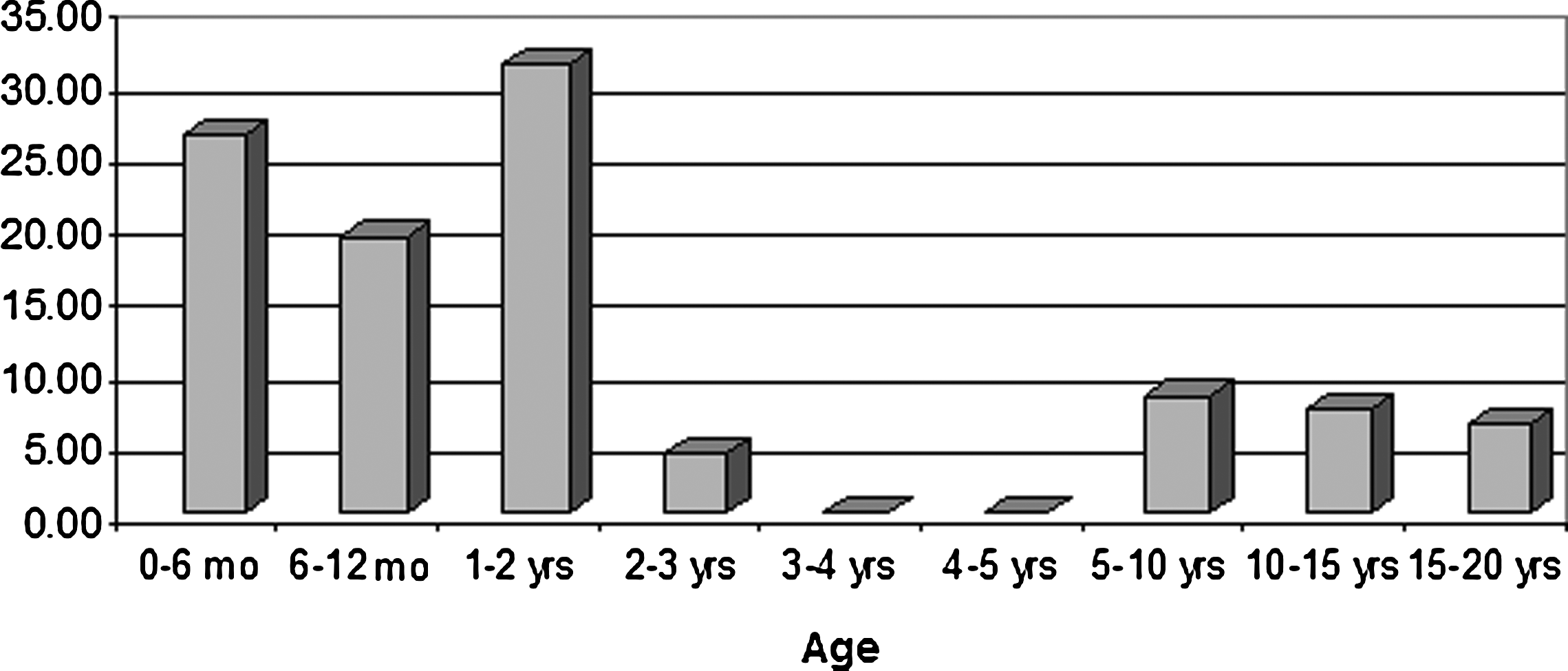
Age distribution of all patients that had a gastrostomy tube surgically placed. There was a bimodal peak, the first peak with an average age of 12.8 ± 10.6 months and the second peak with an average age of 11.4 ± 3.93 years.
(n = 159).
SEM, standard error of the mean; CI, confidence interval; HMO, health maintenance organization; GERD, gastroesophageal reflux disorder.
