
Abstract
Abstract
Purpose:
To describe a modification in the Georgeson technique for laparoscopic gastrostomy tube (LGT) placement and compare the rate of reoperation for disruption of the gastrostomy tract after LGT by our modified technique to our own series of percutaneous endoscopic gastrostomy (PEG) tubes as well as the published rates of reoperation for LGTs and PEGs.
Methods:
In 2003, we modified our technique for LGT to include laparoscopically placed sutures to secure the stomach to the abdominal wall. A retrospective review was performed on all children undergoing LGT placement and PEGs from March 2003 to October 2009. In addition, a review of the literature was performed to identify the published rates of complications for these procedures.
Results:
During this time period, we have performed 85 LGT using this modified technique. In that same period, there have been 34 PEGs placed. The modification in our technique was instituted after a patient required reoperation for dislodgement in a laparoscopic U-stitch gastrostomy. To date, in the modified LGT group, there have been no disruptions of the gastrostomy tract in either the early or late periods, <90 days or >90 days, respectively. There have been 5 (5.9%) early dislodgements of the gastrostomy tube. All of these were before postoperative day 14 (at postoperative days 1, 2, 6, and 12), and all were replaced with placement verified by contrast study. None required reoperation. In the PEG group, there was 1 (2.9%) early and 1 (2.9%) late dislodgements and tract disruption that required reoperation. The published rate of dislodgement requiring reoperation in the Georgeson series of LGTs is 2.6%. The published rate of reoperation for dislodgement in PEGs is 4%–6%.
Conclusion:
This modification of the Georgeson technique has been successful in reducing the need for reoperation associated with gastrostomy replacement after dislodgement.
Introduction
Methods
A total of 192 gastrostomy tubes were placed by surgeons at Yale-New Haven Children's Hospital from March 2003 to October 2009 identified based on a query run from our billing database for all gastrostomy tubes. After institutional review board approval, a retrospective chart review was performed on all children undergoing PEG (n = 34) and LGT (n = 85) with or without anti-reflux procedure. Approximately one third of gastrostomy tubes placed were performed open because of surgeon preference or concomitantly with other open abdominal surgery. These patients were excluded for this review. Collected data included patient age, sex, weight, indications, comorbidities, technique, operative