
Abstract
Abstract
Background:
Although several studies have reported on the feasibility of robot-assisted gastric cancer surgery using the da Vinci surgical system, reconstruction techniques have depended on staplers or hand sewing through minilaparotomy.
Aim:
The aim of this study is to report on the feasibility of reconstruction methods using a robot-sewing technique in robotic surgery for treatment of gastric cancer.
Patient and Methods:
Between January and April 2010, 7 patients in whom gastric adenocarcinoma was diagnosed underwent robotic surgery including robot-sewn anastomosis. We demonstrated the surgical techniques with analysis of clinicopathologic characteristics and surgical outcomes.
Results:
All robotic surgeries were performed without other laparoscopic instruments. Two Roux-en-Y reconstructions for two total gastrectomy, two Roux-en-Y reconstructions, and three gastroduodenostomies, for five subtotal gastrectomies, were successfully accomplished. Total median operation time was 205 minutes, and median reconstruction time was 69 minutes. One patient was readmitted for stasis in the remnant stomach but conservatively recovered.
Conclusions:
A robot-sewn anastomosis for reconstruction in robotic surgery for gastric cancer was feasible regardless of the reconstruction method.
Introduction
Robotic surgery for treatment of gastric cancer has strength in the aspect of lymph node dissection, in which articulated and nontremorous movement of robotic instruments and three-dimensional visual field may be useful. However, most studies have reported that anastomosis after robotic gastrectomy was performed by extracorporeal hand-sewing sutures or intracorporeal stapler.2–5
Here, we present results of a pilot study in which anastomosis after gastrectomy was successfully achieved by a robot-sewing technique. All procedures, including lymph node dissection and anastomosis, were completed by only the adapting robot, which was different from previous robotic surgery for treatment of gastric cancer, so-called “robotic-assisted surgery,” or “robotic-assisted laparoscopic surgery.”
Patients and Methods
All procedures were performed by the da Vinci Surgical System (Intuitive Surgical, Inc, Mountain View, CA). We began using this system for gastric cancer surgery in October 2008 at Ajou University Hospital, Suwon, Korea. Robotic surgery has been applied to patients in whom early gastric cancer was preoperatively diagnosed. Robotic anastomosis was performed from January 2010 by a surgeon (Dr. S.-U. Han) who had experienced 55 cases of robotic-assisted laparoscopic gastrectomy for treatment of gastric cancer. We obtained informed consent for administration of this anastomotic method from all patients.