The most common operative technique used for gastrostomy was the open Stamm (94; 50.3%). The laparoscopic-assisted technique was performed in 34 patients (21.4%) and the pure laparoscopic technique in 31 (19.5%). Fifty-one patients (32.1%) had a conincidental procedure at the time of tube insertion, including 17 that underwent simultaneous Nissen fundoplication. The most common comorbidity was gastroesophageal reflux disease (GERD), with 101 of 159 (63.5%). Fifty-nine patients (37.1%) had neurologic disease. Fifty-seven patients (35.8%) had a genetic disease. Cardiac disease was found in 51 patients (32.1%), and 26 (16.4%) had chronic respiratory disease. Metabolic disease was present in 19 (11.9%) patients. Twenty-one patients (13.2%) had other diagnoses. Twenty-four (15.1%) had a previous abdominal operation.
Table 2 details the rate of early (i.e., during inpatient hospitalization for procedure) and delayed (i.e., after discharge) complications. The overall early complication rate was 13.2%, with the most common being pulmonary embarrassment (n = 9; 5.7%). Feeding intolerance (n = 4; 2.5%), wound dehisence (n = 3; 1.9%), and tube malposition (n = 2; 1.3%) were the next most common early complications. One patient required prolonged hospitalization for uncontrolled pain. One wound infection was treated with incision and drainage. Ileus occurred in 1 patient that had undergone congenital diaphragmatic hernia repair and a Ladd's procedure, along with gastrostomy tube placement.
Delayed complications occurred in 72.3% of patients (115/159). The most common delayed complication was hypergranuation tissue at the tube site (93; 58.5%). Eighty-three of these patients (89.2%) developed granuation tissue in the first 4 months after tube placement. One child required surgery to remove the granulation tissue, while the remaining 92 (98.9%) were treated with topical steroids. Of those with follow-up after granulation tissue was diagnosed, 47 of 67 (70.1%) had complete resolution of their granulation tissue. Five patients had recurrence.
Tube dislodgement occurred in 44 patients (27.7%) a total of 69 times. Twenty-nine patients had a tube dislodgement in the first 4 months after placement. These accidental dislodgements resulted in 50 emergency department visits, 6 additional clinic visits, and 7 interventional radiology visits. No gastrostomy tubes required operative replacement.
Fifty patients (31.4%) experienced leaking around their gastrostomy tube, and 13 (8.2%) developed macerated peristomal skin, which was managed with either a foam self-adhesive dressing or a tube exchange, when indicated. Candidiasis was diagnosed in 9 patients (5.7%), requiring topical antifungal therapy. Delayed wound infections were treated in 8 patients (5.0%) with either antibiotics or incision and drainage. At the completion of this study, 10 patients had their gastrostomy tube removed. Of these, 4 required surgical closure of their gastrocutaneous fistula.
We evaluated for predictors of adverse outcomes after surgical gastrostomy. Table 3 summarizes a subset of these data. Gender, age, insurance status, operative technique, and initial type of tube placed were not found to be risk factors for emergency room visits or early tube dislodgement. We compared the rates of complications between patients with and without the most common comorbidities to determine if any of these diseases or chronic conditions were associated with higher rates of complications after gastrostomy tube placement (not in table format). Patients with cardiac anomalies had higher rates of early tube dislodgement (P < 0.001). Patients with respiratory disease had lower rates of granulation tissue (0.022).
ER, emergency room; HMO, health maintenance organization.
Emergency room utilization is detailed in Table 4. Fifty-five patients (34.6%) made a total of 100 visits to the emergency room for gastrostomy-tube–related complaints. Of those 100 visits, 59 were for tube dislodgements. Seventeen were for drainage around the tube, 6 were for the tube being clogged, and 4 were for generic erythema. Two resulted in diagnosis of malposition of the tube. One of these was a gastrojejunal extension that became misplaced and had to be repositioned in interventional radiology. The other was a patient that presented with diarrhea a few days after the operation and was found to have had the tube inadvertently placed in the colon, requiring an urgent operation for revision. Of these 100 emergency room visits, 93 patients were discharged to home, 5 were admitted to the hospital, and 2 were taken to the operating room. Overall, the 159 patients that had gastrostomy tubes placed made 100 visits to the emergency room, 462 visits to the outpatient general surgery clinic, and required 55 telephone conversations for tube management (Table 5).
