
Abstract
Abstract
Background:
Complete reduction of an indirect inguinal hernia sac during laparoscopic totally extraperitoneal (TEP) repair is not always possible when the sac extends to the scrotum or adheres to adjacent tissues. Laparoscopic TEP repair would be much easier to perform in such cases by transecting the hernia sac. Therefore, the purpose of this study was to determine the safety and efficacy of transection of the hernia sac during laparoscopic TEP.
Materials and Methods:
Five hundred twenty laparoscopic TEP repairs were performed on 498 patients by a single surgeon from July 2003 to December 2008. The patients were classified into two groups: the transected sac (TS) group with 269 patients (275 cases) and the completely reduced sac (RS) group with 230 patients (245 cases).
Results:
Statistical analysis between the TS and RS groups showed no significant differences in postoperative pain, length of hospital stay, and recurrence, except for postoperative seromas, which were more frequent in the TS group (24 of 275) than the RS group (6 of 245; P = .002). And the mean operative time was longer in the TS group (23.62 ± 10.25 minutes) than the RS group (21.49 ± 8.17 minutes; P = .010).
Conclusion:
Although transection of the hernia sac during laparoscopic TEP repair may cause seromas, our study demonstrated that transection of the hernia sac did not cause significant postoperative complications, including recurrence. Transection of the hernia sac is an alternative technique for laparoscopic TEP repair in cases with difficult hernia sac reduction.
Introduction
Materials and Methods
A retrospective analysis of medical records was conducted of patients scheduled for laparoscopic TEP repairs from July 2003 to December 2008. Seven hundred sixty-four cases of laparoscopic TEP repairs were performed for 686 patients by 1 surgeon. The patients were classified into the following two groups: the transected sac (TS) group with 269 patients (275 cases) and the reduced sac (RS) group with 230 patients who underwent complete reduction of the hernia sac (245 cases). The study groups included patients with indirect inguinal hernias; patients with direct inguinal hernias, femoral hernias, obturator hernias, or any type of combined hernias were excluded. Outcome measurements included demographic data and operative results (mean operative time, postoperative pain, seromas, recurrence, and length of hospital stay).
