
Abstract
Abstract
Purpose:
We report our initial experiences with microlaparoscopic cholecystectomy (MLCE) in children using a 2.4-mm mini-scope placed to the right of the umbilicus. The umbilicus was used as the working trocar for large-diameter instruments.
Methods:
The mini-scope was inserted 2–3 cm to the right to the umbilicus and slightly above the umbilical line. A miniport for the 2-mm grasper was inserted laterally through the right abdominal wall, and a 5-mm working trocar was inserted infra-umbilically. The three-angle principle of laparoscopic instrumentation remained, as the trocar positions were merely shifted to the right side of the abdominal wall. With the patient in the supine position, the surgeon stood on the left side of the patient, facing the monitor.
Results:
MLCE was successfully performed in 12 children (average age: 15 years, average body weight: 46.4 kg). In two cases, the optic trocar was repositioned one cm laterally, because the initial trocar position was too close to the umbilicus and was colliding with the 5-mm instruments. The view at the cystohepatic triangle was sufficient. There were no specific complications due to the rearranged trocar positions or the use of a mini-scope. It was possible to displace the scope out of the umbilical area without compromising the superior cosmesis allowed by using only miniports.
Conclusion:
Based on our early experiences, MLCE is safe and feasible. This technique helps reduce the access trauma and operative time while allowing for superior cosmesis.
Introduction
In the recent literature, there are reported attempts to further minimize the access trauma and achieve improvements in the cosmetic appearance after surgical procedures. Natural orifice transluminal endoscopic surgery (NOTES) is becoming popular in experimental settings and in some surgical conditions in adults. However, in our opinion, transgastric, transrectal, and even transvaginal access to the abdominal cavity in the pediatric population appear as unrealistic alternatives to the current minimally invasive surgery.
Single-incision laparoscopic surgery (SILS),5–7 a mini-laparoscopic approach, 8 or even mini-laparotomy 9 for cholecystectomy in children have been sporadically described with the primary aim of minimizing the access trauma. Following this path of evolution in minimal access surgery, we introduced the microlaparoscopic approach for a variety of surgical procedures performed in children during the last four years at our institution.10,11
In this study, we report our initial experience of using the microlaparoscopic approach for cholecystectomy in children with a newly developed 2.4-mm scope in 12 cases while utilizing an unorthodox scope position.
Methods
Between March 2009 and February 2010, we conducted a prospective, nonrandomized pilot study to evaluate the feasibility of microlaparoscopic cholecystectomy (MLCE) in children.
The children with symptomatic cholecystolithiasis considered for cholecystectomy were randomly assigned to the microlaparoscopic approach according to the availability of the mini-scope and a consultant surgeon experienced in microlaparoscopy.
Fully informed consent was obtained by the consultant surgeon; this involved describing the difference between standard laparoscopy and microlaparoscopy to all parents. All procedures were carried out by the first author or by the fellows under his supervision.
All procedures were performed using general anesthesia with endotracheal intubation and were documented by video recording. Data were prospectively collected and retrospectively re-reviewed for the present report. All patients were subjected to follow-up examinations at eight weeks after surgery during a regular out-patient visit.
The indication for surgery was always symptomatic gallstone disease, and all patients underwent detailed preoperative assessment by a pediatric gastroenterologist including a general laboratory examination and liver function tests. Ultrasound examinations to confirm cholecystolithiasis and to exclude obstruction of the biliary tree were performed preoperatively in all patients. Patients with suspected biliary obstruction were referred for magnetic resonance cholangiopancreatography scanning.
