
Abstract
Abstract
Background:
Omental infarction (OI) is an unusual, poorly characterized cause of abdominal pain in children and is often mistaken for appendicitis preoperatively. We present our experience with this disease process over a 5-year period to identify preoperative factors to aid in timely diagnosis and treatment.
Methods:
We retrospectively reviewed the medical records of all children that had OI and underwent laparoscopic omentectomy from November 2004 to June 2009.
Results:
Ten patients with the diagnosis of OI were identified. OI occurred in 9 boys and 1 girl, with a median age at presentation of 8.5 years (range, 7–11). Median body mass index at presentation was 23.7 (range, 17–29), with 1 child categorized as healthy weight for age, 1 child as overweight for age, and 5 children as obese for age, based on Centers for Disease Control and Prevention criteria. All patients complained of right-sided abdominal pain; 4 patients complained of predominantly right-upper quadrant (RUQ) pain, 3 patients of right-lower quadrant (RLQ) pain, and 3 of combined RUQ/RLQ pain. On examination, 6 patients had RUQ tenderness and 4 patients had RLQ tenderness. The median duration of symptoms prior to seeking medical attention was 3 days (range, 2–7). All patients underwent computed tomography and the preoperative diagnosis of OI was established in 9 of 10 cases. Operative time was 48 ± 14 minutes. All patients underwent resection of the infarcted omentum; 2 patients underwent concurrent appendectomy. Median length of stay was 2 days (range, 2–4).
Conclusions:
OI occurs predominantly, but not exclusively, in obese preadolescent males. OI can be reliably distinguished from appendicitis on preoperative history, physical examination, laboratory analysis, and imaging. Laparoscopic omentectomy results in prompt resolution of symptoms and discharge.
Background
Methods
A retrospective chart review was performed for all patients identified as having undergone laparoscopic omentectomy from November 2004 to June 2009. Data collected included patient demographics, history, physical examination, laboratory data, radiographic findings, operative findings, pathology reports, and postoperative hospital course.
Results
All preoperative patient characteristics are presented in Table 1. Ten patients with the diagnosis of OI were identified. There was 1 case of recurrent OI 22 months after the initial presentation. OI occurred in 9 boys and 1 girl, with a median age at presentation of 8.5 years (range, 7–11). Complete height and weight information for calculation of body mass index (BMI) was available for 7 patients. Median BMI at presentation was 23.7 (range, 17–29). Based on Centers for Disease Control and Prevention (CDC) criteria, patients with a BMI between the 5th and 85th percentile for age and gender are categorized as healthy weight for age, greater than 85th percentile are overweight for age, and greater than 95th percentile are obese for age. 8 Applying these criteria to our patient population, 1 child was categorized as healthy weight for age, 1 child as overweight for age, and 5 children as obese for age. Additionally, the 3 children for whom height measurements were not obtained had weights ranging from the 95th to 97th percentile for age.
indicates recurrence in the same patient; BMI indicates body mass index; Complaint indicates region of abdominal pain the patient complained of (RUQ = right upper quadrant; RLQ = right lower quadrant); Exam indicates the area of maximal tenderness on physician examination; Preop Dx indicates whether the diagnosis of omental infarction was made preoperatively.
We chose to differentiate between the patients' location of pain versus the physician's finding of tenderness. All patients complained of right-sided abdominal pain; 4 patients complained of predominantly right-upper quadrant (RUQ) pain, 3 patients of right-lower quadrant (RLQ) pain, and 3 of combined RUQ/RLQ pain. On examination, 6 patients had RUQ tenderness and 4 patients had RLQ tenderness. The median duration of symptoms prior to seeking medical attention was 3 days (range, 2–7). The average temperature at presentation was 37.0 ± 0.7°C, and the average white blood cell count was 10.3 ± 2.6 (1000/mcL). All patients underwent preoperative computed tomography (CT), and the preoperative diagnosis of OI was established in 9 of 10 cases (Fig. 1).