Laparoscopic technique
Laparoscopic TEP repairs were performed using the three-port technique. To create the preperitoneal space, a 12-mm skin incision was made in the inferior edge of the umbilicus. The incision was carried down to the anterior rectus sheath. Then, a small incision was made on the anterior rectus sheath, exposing the rectus abdominis muscle. A channel between the rectus muscle and posterior sheath was created with blunt endopeanuts aiming toward the symphysis pubis. A small tunnel was made in the direction to the pubis between the rectus muscle and the peritoneum. Using a 45 degree telescope and CO2 gas pressure, the preperitoneal space was entered. Finally, two accessory 5-mm ports were created, one port was 2 cm above the symphysis pubis in the midline and the other port was in the middle between the existing two ports.
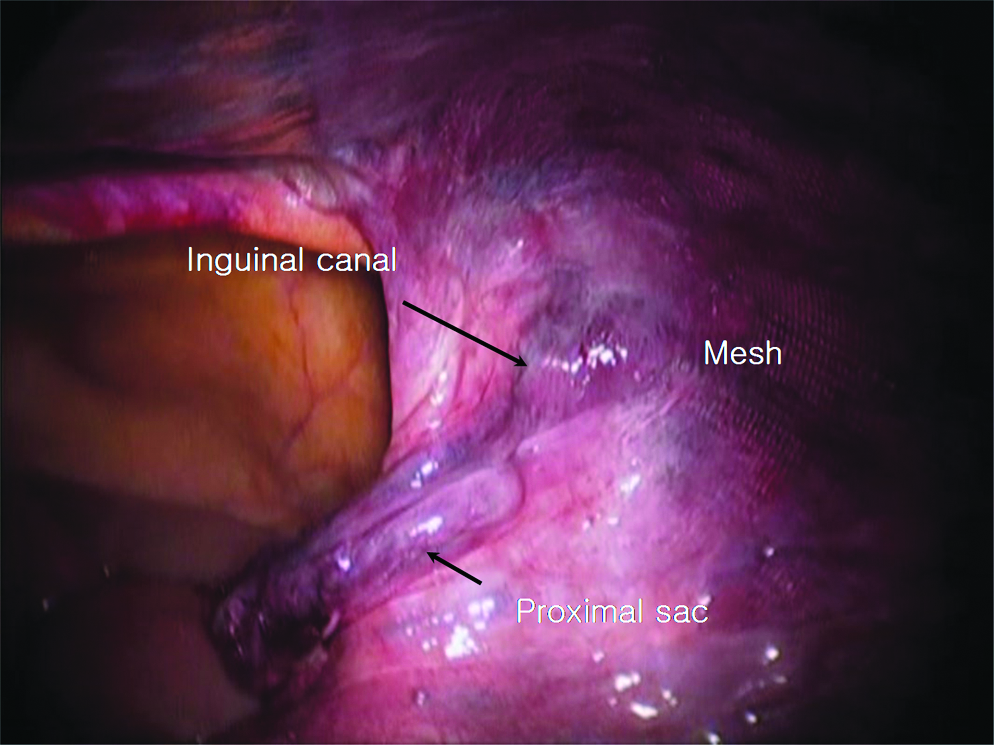
The operative strategy was to perform complete reduction of the hernia sac, but transection of the sac was performed in cases with severe adhesions. In the RS group, the sac was isolated from the vas deferens and testicular vessels, and then it was completely reduced. In the TS group, the sac was isolated from the vas deferens and testicular vessels in an identical manner (Fig. 1) and transected at the midportion (Fig. 2). The proximal sac was twisted and clipped (Fig. 3) to prevent a pneumoperitoneum. In cases in which a pneumoperitoneum was not apparent, the sac was left without clipping. The distal hernia sac was left in situ. A 13 × 8 cm surgipro mesh (Covidien, Mansfield, MA) was placed and anchored with 5-mm spiral tacks (Tyco healthcare, Norwalk, CT) in most patients, or left without anchoring. After that, we explored the intra-abdominal cavity when the possibility of intra-abdominal complications was suspected (Fig. 4).
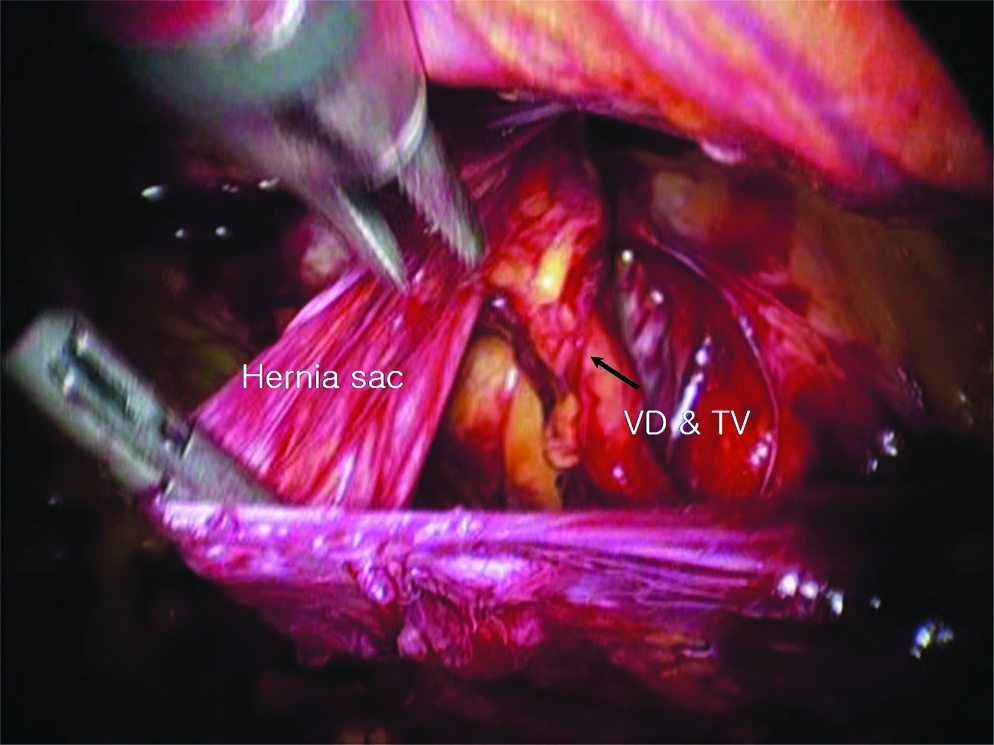
The sac was isolated from vas deferens and testicular vessels.