Surgical technique
A patient was placed in the reverse Trendelenburg position under general anesthesia. The camera port was inserted into the infra-umbilical area for a 12 mm trocar by the open technique. After establishing pneumoperitoneum, the other four ports were placed under the aid of camera visualization. Three 8 mm trocars were inserted in the left subcostal area, the right paraumbilical, and the subcostal area. One 12 mm trocar for an assistant was located in the left paraumbilical area for insertion of an endo-stapler for resection of the duodenum, the stomach, or the abdominal esophagus and for placement of gauze or a suction device for clearing of the operative field (Fig. 1).
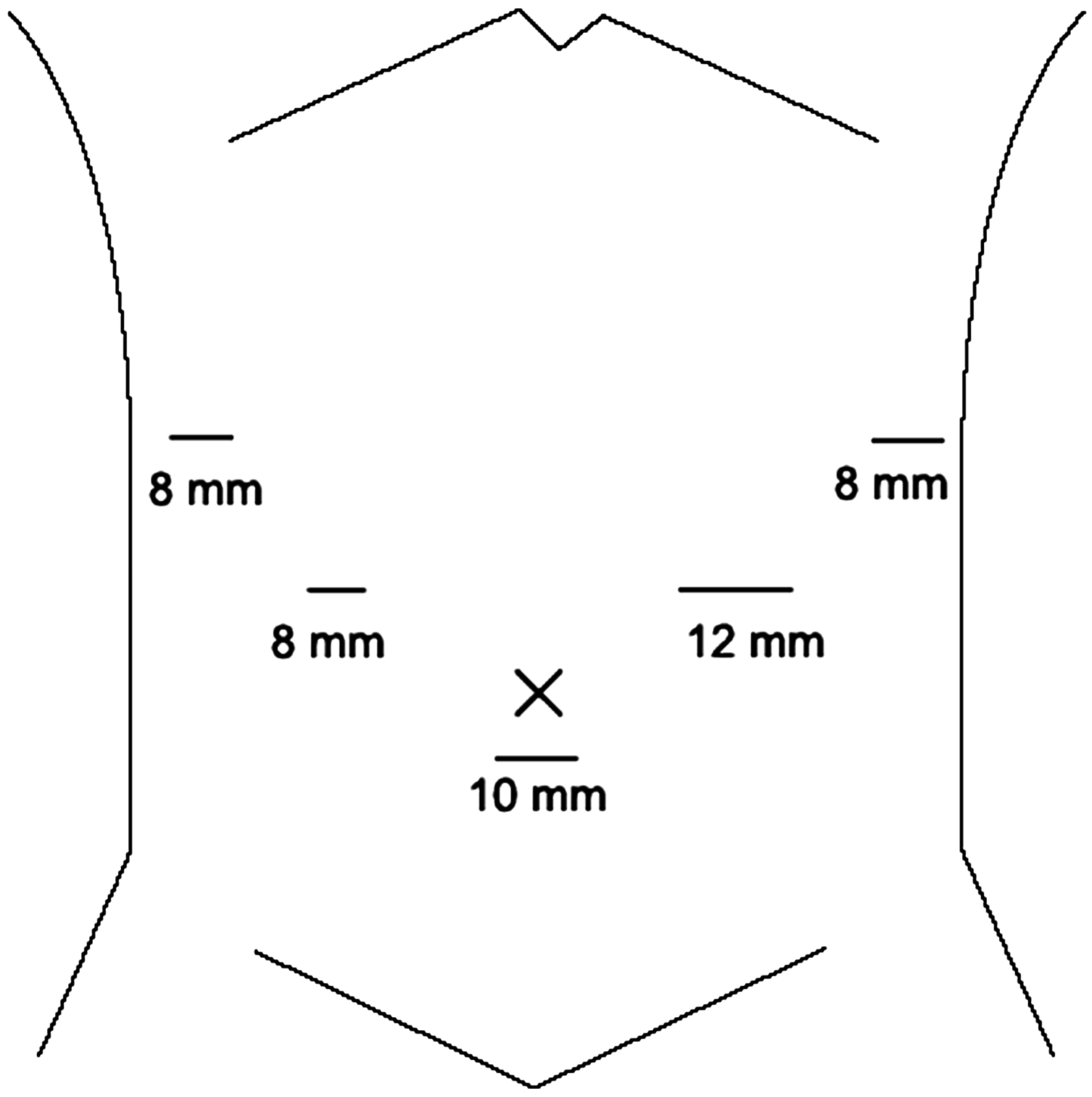
Trocar sites in robotic gastrectomy.
Robotic gastrectomy with lymph node dissection was performed according to standard procedures for laparoscopic gastrectomy, as previously reported. 6 D1 + β lymph nodes were dissected according to the rules of the Japanese Research Society for Gastric Cancer.7,8 Total gastrectomy or distal subtotal gastrectomy was decided according to tumor location.
After distal subtotal gastrectomy, 3 patients underwent gastroduodenostomies and 2 underwent gastrojejunostomies for reconstruction. For gastroduodenostomy, the duodenum was resected by an endo-linear stapler inserted from an assistant's 12 mm trocar. Tow endo-bulldogs were applied in the greater curvature of the stomach to prevent spillage of the stomach contents; resection was then performed using an ultrasonic shear to the middle of the portions where the endo-bulldogs were placed. The remnant portion of the lesser curvature was resected by an endo-linear stapler, and the completely resected stomach was then wrapped by an endo-bag. The posterior walls of the duodenum and the stomach were approximated by continuous seromuscular sutures (Fig. 2A); the duodenal stump was then opened by an ultrasonic shear. A continuous suture with interlocking of the full intestinal layers of the posterior and anterior wall of the duodenum and the stomach was then made (Fig. 2B, C). Finally, the anterior wall of the anastomosis was reinforced by interruptive seromuscular sutures (Fig. 2D). The specimen was extracted from the abdominal cavity through the intraumbilical port site extended to 3 cm.