Operative technique
The patient was positioned in the supine position, and the surgeon stood on the patient's left side, facing the monitor. A Veress needle was introduced into the abdominal cavity at the umbilicus, and a CO2 pneumoperitoneum was established with an initial flow of 0.3 L/min (to ensure proper placement of the Veress needle) and subsequently increased to 1 L/min. A maximum intraperitoneal pressure of 12 mm of mercury was established. The Veress needle was replaced by a miniport (Autosuture MiniPort, 2 mm, short [7 cm] trocar length; United States Surgical Corp., Norwalk, CT), and a 2.4-mm 0° scope (Storz, Tuttlingen, Germany) was introduced (Fig. 1). This scope was developed in cooperation with the first author of this manuscript, specifically designed for use by the microlaparoscopy study group in our department (There is no potential conflict of interest between the first author and Storz. The first author does not have any financial interest in the sale or distribution of the instrument nor does he receive any type of compensation). After performing a diagnostic laparoscopy with specific attention paid to the anatomical position of the gallbladder, a miniport was inserted 2–3 cm to the right of the umbilicus and slightly above the umbilical line. The mini-scope was repositioned from the umbilicus to the lateral trocar to provide a direct view of the gallbladder. The miniport at the umbilicus was then replaced by a 5.5-mm working trocar for the use of conventional 5-mm diameter laparoscopy instruments including Ligasure, monopolar hook, and bipolar thermocautery devices. Another working miniport for the 2-mm grasper was inserted laterally through the right abdominal wall. In the first five cases, a 2.5-mm liver retractor was introduced directly through the abdominal wall at about 2 cm inferior to the xiphoid process. In the remaining cases, the gallbladder was lifted up by a 2-mm grasper introduced through a miniport placed very laterally in the anterior axillary line and just below the right costal margin. The cholecystectomy was performed beginning with the visualization of Calot's triangle; the dissection of Calot's triangle was achieved in the standard fashion using a monopolar cautery device. Once the cystic artery and duct were exposed, the cystic duct was divided using a Ligasure device, and the cystic artery was divided using a bipolar cautery device. After complete dissection of the gallbladder, it was removed through the slightly widened umbilical incision with the use of a plastic bag of Redon drainage. Before the removal of the gallbladder, it was grasped within the plastic bag by a conventional grasper used in open surgery, and the edge was lifted extracorporeally. The gallbladder content was aspirated with a 12 G needle, thus making the removal of the gallbladder significantly easier, preventing the need for a large incision at the umbilicus. Closure of the fascia at the umbilicus was achieved using 2-0 Vicryl sutures, and the skin closure was performed using 4-0 Monocryl interrupted sutures. The 2-mm trocar sites were infiltrated with local anesthetic, and the skin was approximated using only Steri-Strip™ Adhesive Skin Closures.
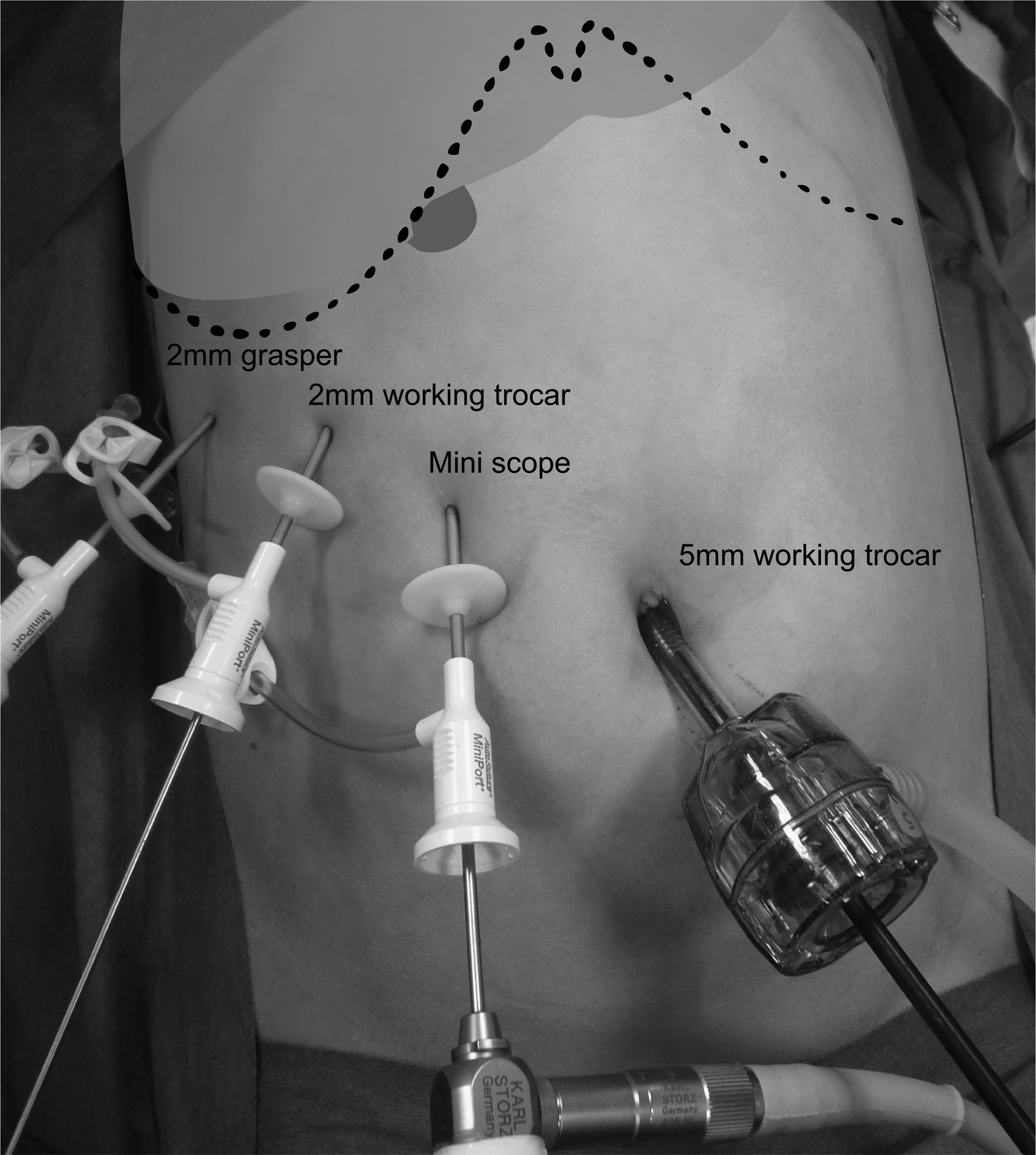
Peri-operative image indicating positions of the trocars.