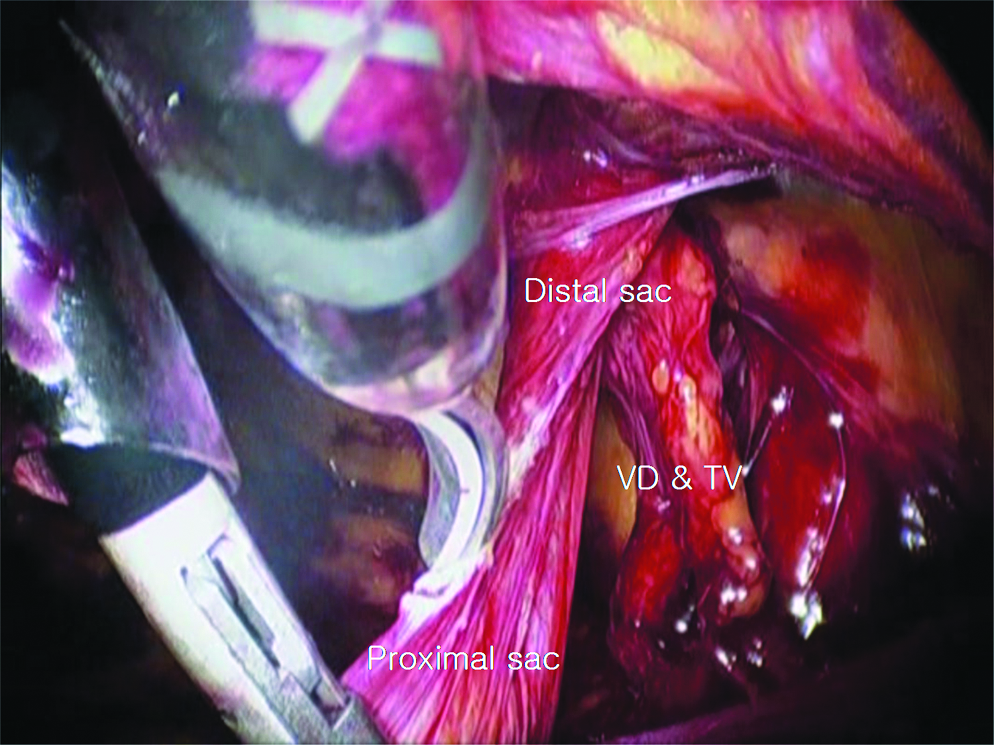
The sac was transected by endoscopic scissors.

The distal sac was twisted and fixed with 5-mm clips to prevent untwisting.
Intraperitoneal findings after transection of hernia sac without clipping.
The operative time was recorded from skin incision to skin closure. Postoperatively, patients who needed more than two doses of analgesics for operative site pain were recorded. A seroma was defined as the presence of a palpable fluid collection or swelling over the operative site or scrotum during follow-up. The length of hospital stay was defined as the total number of nights spent in the hospital after surgery. Most patients were discharged on the day after surgery. The patients were followed up in the outpatient hernia clinic on a regular basis.
Statistical analysis
Operative time, postoperative pain, the occurrence of seromas, length of hospital stay, and recurrence rates were compared by chi-square tests and independent t-test. All data collected in the database were analyzed using SPSS version 12.0. A P value of <.05 was considered significant.
Results
Five hundred twenty cases of laparoscopic TEP repairs were performed in 498 patients. Among the 520 cases, there were 476 males (253 cases in the TS group and 223 cases in the RS group) and 44 females (22 cases in the TS group and 22 cases in the RS group).
Table 1 shows the characteristics of each group. Two hundred seventy-five cases in 269 patients underwent transection of the hernia sac, and complete reduction of the hernia sac was performed in 245 cases of 230 patients. One patient who had a bilateral indirect inguinal hernia underwent complete reduction of the hernia sac on one side and transection of the hernia sac on the contralateral side. The age of the study population ranged from 11 to 88 years, with a mean of 49 years (41.78 years in the TS group and 50.36 years in the RS group). There were 199 cases of left indirect inguinal hernias (100 cases in the TS group and 99 cases in the RS group) and 321 cases of right indirect inguinal hernias (175 cases in the TS group and 146 cases in the RS group). Fifteen cases in the TS group and 11 cases in the RS group were recurrent inguinal hernias.