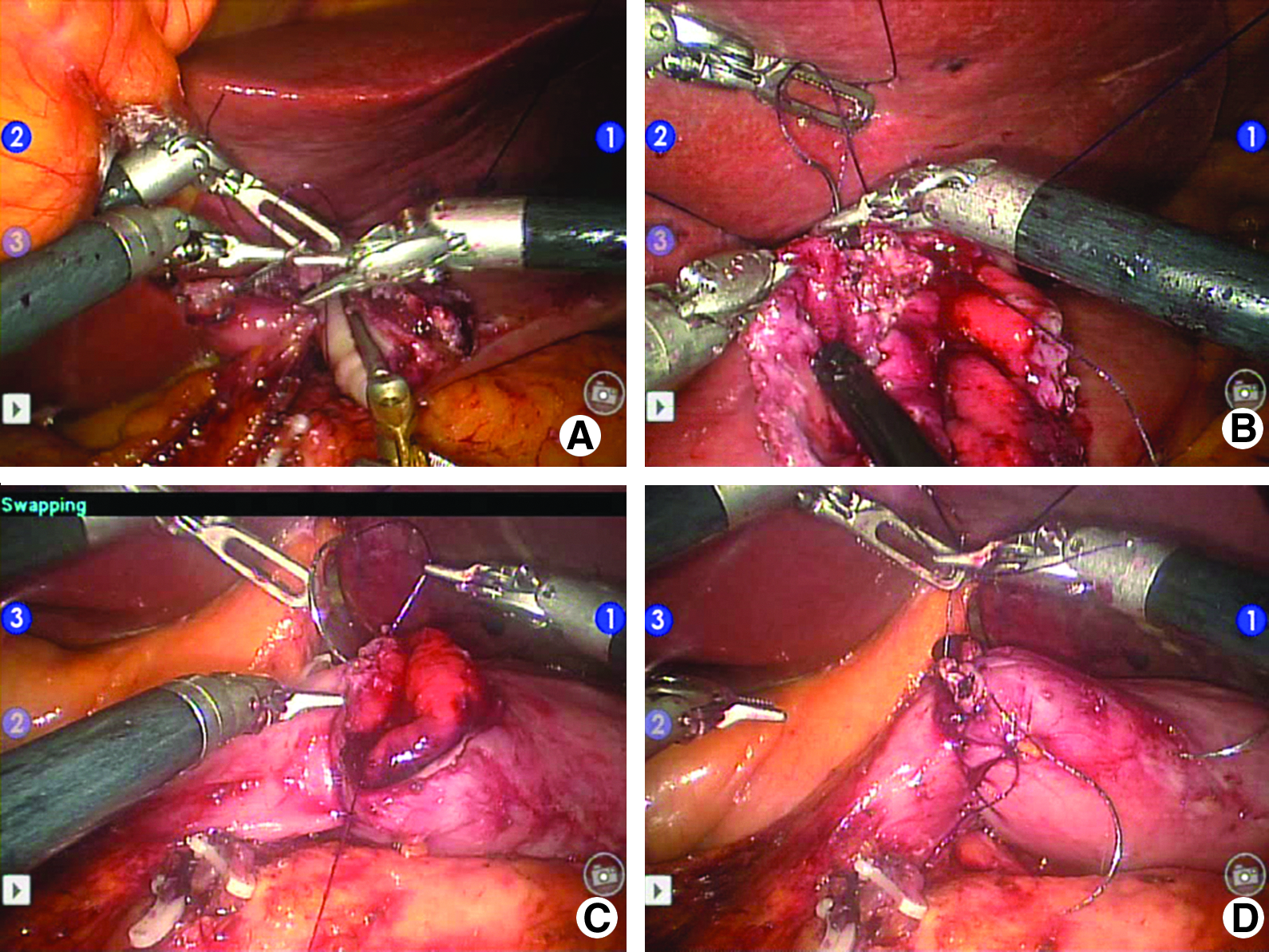
Robotic anastomosis for gastroduodenostomy. (
For Roux-en-Y reconstruction after total gastrectomy or distal subtotal gastrectomy, the jejunojejunostomy and jejunal stump were made using a hand-sewing technique, and the specimen was extracted through the assistant's 12 mm port site in the left side of the umbilicus extended to 4 cm. After closure of the wound, two esophagojejunostomies or three gastrojejunostomies was performed using methods similar to those described above (Fig. 3).