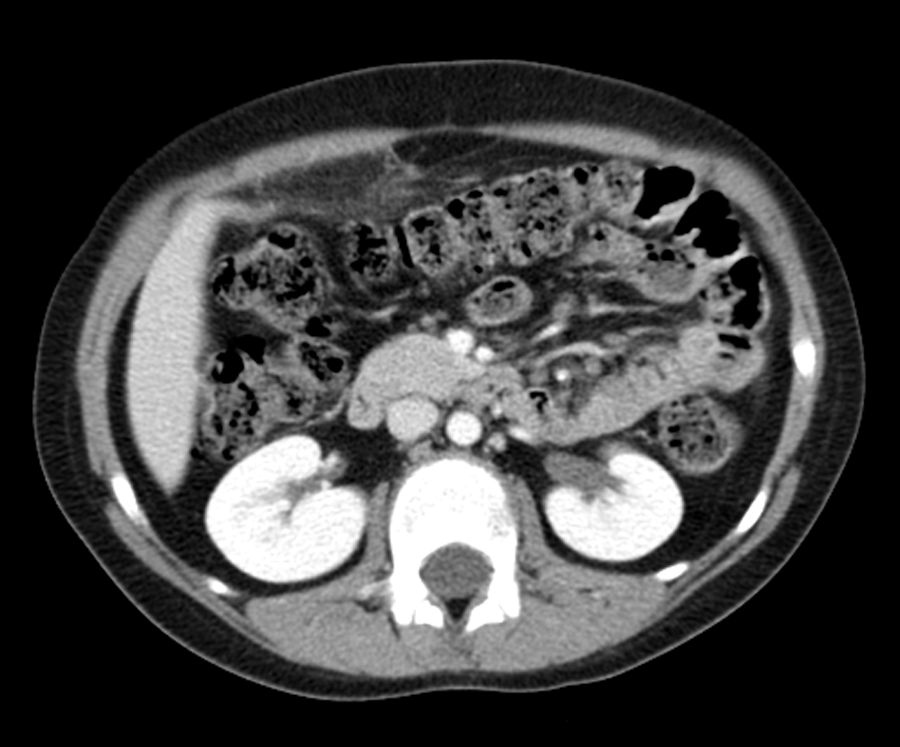
Typical computed tomography (CT) appearance of omental infarction. CT of the abdomen with intravenous contrast demonstrates focal nonenhancing stranding of the fat in a fusiform configuration between the anterior abdominal wall and the transverse colon on the right. There is no bowel wall thickening or adenopathy.
All intra- and postoperative patients characteristics are presented in Table 2. Mean operative time was 48 ± 14 minutes. The infarcted omentum was resected by using LigaSure™ (Covidien, Mansfield, MA) in 2 cases, Harmonic scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH) in 7 cases, and with an endoscopic stapler in 1 case (Fig. 2). Two patients underwent concurrent appendectomy. There did not appear to be any significant differences, depending on the method of division of the omentum or whether concurrent appendectomy was performed. Review of the pathology reports for these two specimens demonstrated normal appendices without evidence of inflammation. Median length of stay was 2 days (range, 2–4), including the day of operation. There were no morbidities or mortalities in the series.
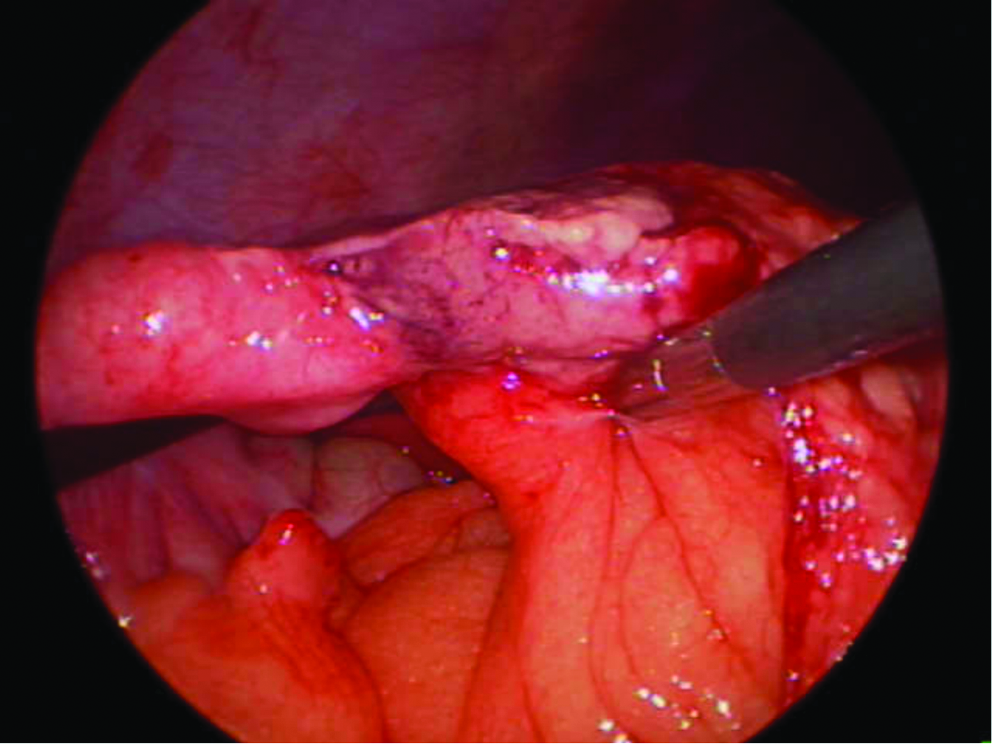
Typical intraoperative appearance of omental infarction.
LigaSure™ (Covidien; Mansfield, MA); Harmonic scalpel (Ethicon Endo-Surgery, Inc., Cincinnati, OH).
Discussion
OI is a rare cause of acute abdominal pain in children, occurring in approximately 0.1% of patients evaluated for appendicitis.6,7 Historically, there has been a great deal of focus in primary care, emergency medicine, and the surgical literature on the preoperative diagnosis of appendicitis in patients presenting with abdominal pain. 9 We have recently shown, and the findings of this study confirm, that pediatric surgeons can accurately distinguish between appendicitis and nonappendicitis causes of abdominal pain. 10 In recent years, there has been an increase in the number of cases series of omental infarction reported in the literature. It is unclear whether this reflects a true increase in the incidence of disease, or that it is a surrogate for the increasing incidence of childhood obesity, or that the widespread acceptance of laparoscopic exploration for acute abdominal pain has allowed its diagnosis.