Results
Between March 2009 and February 2010, a total of 13 children were considered for MLCE. In 12 children (eight boys and four girls), an MLCE was successfully completed. The average age of these patients was 15 years, with a range of 7 to 21 years, and the average body weight was 46.4 kg (range 26–83 kg). In one boy (15 years old with a body weight of 96 kg), the mini-scope had to be replaced by a conventional 5-mm scope due to difficulties when trying to maneuver the scope up or down. The surgeon feared the possibility of fracturing the mini-scope after it had become bent at the very end of the trocar during the laparoscopy due to the very thick abdominal wall in that child.
All patients had a history of recurrent biliary colic and multiple gallbladder stones diagnosed by repeated ultrasound examinations. Two children suffered from sickle cell disease, and one child suffered from spherocytosis. One child had Pendred syndrome, and one had type 1A pseudohypoparathyroidism. The remaining children had idiopathic gallbladder stones; among them, five children were symptomatic after a dietary cure for obesity. In two children, obstructive jaundice and biliary pancreatitis were noted and treated preoperatively. Two patients, each 21 years of age, suffered from severe psychomotor disability and retardation. In one of these patients, previous abdominal surgeries (fundoplication and redofundoplication through upper median laparotomies) were performed during childhood, and both patients had gastrostomy tubes in place during the MLCE.
The mean operative time was 110 minutes, with a range of 45–180 minutes; in 60% of cases, the operative time was affected by fellows performing the MLCE procedure to treat laparoscopic cholecystectomies for the first time.
In two initial cases, the optic trocar was repositioned 1-cm laterally, because the initial trocar position was too close to the umbilicus and resulted in backend instrument collision with the 5-mm instruments at the umbilicus. The view at the cystohepatic triangle was sufficient after repositioning. There were no specific complications secondary to the rearranged trocar positions or due to the use of the mini-scope.
The closure of the cystic duct was sufficient in all cases. There was no biliary leakage noted (either intraoperatively or postoperatively). No postoperative drains were placed in any case, and there were no postoperative wound complications.
In one 7-year-old boy with spherocytosis, a progressive icterus was noted on the first postoperative day. Magnetic resonance cholangiopancreatography revealed a partial stenosis high in the duct, at the area of bifurcation. After diagnosis, an exploratory laparotomy was performed to examine the biliary tree. No direct injury to the common bile duct was found during the exploration, but some thermal changes were detected in the surrounding tissues as a result of transmitted thermal energy. Percutaneous transhepatic biliary drainage was performed in the same session followed by repeated balloon dilations. During the second review of the intraoperative video recording for this patient, it was not possible to determine the moment the injury occurred or the cause of the collateral thermal lesion to the common bile duct. The intraoperative visualization did not play any part in the error. We suspect the cause of this complication was an error of the bipolar cautery device while being used to control minor bleeding.
Histopathologic examinations of the specimens revealed chronic cholecystitis in all cases and fibrosis of the cystic duct in eight cases.
Three patients were discharged within 19 hours after spending one night in the hospital; five patients were discharged on the second postoperative day; and four patients were discharged on the third postoperative day. The boy who required re-laparotomy and repeated balloon dilatation of the common bile duct was discharged 22 days after the initial operation.
At the follow-up visit, which occurred an average of three months post-operation (range 1–11 months), all 12 children who underwent microlaparoscopy were clinically reexamined and the parents were interviewed to assess for cosmesis. No complications occurred after the regular follow-up period. All of the parents were unable to identify the former 2-mm trocar insertion site in the abdominal wall, and the umbilicus appeared scarless with the exception of a thin scar only visible on manual exploration of the umbilical fossa. All but one set of parents were strongly satisfied with both the achieved cosmetic appearance and the surgical procedure. The single exception was the parents of the boy who suffered from the bile duct obstruction and subsequent laparotomy.