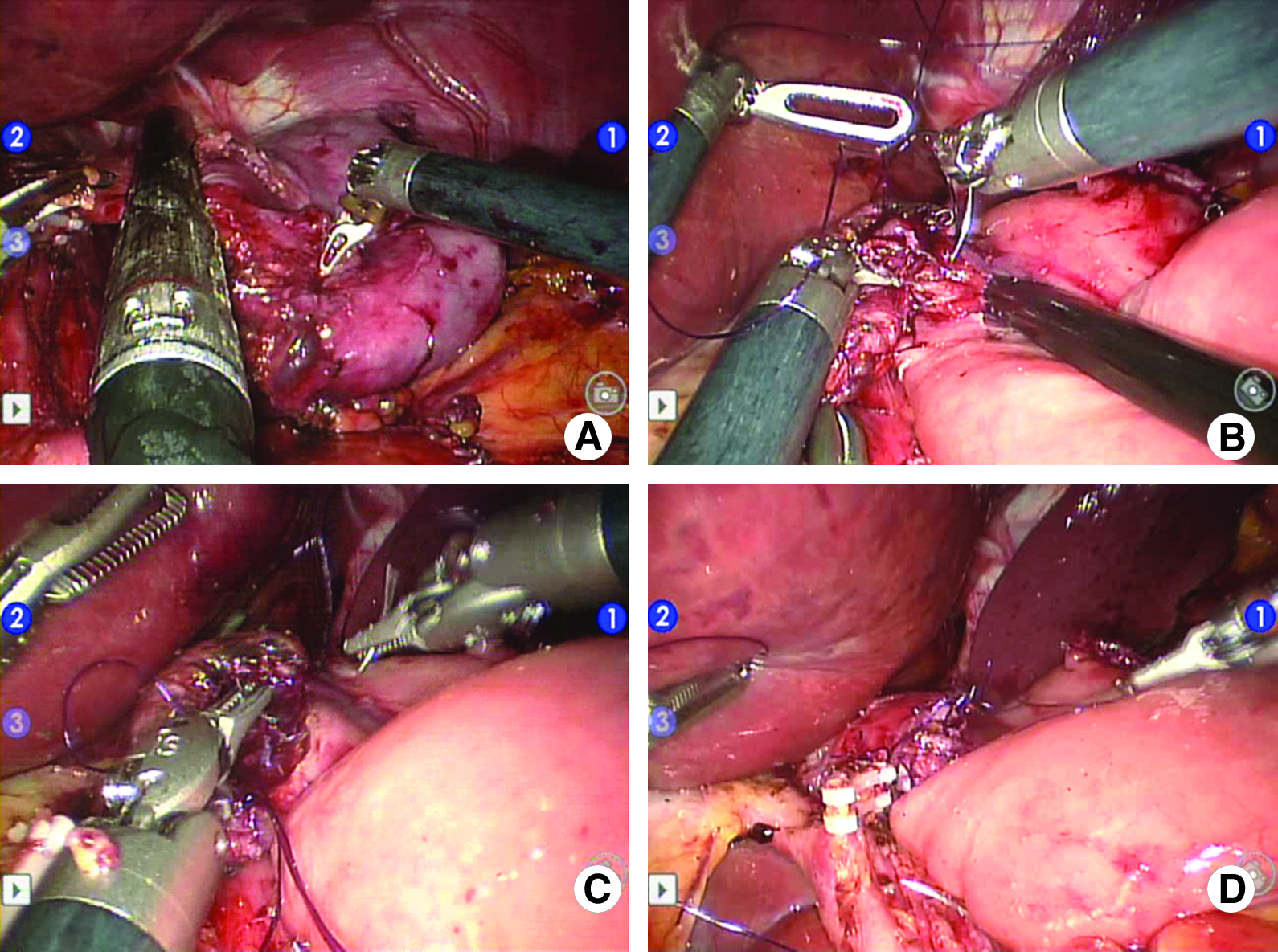
Robotic anastomosis for esophagojejunostomy. (
Results
The total 7 patients in whom gastric adenocarcinoma was diagnosed underwent robotic surgery including robot-sewn anastomosis. The median age of patients was 62 (range: 35–72) years old, and the median body mass index was 24.5 (23.6–27.5) kg/m2. In pathologic findings, the median number of harvested lymph nodes was 36, and no metastatic lymph nodes were found. Primary tumors in 2 patients had invaded the muscle proper; however, those of others were limited to the submucosal layer.