Multiple groups have previously reported an association between obesity and OI; however, these reports present only weight in kilograms or arbitrary designations of “obese.”1,11,12 BMI, calculated from weight and height, reliably correlates with direct measures of body fat and readily allows for intergroup comparisons. 13 Recognizing that the amount of body fat changes with age and differs between boys and girls, the CDC have published age- and sex-specific BMI-for-age growth charts and weight-status categories for use in pediatric patients. 8 Our series is the first to utilize this classification schema in the discussion of OI. We found that 6 of 7 patients, for whom we had complete height and weight information for BMI calculation, were overweight or obese, reinforcing and extending the findings of prior studies. Others have postulated that greater omental fat deposition in the obese may predispose to omental torsion and infarction by outstripping the blood supply or causing traction. 12 We would argue, in addition, that the android pattern of fat deposition seen in overweight young males may account for the gender predilection over females, who demonstrate a gynoid pattern of fat deposition. 14 Finally, a few researchers have speculated on anatomic variants that may predispose to OI, including bifid omentum, tongue-like omental projections, and constitutive anomalies in the omental blood supply (particularly, the distal right epiploic artery).12,15,16
All patients in our series received CT scans as part of their preoperative work-up for abdominal pain and suspected appendicitis. Other groups have reported the use of ultrasound for the diagnosis of OI, with diagnostic criteria, including “cake-like,” noncompressible, and hyperechoic lesions of omental fat. Ultrasound has the benefit of avoiding exposing the child to ionizing radiation. 17 An important limitation of ultrasound in the evaluation of appendicitis versus OI is the reduced ability to visualize the appendix in obese individuals. CT is not subject to the limitations of operator dependence and may be most useful for identifying alternative diagnoses to appendicitis. 18
It should be noted that we had 1 patient in our series without a preoperative diagnosis of OI, despite receiving a preoperative CT scan. In this case, the CT scan was interpreted by radiology as early apical appendicitis. While the admitting surgeon did not initially agree with the diagnosis of appendicitis, the child's pain persisted during in-hospital observation, and he was taken to surgery on hospital day 3 with presumed appendicitis. The diagnosis of OI was made intraoperatively, and his recovery was uneventful. Interestingly, this was the only patient in the series with a healthy-for-age BMI, which may indicate a difficulty in making the CT diagnosis of OI in patients without excess abdominal adipose tissue.
In our series, 2 patients underwent appendectomy at the time of laparoscopic omentectomy. The pathology in both of these specimens demonstrated a normal appendix without evidence of inflammation. Other groups have variously reported appendectomy as well as cholecystectomy at the time of omentectomy, removing the presumed organ at fault when the preoperative diagnosis of OI was not made. 11 These researchers invariably report the pathology on those specimens to be normal or without inflammation. 11 We conclude, based on those series and ours, that appendectomy is not warranted at the time of laparoscopy for OI.
Recently, some have advocated a nonoperative approach to OI, arguing that it is a self-limiting, benign condition that will resolve spontaneously.1,2,19,20 In these series, time to resolution of symptoms may take up to 2 weeks, and the risk of prolonged pain and abscess formation exists. 21 Nubi et al. 1 reported 10 patients with OI, 4 of whom received “conservative” therapy, consisting of intravenous (i.v.) analgesics for 24 hours followed by oral analgesics, as well as i.v. antibiotics for the duration of hospitalization. In the 6 patients that underwent laparoscopic omentectomy, 3 initially failed “conservative” therapy because of severe pain and persistent peritoneal signs. The patients receiving “conservative” therapy had longer lengths of stay, ranging from 3 to 5 days, which parallels the 1 patient in our series that underwent observation for 2 days prior to observation for presumed appendicitis.
Our series confirms prompt resolution of symptoms and negligible morbidity after laparoscopic resection of OI. Additionally, the benefits of laparoscopy include ease in establishing an intraoperative diagnosis and exploring for alternative pathology when the preoperative diagnosis is not certain, which may be difficult when exploring the abdomen through McBurney's incision. Due to the rarity of OI, it is unlikely that a prospective comparative study of operative versus nonoperative management of OI will be undertaken. However, our series and those of others can be used to discuss the possibilities with families during the informed consent process. While nonoperative therapy results in slower resolution of symptoms and may fail, there are likely fewer long-term complications, such as adhesive bowel obstruction, that are inherent to the operative approach.
Conclusions
In conclusion, omental infarction remains an unusual cause of acute abdominal pain in children and seems to affect primarily obese, pre-adolescent males. Our series demonstrates that the diagnosis can be accurately made preoperatively based on history, physical examination and imaging studies. While it is possible that there exists a subset of patients that will experience prompt resolution of symptoms with analgesia and hydration, perhaps representing intermittent or reversible torsion, laparoscopic treatment results in prompt resolution of symptomatology and discharge home.
Footnotes
Disclosure Statement
No competing financial interests exist.