time, need for anti-reflux procedure, and complications. Complications were defined as early or late, <90 days or >90 days after the gastrostomy tube placement, respectively. In addition, the literature was reviewed to identify the published rates of complications for these procedures. Statistical analysis was performed using Student's t-test; a P value <0.05 was considered significant. All quantitative data were expressed as mean ± standard deviations.
Operative technique
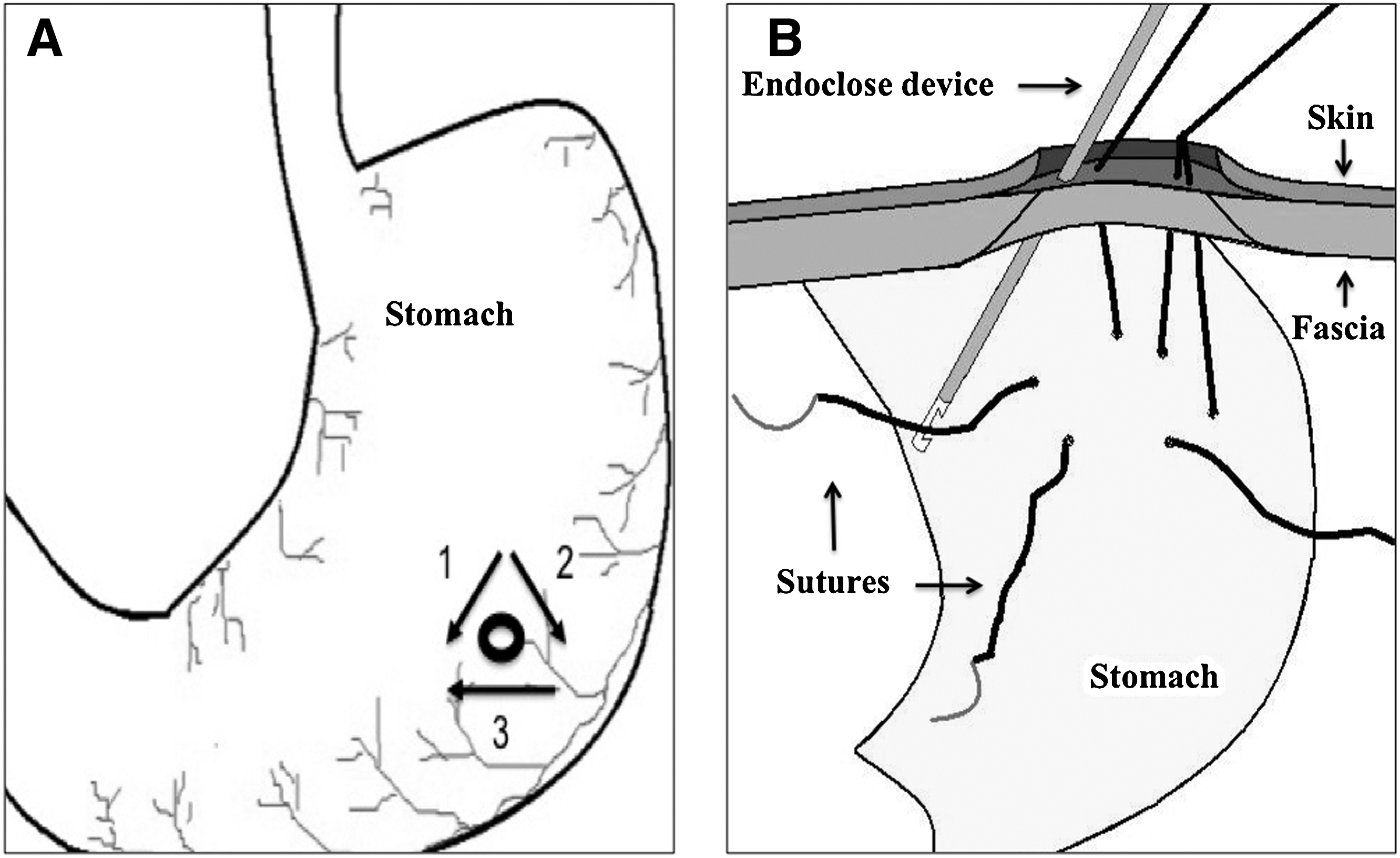
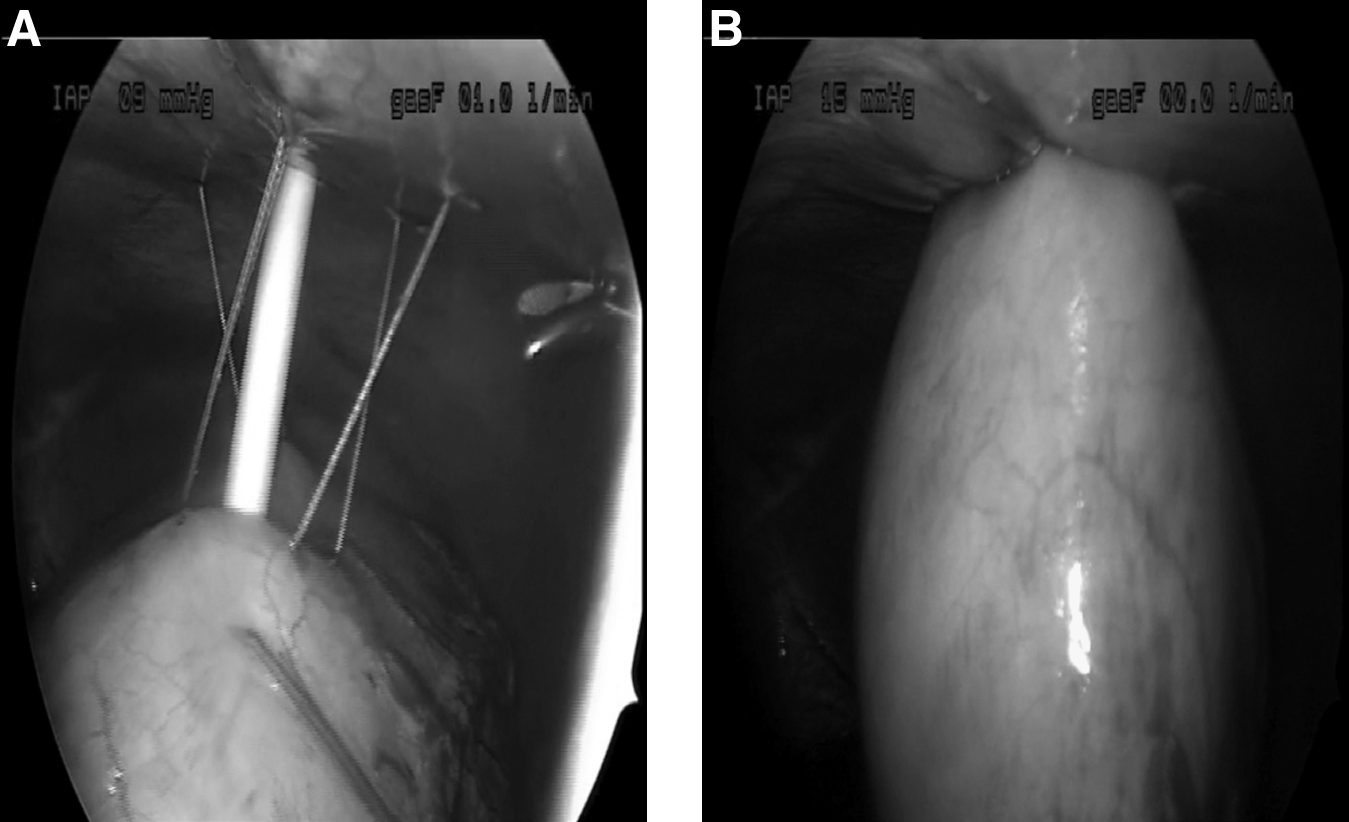
Under general anesthesia, an incision is made through the base of the umbilicus and blunt dissection is used to enter the peritoneal cavity. A 4-mm laparoscopic port is inserted through this incision and the abdomen insufflated until an adequate pneumoperitoneum is achieved. This port is used for a 4-mm 30-degree laparoscope. A 3-mm stab wound is placed in the left side of the abdomen, lateral to the rectus at the level of the umbilicus under direct observation. The stomach is inflated with air via a feeding tube. A site is chosen in the left upper quadrant for a gastrostomy tube placement, an incision is made at the chosen site, and a 3-mm port is introduced through this incision. Three Vicryl sutures, 3–0 on a CV-23 needle, are introduced through the stab incision lateral to the umbilicus and placed using a laparoscopic needle driver through the stab incision. A grasper through the 3-mm port at the gastrostomy tube site is used to assist in the placement of the sutures; this allows placement of the sutures without working paradoxically (not a one-handed task). A site is chosen two-thirds the distance from the gastroesophageal junction along the greater curvature and three interrupted absorbable sutures are placed in the anterior wall of the stomach (Fig. 1A). An ENDO CLOSE™ Trocar Site Closure Device (COVIDIEN, Mansfield, MA) is used to draw these sutures out through the fascia but not the skin (Fig. 1B). These sutures are used to suspend the stomach up toward the abdominal wall (Fig. 2A). After this, the 3-mm port is removed and the large-bore needle is passed through the incision into the inflated stomach and a guidewire is passed through the needle. The tract is sequentially dilated over the guidewire. A gastrostomy button is inserted over the guidewire into the stomach under direct observation and the balloon is inflated (Fig. 2B). The fascial sutures are tied down and the incisions are closed (Fig. 3).

Gastrostomy button final position.
Results