Two Roux-en-Y reconstructions for two total gastrectomy, two Roux-en-Y reconstructions, and three gastroduodenostomies for patients who underwent five subtotal gastrectomies were successfully accomplished. Total median operation time was 205 minutes, and median reconstruction time was 69 minutes (Table 1). The median length of postoperative hospital stay was 9 days. There were no cases of morbidity or mortality during the hospital stay; however, after discharge, 1 patient was readmitted due to stasis in the remnant stomach. He was successfully treated with conservative care.
Discussion
Robotic surgery using the da Vinci system is one of the minimally invasive cutting edge surgical techniques for treatment of gastric cancer. Since articulating instruments of the robotic device may provide complete wrist dexterity, allowing fine control with precision when it comes to the intracorporeal suture, we introduced robot sewing, a new anastomosis method for use in robotic gastric cancer surgery that could avoid minilaparotomy and additional laparoscopic techniques.
A recent trend in minimally invasive surgery for treatment of gastric cancer has been an attempt to reduce the length of skin incision, which is applicable to robotic surgery as well. The first laparoscopic surgery for treatment of gastric cancer was named laparoscopy-assisted gastrectomy, because a small incision was required for extraction of the specimen and for performance of extracorporeal gastroduodenostomy for reconstruction. 9 However, the fact that minilaparotomy itself can cause traumatic stress to surgical patients led to development of a totally laparoscopic technique in which all of the surgical procedures, including reconstruction, are intraabdominally performed under a laparoscopic field.10,11 As for robotic gastric cancer surgery, efforts are being made to perform intracorporeal rather than extracorporeal anastomosis. Although many surgeons still use extracorporeal reconstruction,2–4 a recent study of a large volume center showed the feasibility of intracorporeal anastomosis using staplers; the authors of the study insisted that anastomosis will move from extracorporeal anastomosis to intracorporeal anastomosis with a stapling device. 5 We have also attempted to omit minilaparotomy in performance of robotic gastric cancer surgery using intracorporeal staplers.
During the past several decades, anastomosis using a stapler has facilitated replacement of the conventional hand-sewing technique, because it can reduce operation time and offer consistent results. 12 In particular, with technical advancements in performance of minimally invasive surgery, enteroenteric anastomosis using an endo-stapler has become popular in totally laparoscopic surgery due to the technical difficulty of laparoscopic anastomosis. However, there have been no conclusive results on the superiority of staplers compared with the hand-sewing procedure. Moreover, the staple method could not provide surgeons with as much relief from the risk of anastomotic complications as hand sewing does.13–15 With regard to the increment of the experience about the robotic surgery, we confirmed that robot-sewing anastomosis would be feasible and suitable for overcoming the limitation of the stapling method. In these series, continuous suturing with interlock and reinforced seromuscular suture by the robot-sewing technique may offer the surgeon assurance against risk of anastomotic bleeding or leakage compared with anastomosis using staples.
According to our results, not only anastomosis, such as gastroduodenostomy or gastrojejunostomy, was possible; but also esophagojejunostomy, which should be performed in the deep and narrow space of the abdominal cavity, was feasible. Esophagojejununal anastomosis for Roux-en-Y reconstruction after total gastrectomy is an important procedure, for which failure can lead to postoperative mortality. Since introduction of the circular staple for anastomosis, its use in esophagojejunostomy has been popular, because the surgical outcome was considered to be as reliable as that for the hand-sewing technique.16–18 However, despite the introduction of various methods, use of endo-staplers for esophagojejunostomy in laparoscopic fields has not yet provided confirmation to surgeons.19–21 In robotic surgery for other fields, complex robotic procedures, such as urethral anastomosis in radical prostatectomy or valve replacement in cardiac surgery, were possible in a narrow operative space, owing to three-dimensional visualization, wristed instruments with 6 degrees of surgical freedom, and tremor filtration.22–24 We were able to perform esophagojejunostomy by the robot-sewing technique after total gastrectomy with lymph node dissection. Although the procedure was performed in 2 cases, that procedure was as technically confirmative as hand-sewn anastomosis.
In conclusion, robotic surgery for treatment of gastric cancer is already well known to be technically feasible in lymph node dissection only. However, judging from the advantage of robotic devices such as articulated instruments, enetroenteric anastomosis by the robot-sewing technique will be considerable as a method for overcoming the limitation of anastomosis using a stapler. It may be a standard surgical technique for use in “totally” robotic surgery for treatment of gastric cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.