Discussion
Surgical gastrostomy tube placement is an intervention associated with a high rate of early and delayed complications. In this study, 73.2% of patients experienced a complication, the majority of which were delayed beyond the immediate postoperative period. Hypergranulation tissue was the most common postoperative complication, occurring in 59% of patients. Tube dislodgement was the second most common complication, occurring in 28% of patients. For 159 patients undergoing gastrostomy tube placement, postoperative care included 100 emergency room visits, 462 clinic visits, and 55 telephone calls. Gender, age, insurance status, and operative technique were not predictive of complications.
Early gastrostomy tube complications have been previously reported in up to 83% of children 5 years after laparoscopic-assisted gastrostomy tube placement, 1 the majority of which was granulation tissue, occurring in 31–51% of patients.1,5 Our data are similar, with a 73% overall complication rate and a 59% incidence of hypergranulation tissue. There were no differences in rates of hypergranulation tissue among various techniques for gastrostomy tube placement. Although hypergranulation tissue rarely leads to more serious gastrostomy complications (e.g., hemorrhage, infection, or tube dislodgement), it can result in peristomal skin irritation, gastrostomy leakage, or minor bleeding from the site. In our study, the majority of patients (47/67) had complete resolution of hypergranulation tissue by postoperative month 4.
Accidental tube dislodgement occurred in 28% of patients in our study. This is much higher than the 4% documented in a study by Jones et al 6 , but lower than the 59% tube-dislodgement rate documented by Lewis et al. 7 Age, gender, operative technique, and insurance status did not predict patients at a higher risk for accidental tube dislodgement. Patients with cardiac anomalies had higher rates of early tube dislodgement (P < 0.001). Only one other study of pediatric gastrostomy tubes has shown similar data, with cardiac patients having a higher rate of overall postoperative complications. 1 Relative to our education practices, patient families received printed and videotaped gastrostomy care instructions, as well as personal teaching by one of three advanced practice nurses. The retrospective nature of the study precluded further identification of more specific information as to why these dislodgements were occurring at high rates among our patients.
Operative technique did not have any effect on postoperative complication rates among children. There is a paucity of literature effectively comparing various techniques for enteral access in children. Percutaneous endoscopic gastrostomy has been widely described,8–10 along with various modifications to the laparoscopic approach.4,6,11 The majority of these studies addressed major complications (i.e., wound infection, gastrointestinal bleeding, and dehiscence), but did not consider granulation tissue or tube dislodgement to be postoperative complications. At the time of writing, there is no strong evidence to advocate for one operative technique, compared to a different technique, in order to reduce the incidence of postoperative complications.
The high rate of complications after gastrostomy resulted in high utilization of outpatient clinic resources and hospital emergency rooms. In this study, postgastrostomy complications resulted in 462 clinic visits, 100 emergency room visits, 7 procedures in interventional radiology, and 3 additional operative procedures among the 159 patients undergoing gastrostomy placement. The economic burden of these visits was not separately addressed in this study, but it is expected to be high. The economic and social burden of the visits on the families is also expected to be high. However, despite these burdens on the caregivers, the quality of life for the children and their caregivers can be markedly improved after gastrostomy tube placement. 12 As more studies address the frequent postoperative complications of granulation tissue and tube dislodgement, perhaps the burden on health care and the families of these children can be further diminished.
Conclusions
In summary, gastrostomy tubes are a necessary and important adjunct in the management of children with many different types of chronic disease. The complication rate after gastrostomy tube is unacceptably high and requires considerable resources for day-to-day management and treatment of common complications. Further research needs to be done to determine what interventions can be made to prevent or more effectively treat these complications.
Footnotes
Acknowledgments
The authors would like to acknowledge research assistant Nicole Loughran, who helped in collecting data for this study.
Disclosure Statement
No competing financial interests exist.