During this period, we have performed 85 LGT using this modified technique, all of which were primary buttons. In that same period, there have been 34 PEG tubes placed. The overall mean age for both groups was 4.4 years (ranging 1 day–26 years) and the mean weight was 5.9 kg. The mean age, sex, and weight of both groups are represented in Table 1. The patients in the LGT group were significantly younger and smaller than those undergoing PEG tubes. The completion rate was 100% for both procedures. The average operating time for LGT group was 43 minutes (ranging 21–68 minutes) and for the PEG group was 19.5 minutes (ranging 10–50 minutes). The longest follow-up for the LGT group was 5.7 years, and for the PEG group was 5.4 years.
P = .02, bP = .0008.
LGT, laparoscopic gastrostomy tube; PEG, percutaneous endoscopic gastrostomy.
The most common indication for gastrostomy tube placement in 51.2% of patients was failure to thrive (Table 2). Additionally, the most common comorbidity was neurologic impairment 36.5%, followed by gastroesophageal reflux disease 29.5%. Comorbidities are summarized in Table 3. Forty percent of the patients in the LGT group underwent concurrent anti-reflux procedure.
GERD, Gastroesophageal reflux disease.
Complications
To date, in the modified LGT group, there have been no disruptions of the gastrostomy tract in either the early or late periods. There have been 5 (5.9%) early dislodgements of the gastrostomy tube (button) in the LGT group. Four of these were before postoperative day 14 (at postoperative days 1, 2, 6, and 12) and one after 1 month, and all of these were replaced successfully at bedside with placement verified by a contrast study. None required reoperation. One patient developed cellulitis 3 weeks after placement and was treated with antibiotics. Our gastrostomy buttons are changed electively after 1 month, and the parents are taught to replace if it is dislodged. There were 6 (7%) late dislodgements of the gastrostomy tube, which required evaluation at the hospital. Two of these were late presentations and the tract was almost closed at presentation. Both were taken to the operating room where the tract was dilated and the button replaced. The rest were replaced at bedside with placement verified by a contrast study. None required reoperation for disruption of the tract or intraperitoneal placement. Only one patient required an anti-reflux procedure 2 months after the initial placement of the LGT, and three patients required redo anti-reflux procedure due to paraesophageal hernias. All early and late complications for the LGT group are listed in Table 4.
