
Abstract
Abstract
Background:
Laparoscopic fundoplication has not been extensively reviewed to establish the efficacy and outcome in infants. Our aims were to investigate the outcome of laparoscopic fundoplication in infants and assess factors predicting outcome.
Methods:
We performed a retrospective study on infants undergoing laparoscopic fundoplication. Demographic data, operating time, length of hospital stay, complications, and need for redo fundoplication were recorded. Chi-squared test was performed to correlate symptoms and outcome. There were 79 patients. Median age was 6 months (range 0.5 to 11) and weight was 5.6 kg (2.6 to 10). Forty-eight were neurologically impaired, 4 had esophageal atresia and tracheo-esophageal fistula.
Results:
The most common presenting symptoms were vomiting (71), failure to thrive (63), recurrent aspiration (47), and acute life threatening events (35). Thirty-six had severe, 20 moderate, and 19 mild reflux. Three intraoperative complications occurred: 2 (2.5%) conversions (liver bleed, inability to tolerate pneumoperitoneum) and 1 pneumothorax. Median time to full feeds was 4 days (interquartile range 3 to 6) and discharge 6 days (4 to 16). Thirty-one patients had late complications. Nineteen had retching; 2 had dysphagia-needing dilatation. Sixteen patients (20%) had late mortality due to co-morbidities. Fourteen (18%) needed redo fundoplication. There was no correlation between weight, severity of reflux, presence of either ATLE, or neurological impairment and the incidence of recurrence.
Conclusions:
Laparoscopic fundoplication can be safely performed in infants. There was no predictor of recurrence. However, there is a 20% late mortality in patients with severe co-morbidities, which needs to be taken into account when counseling patients.
Introduction
Materials and Methods
There were a total of 79 patients of whom 44 (56%) were male. The median age of the patients at the time of surgery was 6 months (range 14 days–11 months). The median weight at the time of surgery was 5.6 kg (range 2.6 to 10 kg).
A retrospective case note study was carried out after obtaining local ethics committee approval. All children under the age of 1 year presenting to Great Ormond Street Hospital for LNF from October 2003 to January 2007 were included. The LNF was performed using either four or five trocars; a fifth trocar was occasionally used to assist retraction of the esophagus during dissection. Depending on the size of patient, the instruments were 5 or 3 mm. Standard Nissen fundoplication was performed using laparoscopic techniques. In summary, the esophagus was mobilized to achieve an appropriate intra-abdominal length. The hiatus was repaired, and a 360° wrap was constructed using nonabsorbable sutures. The fundal wrap was 2 to 3 cm in length depending on the size of the patient. Division of the short gastric vessels was performed only if required to produce a loose wrap. Postoperative care was standardized by a protocol in place at our institution. Postoperative out-patient follow-up was carried out in all patients. Recurrence was defined as vomiting requiring the restart of anti-reflux medication, the finding of reflux, or wrap failure/migration on investigation and the need for re-do surgery.
Demographic data, indication for performing the procedure, preoperative symptoms, operating time, length of hospital stay, and complications were recorded. There was 100% case note retrieval. No patients were excluded from the study based on size, condition at the time of surgery, or previous surgery. Demographic data are presented as median and interquartile range unless stated. Statistical analysis was performed using Chi-squared test to correlate symptoms and outcome; P < 0.05 was considered statistically significant.
Results
The primary or the underlying conditions of these patients were as follows. Forty-eight (61%) of patients were neurologically impaired, of whom 15 had associated syndromes, 17 had hypoxic ischemic encephalopathy, 2 had cerebral palsy, and 14 had neurological impairment of undiagnosed etiology. Thirty-one patients were neurologically normal; 4 were patients with corrected esophageal atresia.
The presenting symptoms are shown in Figure 1. Vomiting and failure to thrive were the most common; recurrent aspiration and acute life-threatening events (ALTE) were the next most common.

Presenting symptoms in infants with gastroesophageal disease in this series. Numbers represent number of patients with symptom. ALTE, acute life-threatening events.
All patients were investigated preoperatively for evidence of reflux as shown in Figure 2. On the basis of pH study patients were categorized as mild if the pH was below 4 for ≤5% of the time of the study, as moderate if it was between 5% and 10% of the time, and severe for >15% of the time. Patients were indicated to have severe reflux if esophagitis was present and if there was reflux to the upper esophagus/aspiration on contrast study. Overall, there were 36 patients with severe reflux, 20 with moderate reflux, and 19 with mild reflux. All patients were on anti-reflux medication immediately before surgery either in the form of proton pump inhibitors or H2 receptor antagonist and pro-kinetic medication.