Discussion
Dutta, 5 in his report about his early experience with SILS (2009), used the term “stealth surgery” to describe approaches that could be performed without leaving visible evidence that they ever occurred. The author expanded this term to include all approaches aimed at achieving better cosmetic appearance after surgical procedures or those aimed at reducing scar building (e.g., NOTES, SILS), in addition to his previous descriptions of subcutaneous endoscopic techniques.12–14 Additionally, others have used different terms, for example, mini-laparoscopic 8 or needlescopic, 15 to describe procedures with the same goals as mentioned earlier. We use the term “microlaparoscopy” to refer to laparoscopic approaches using exclusively 2-mm instrument sets and scopes less than 3 mm in diameter.10,11 This terminology has been used in gynecology and internal medicine for the last two decades. Since the ultimate goals continue to be not only superior cosmetic appearance but also the minimization of access trauma, such surgical approaches have increasingly appeared in the reported literature. In the cases of elective cholecystectomy, excluding the simultaneous cholecystectomy during splenectomy in children with hemolytic disorders, we had been using 2-mm instrument sets and a 5-mm scope at the umbilicus for visualization (mini-laparoscopy) for the last few years. The results of that series will be separately reported. The primary disadvantage of that technique was that the use of the miniports as the working trocars excludes 5-mm instruments, such as the Ligasure, bipolar thermocautery, or 5-mm suction/irrigation devices. Additionally, to encourage the superior cosmesis and minimal access trauma of mini-laparoscopy, ligatures needed to be manually performed before division of the cystic duct. The 2-mm microlaparoscopes, mainly used for adults, were unable to provide sufficient illumination of the cystohepatic triangle to safely perform a cholecystectomy in children.
In the current study, we used a recently developed 2.4-mm scope (0°, 18 cm length; product number SN 26005 AA, Storz) instead of a standard 5-mm scope. This scope was developed in cooperation with the first author of this manuscript and specifically designed for use by the microlaparoscopy study group in our department. Therefore, it was possible to displace the scope out of the umbilical area without compromising the superior cosmesis that is provided by the use of miniports. This unorthodox scope position allows the surgeon to use the umbilicus as a larger-diameter working trocar with the benefits of the full comfort of conventional laparoscopy. The newly developed mini-scope provides a level of illumination that is nearly identical to that of the standard 5-mm scope.
The mechanical instability of the small-diameter scope was only a problem during a single procedure in a boy with a body weight of 96 kg. Additionally, a higher wastage was noted using the mini-scope within the miniport. The reason for this may be the fact that the mini-scope becomes bent at the very end of the trocar during the laparoscopy when trying to manipulate the scope up or down. To eliminate this disadvantage of the mini-scope, further technical solutions have to be found and are currently the subject of investigation.
The perioperative results and surgical outcomes in the series of patients described in this study are comparable to those reported using either conventional laparoscopy,1–4 mini-laparoscopy, 8 or even SILS for cholecystectomy in children.5–7 In this series, the only serious surgery-related complication, the thermal lesion of the common bile duct, was caused by an error of the bipolar cautery device and was not due to the use of the mini-scope. We feel that the microlaparoscopic procedure results in superior cosmesis and significantly helps reduce access trauma. After the exclusive use of the 2-mm instruments, the scars were, in the majority of the cases, visible to the surgeon only as a small dot on the abdominal wall. We do not require any more of an incision in the abdominal wall than the puncture required for the 2-mm ports. Cholecystectomies performed in children using SILS result in similarly nearly-scarless cosmetic results.5–7 The described disadvantages of SILS are mainly due to the close co-location of the instruments, potentially resulting in bothersome backend collisions that interfere with instrument movement.5–7 Additionally, in our opinion, particularly in the pediatric population, the 2.8-cm large incision at the umbilicus needed for SILS access may not be truly “minimally invasive” access. In the case of MLCE, the golden three-angle principle of conventional laparoscopic instrumentation remains with only a shift to the right side of the abdominal wall.
The mini-laparoscopic approach for cholecystectomy in children described by Seleem et al. 8 required two 10-mm trocars, one of them high at the epigastrium. At present, NOTES seems to be the least appropriate approach for cholecystectomy in children, regardless which one of the so-called natural orifices (vagina, rectum or stomach) is incised for access to the gallbladder.
Conclusion
Based on our early experiences, MLCE is safe and feasible, and it helps reduce access trauma and operative time with a resulting superior cosmesis.
Footnotes
Disclosure Statement
No competing financial interests exist.