Table 2 shows the postoperative results between each group. The mean operative time was 23.62 ± 10.25 minutes in the TS group and 21.49 ± 8.17 minutes in the RS group (P = .010). The average length of hospital stay was 0.93 ± 0.47 day in the TS group and 0.93 ± 0.51 day in the RS group (P = .986). Postoperative pain occurred in 7 patients in the TS group and 6 patients in the RS group (P = .994). Seromas occurred in 24 and 6 patients in the TS and RS groups, respectively (P = .002). There were no cases of intra-abdominal complications such as intestinal obstruction during follow-up. There was only 1 case of recurrence in the TS group (no statistical significance). The duration of follow-ups ranged from 6 months to 6 years, with a mean follow-up of 40.8 months.
Discussion
During laparoscopic TEP repairs, complete reduction of an indirect inguinal hernia sac is not always easy, especially in cases with adhesions or in which the hernia sac extends into scrotum. 3 Many surgeons who perform laparoscopic TEP repairs appear to hold the unproven belief that complete reduction of the hernia sac is always necessary. Isolation and transection of the hernia sac might be an option to be applied in difficult cases selectively. Further, transection of the hernia sac is a common technique in open anterior hernia repairs.
Seromas are a common complication after laparoscopic TEP repairs of inguinal hernias, with a reported incidence ranging from 1.9% to 11.7%. 4 Jehaes 5 reported that when a sac of an indirect or direct inguinal hernia is left in the scrotum, a potential cavity exists between the mesh and fascia transversalis, resulting in frequent seroma formation after laparoscopic TEP repairs. In addition, prosthetic materials have the potential to create exaggerated seromas as a result of irritation, followed by serum leakage after incisional hernia repairs. 6 Lau and Lee 7 have reported that after clear identification of the vas deferens and gonadal vessels before transection of a ligated indirect hernia sac, transection of the hernia sac and leaving the distal sac in situ does not result in increased postoperative complications. Surgipro mesh was used in all the cases in the present study, distal sacs were left in situ in the TS group, and postoperative seroma formation was shown to be more frequent in cases of hernia sac transection (P = .002).
Susmallian et al. 8 suggested that seromas are diagnosed clinically in only 35% of cases, whereas ultrasound examination revealed the presence of seromas in 100% of patients, and the amount of fluid collection increases until the 7th day after surgery and then decreases after laparoscopic repair of the incisional hernia. One study suggested that all seromas resolve spontaneously without sequelae by an average of 2.4 months, so expectant management with observation appears to be justified. 4 Additionally, inguino-scrotal hernias have a fourfold increased risk of developing postoperative seromas after laparoscopic TEP repairs. 4 Park et al. 9 have reported that seromas that persist >6 weeks and are symptomatic following laparoscopic repairs of incisional hernias should be regarded as a complication. In our study, there were 30 cases of seromas and most of them disappeared within 7 days, but in 4 cases, aspiration was needed because seromas are persistently found until 30 days after surgery. So in our data, seromas may be influenced by sac transection; however, they was a minor complication, which resolves spontaneously in a short period of time.
The relation between seroma and postoperative pain is interesting. There were 5 cases of postoperative pain among 30 cases of presence seroma, and only 8 cases of pain among 490 cases of no seroma, so it had statistical significance (P < .001). However postoperative pain itself did not show the significant relationship directly to whether transect the sac or not.
Also, transected proximal sac could cause intra-abdominal complications such as intestinal obstruction. However, Figure 4 shows that the mesh did not contact to bowel directly even if the sac was transected, and there was no intestinal obstruction in our data during follow-ups.
There were some more limitations to our study. It is difficult to explain postoperative pain clearly and there were no recorded data available for the severity of pain. Some surgeons have suggested that ligation of the sac could increase postoperative pain after open hernioplasty because the peritoneum is a highly innervated membrane, and ligation of the peritoneum causes ischemia and may augment postoperative pain. 10 Some surgeons have ligated the proximal hernia sac with a clip, or left it unligated. Whether or not to transect the sac was decided intraoperatively by the surgeon in select difficult cases, such as scrotal hernias, incarcerated omental hernias, or young patients with hard and dense tissues.
Conclusion
According to our study, transection of the hernia sac in laparoscopic TEP is safe and feasible even though it is associated with a higher incidence of postoperative seromas, because the seroma is a minor complication lasting for a short time, which subsided spontaneously in most cases. Also, there were no differences in terms of postoperative results between complete reduction and transection of the hernia sac. Complete reduction of the hernia sac might not always be necessary, and transection of an indirect hernia sac could be an alternative option for reduction of the hernia sac during laparoscopic TEP repairs, especially in difficult cases.
Footnotes
Disclosure Statement
No competing financial interests exist.