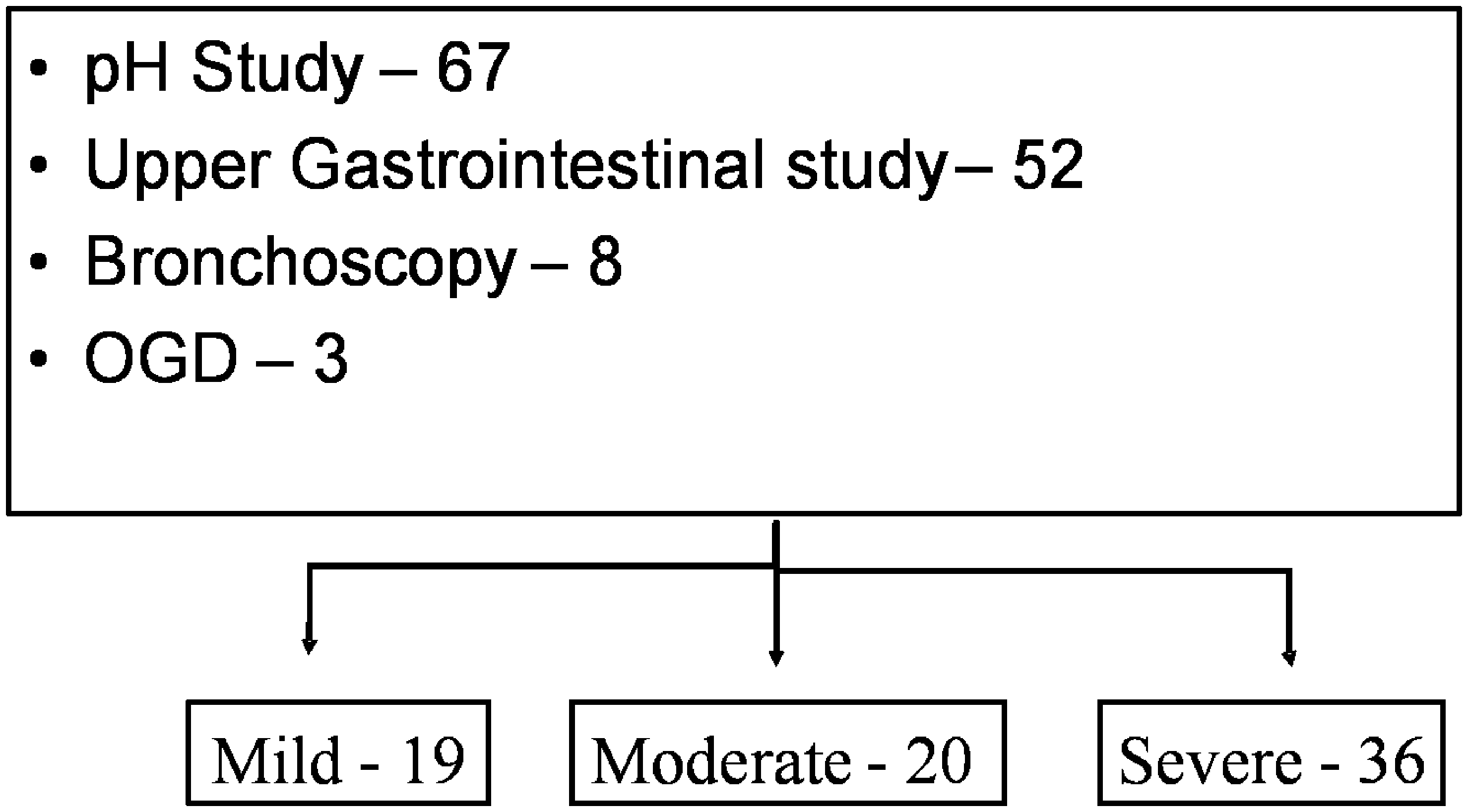
Investigation and classification of the severity of the reflux in patients. OGD, esophago-gastric-duodenoscopy.
The mean operating time was 138 minutes (range 95 to 230, including anesthesia). Sixty-seven patients had formation of gastrostomy and 4 patients had minor procedures under the same anesthetic. There were three intra-operative complications, of which two (2.5%) needed conversion to open procedure. The first patient had bleeding from the liver edge and the second patient was unable to tolerate pneumoperitoneum. The third patient sustained a pneumothorax intra-operatively, which did not warrant a change in approach, and was treated conservatively. Early postoperative complications occurred in 16 (20%). Ten were related to the gastrostomy, and 7 patients developed postoperative chest infection. The median time to full feeds was 4 days (3 to 6 days) and the median time to discharge was 6 days (4 to 16).