In the PEG group, there have been 2 (5.9%) early dislodgements. One (2.9%) required reoperation for intraperitoneal placement. The first patient pulled out the tube on day 4 after placement and was taken to the operating room for exploratory laparotomy and converted to open gastrostomy. The second patient was replaced at bedside on postoperative day 24 with placement verified by a contrast study. One patient developed cellulitis after the low profile conversion clip on the PEG tube became embedded in the abdominal wall and was taken to the operating room to change the tube to a button. After 90 days, there was 1 (2.9%) late disruption of the gastrostomy tract. This patient suffered an intraperitoneal tube placement at the time of her first tube change at 4 months postoperatively. The patient was taken back to the OR for diagnostic laparoscopy and placement of new LGT. Only one patient in the PEG group underwent an anti-reflux procedure after PEG placement. All early and late complications for the PEG group are listed in Table 5.
There were no procedure-related deaths in either group. A total of seven children died distant from their procedures due to complications of their underlying illness.
Discussion
Gastrostomy tubes for the management of infants and children requiring long-term nutritional support in cases of failure to thrive, GERD, neurologic impairment, or oral aversion has been used over the years by pediatric surgeons. 8 The procedure of choice before the introduction of endoscopy or laparoscopic surgery was the use of the open or Stamm gastrostomy. 9 This has dramatically changed over the last 30 years with the introduction PEGs and more recently over the last decade the use of laparoscopic surgery for gastrostomy tube placement.1,4 This latter technique has gained popularity among pediatric surgeons, due to the significantly increase morbidity associated with Stamm gastrostomies (19%) and PEGs (9%–14%).5–7 PEG tube placement, although a minimally invasive procedure, is limited by the size of the endoscope itself precluding its use in smaller infants and many well-known complications such as the risk of inadvertent injury to other organs (1%–3%). 10 Another major complication is tube dislodgement with tract disruption and intraperitoneal placement (4%–6%).9–11 In our institution, the technique chosen was surgeon preference. The older age of the patients receiving PEGs was at least in part because of the technical difficulty and limited equipment available to do PEGs in infants. It is a selection bias against performing PEGS in infants.
With the introduction of the laparoscopic U-stitch technique, many of these disadvantages were negated. Laparoscopy allows for tube placement under direct observation, thereby minimizing the risk of other organ injury. It also allows for primary button placement, which is extremely convenient and valued by caregivers. This technique does not, however, decrease the risk of early and late tract disruption and intraperitoneal placement of the gastrostomy tubes (2.6%). 5 The U-stitches placed during the procedure are typically removed on the second or third postoperative day to prevent site erosion. The modification of our laparoscopic technique to anchor the gastric wall to the anterior abdominal wall combines the security of the open Stamm gastrostomy with the elegance and convenience of the Georgeson laparoscopic technique for placement of a primary gastrostomy button. Avoiding the use of external sutures prevents local erosion, improves the cosmetic results, and more importantly reduces the incidence of tract disruption and intraperitoneal placement either before 90 days or after 90 days. Our overall complication rate was for both PEGs and LGT was 12.8% for patients who required return to the operating room. The complication rate for the PEG group was 11.7% (1 for reoperation for anti-reflux procedure, 1 for migration of PEG, and 2 patients for tract disruption and intraperitoneal placement) similar to the published rates in the literature. The complication rate for the LGT group was 1.1% (one patient requiring anti-reflux procedure after LGT placement). No patient who underwent LGT required reoperation for tract disruption or intraperitoneal placement. Two patients presented late after dislodgement and required return to the operating room for dilation of the tract.
Potential disadvantages of the modification of our technique may include the need of a third stab incision lateral to the umbilicus; this aspect of the operation can be omitted (surgeon preference) since the procedure can be performed through two incisions. The second disadvantage may be added operative time that once the technique is performed routinely might be 5 to 10 extra minutes. Finally, the use of a single-use device (ENDO CLOSE™) for our technique only adds 7 dollars per device per patient. Here we feel that the benefits outweigh the minimal extra cost. If a patient requires exploratory laparotomy for tube dislodgment either during the same admission or a readmission with all the associated comorbidities with this type of complication, the cost would be in the thousands of dollars.
Although the dislodgement rate for gastrostomy buttons that are replaced at bedside is not known, it is of important consideration that this happens regularly in all patients, even multiple times in the same patient. With the modification of our laparoscopic technique, we have increased the security of the gastrostomy tract by subcutaneously anchoring the anterior gastric wall to the abdominal wall. Although the operative time increased when we first instituted this modification, it has since been consistently <30 minutes. We believe that avoiding the need for reoperation for dehiscence of the tract warrants the change in technique and increased operative time.
Conclusion
This modification of the Georgeson technique of LGT placement has been successful in reducing the incidence of reoperation after dislodgement of the button in both the early and late postoperative periods. The technique itself enhances the security of the gastrostomy site without significantly increasing the complexity of the procedure.
Footnotes
Disclosure Statement
No competing financial interests exist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.