Follow-up was between 6 and 58 months with median of 33. Thirty-one patients (39%) had late complications as shown in Figure 3. Nineteen patients had retching; this symptom improved with time and with conservative management resolved in 11 patients. Two patients presented with gas bloat, and changes in feeding regimen solved this problem. Two patients who had dysphagia needed dilatation.
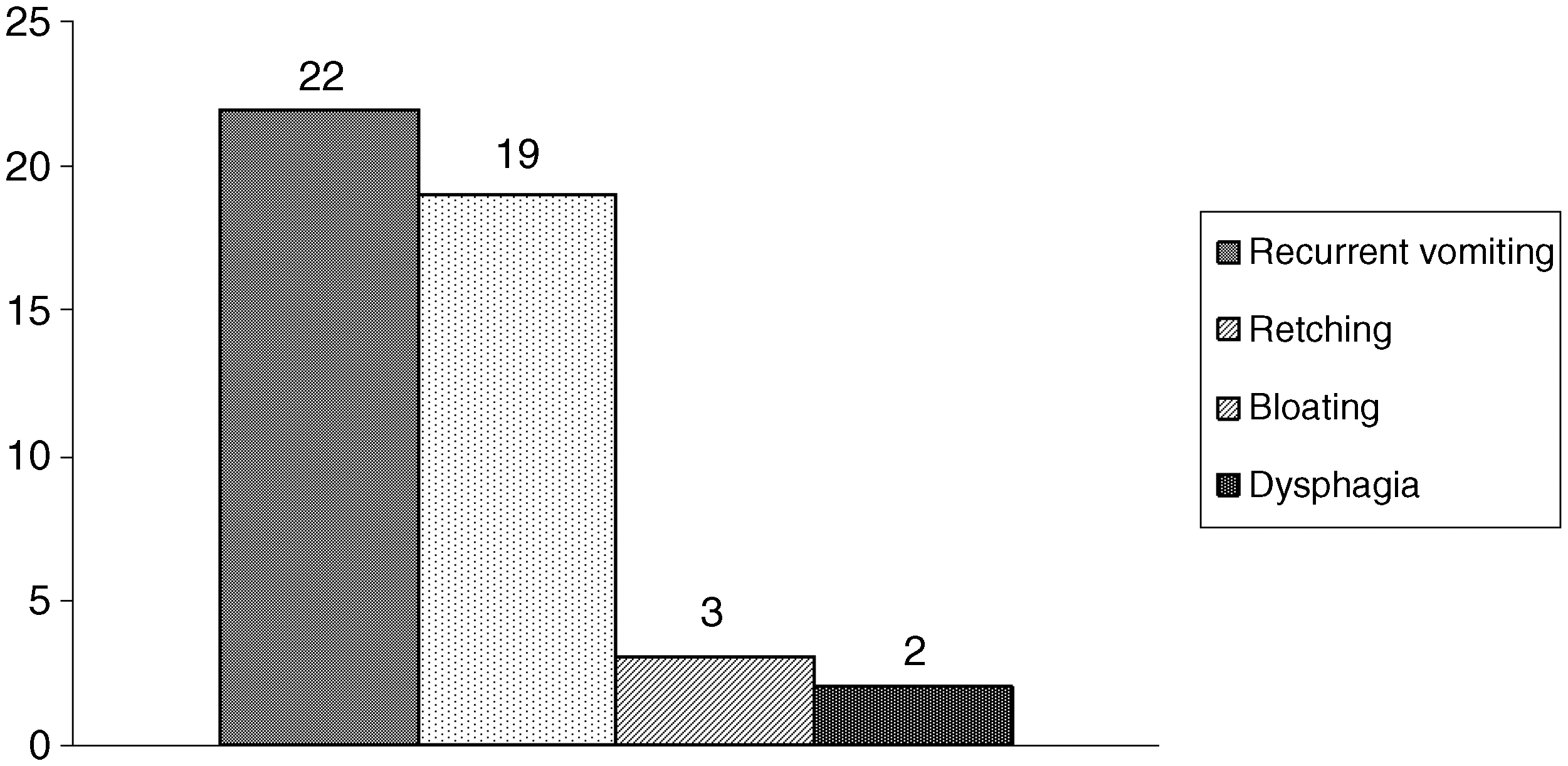
Late complications after laparoscopic Nissen fundoplication. Numbers represent number of patients with complication.
Twenty-two patients (28%) presented with recurrent vomiting and were started on anti-reflux treatment. In 8 patients symptoms resolved; however, 14 patients needed revision surgery (18%). In these, an upper gastrointestinal contrast study demonstrated wrap migration in 8 patients and wrap failure in 6. Seventeen of the 22 patients (77%) with recurrence presented within 1 year of surgery. The median time from first fundoplication to the redo fundoplication was 14 months (range 2 months to 23 months). Severity of reflux did not predict the incidence of recurrence (P = 0.75). There was no significant correlation between patient weight (<5 kg), presence of either ALTE or neurological impairment, and the incidence of recurrence as shown in Table 1.
In 4 patients we were unable to find a record of their exact weight at the time of surgery and were therefore not included in the data for weight stratification.
ALTE, acute life-threatening events.
There was a mortality of 20% (16 patients), at a median time after surgery of 1 year (range 1 to 52 months). None of the deaths were related to the surgical procedure, but were related to the underlying diagnosis.
Discussion
Nissen fundoplication has been the surgical treatment for gastroesophageal reflux disease performed by the majority of surgeons.6–9 It has been 18 years since the introduction of laparoscopic fundoplication 10 ; the favorable results in children have provided the impetus to perform LNF in infants.11,12 This change in trend in favor of surgery is a combined result of the favorable outcome of this surgery in a number of series and the emerging evidence of the role of gastroesophageal disease in ALTE.13,14 In our series, 35 of the 79 infants undergoing LNF had one or more documented episode of ALTE. The indications for surgery in infants are somewhat different from those in older children. Infants are often referred after documented episodes of ALTE. In older children, the most common nongastrointestinal indications are related to chronic respiratory problems 15 with very few exhibiting ALTE.
In this series there were two conversions to open procedure. The first one was to control bleeding. The second one was in ex-premature infant with chronic lung disease, who was unable to tolerate pneumoperitoneum. One patient developed pneumothorax during dissection around the crura of the diaphragm; this, however, did not warrant conversion to an open procedure. We believe that the conversion rate of 2.5% in this patient population is acceptable and similar to other reports. 16
The preponderance of the early postoperative complications was gastrostomy related, mainly leakage from the stoma and skin excoriation. Postoperative retching was another common early complication. Retching after fundoplication occurs predominantly in the neurologically impaired group. This can resolve with changes in the feeding regimen and type of milk. In 19 patients with postoperative retching in our series, 11 resolved with changes in feeding regimen. In some it persists and a trial of alimemazine, an antihistamine that has shown to improve this symptom, may be effective. 17
A recurrence rate of 28% was seen in this series. The need for re-do surgery in this series (18%) is similar in other reviews; ranging from 3% to 15%.16,18 In this study over three-quarter of patients with recurrence presented within 1 year of surgery. These findings are consistent with those reported in older children and adults, in whom the majority of wrap failures occur in the first year.19,20 Patients who presented with recurrence were initially treated medically with anti-reflux medication. If further surgical intervention was being considered, an upper gastrointestinal contrast study was performed to assess the integrity and position of the wrap. Assessment of the wrap in these recurrences demonstrated an equal incidence of wrap failure and migration.
In this series there was a 20% late mortality, all of which were related to underlying conditions. Thirteen of the 16 deaths were in neurologically impaired children and the other 3 had major cardiac anomalies. The earliest death occurred 30 days after surgery in a 9-month-old boy who had spinal muscular atrophy and deteriorating muscular and respiratory function. Long-term mortality has been previously reported in children after fundoplication. Cheung et al. found 20% mortality after fundoplication in neurologically impaired children when followed up for 1.3 to 5.7 year. 21 Bradnock et al. 22 in their series of 85 patients found a late mortality of 7% in children who underwent laparoscopic fundoplication. Tovar et al. 23 reported their series of 252 children who had either open or laparoscopic fundoplication; there were 17 deaths (6.7%), 3 in the first postoperative month and only 1 (0.4%) related to the operation.
Sixteen patients were ventilated at the time of surgery and it was possible to wean 13 of them off the ventilator after surgery. Three patients were on ventilatory support until death. We believe that the improvement in the 13 patients who were weaned off the ventilator was due, at least partially, to resolution of their reflux. Although no respiratory function test was performed to substantiate this, we believe that their clinical improvement and weaning off the ventilator indirectly support this. Improvement in the pulmonary function in children post-fundoplication is consistent with the findings of Rothenberg and Powers.24–26 Therefore, fundoplication is justifiable in infants requiring continued respiratory support and documented reflux.
In conclusion, LNF in children under 1 year old is feasible, effective, and safe, with no immediate surgery-related mortality. However, there is a 20% late mortality in patients in this series as a consequence of associated diseases. This needs to be taken into account when counseling parents. Most postoperative morbidity is temporary, treatable, and not disabling. The requirement for revision in this series (18%) is comparable with many series of open fundoplication in this age group. There were no factors that reliably predict failure, recurrence, or complications in this series.
Footnotes
Disclosure Statement
No competing financial interests exist.