
Abstract
Abstract
Background:
Laparoscopic surgery has not yet met with widespread acceptance due to its degree of technical difficulty. The laparoscopic radical nephrectomy procedure was improved with the aid of an abdominal wall sealing device, a wound retractor, and a surgical glove.
Methods:
A 5 cm skin incision was made at the beginning of the operation. The Alexis wound retractor S was set up through this small incision. The wrist portion of the surgical glove (size 8-0) was then used to cover the outer ring of the wound retractor to maintain pneumoperitoneum. The surgeon can use most of the usual surgical instruments through the wound retractor during the laparoscopic surgery.
Results:
These procedures were successfully conducted in all cases without open conversion, and no postoperative complications were observed.
Conclusions:
Glove-assisted laparoscopic surgery can be used to perform advanced laparoscopic procedures. This new technique made laparoscopic abdominal surgery easier and safer for beginners in laparoscopic surgery and skilled surgeons in open surgery.
Introduction
Methods
Patients
Six patients (3 men and 3 women) with suspicious renal cell carcinoma underwent a laparoscopic radical nephrectomy (5 cases) or retroperitoneoscopic radical nephrectomy (1 case) using the GALS technique in Toyama University Hospital from September 2009 through February 2010. The mean patient age was 58.0 + 14.4 years (range 37 to 71).
Surgical procedure
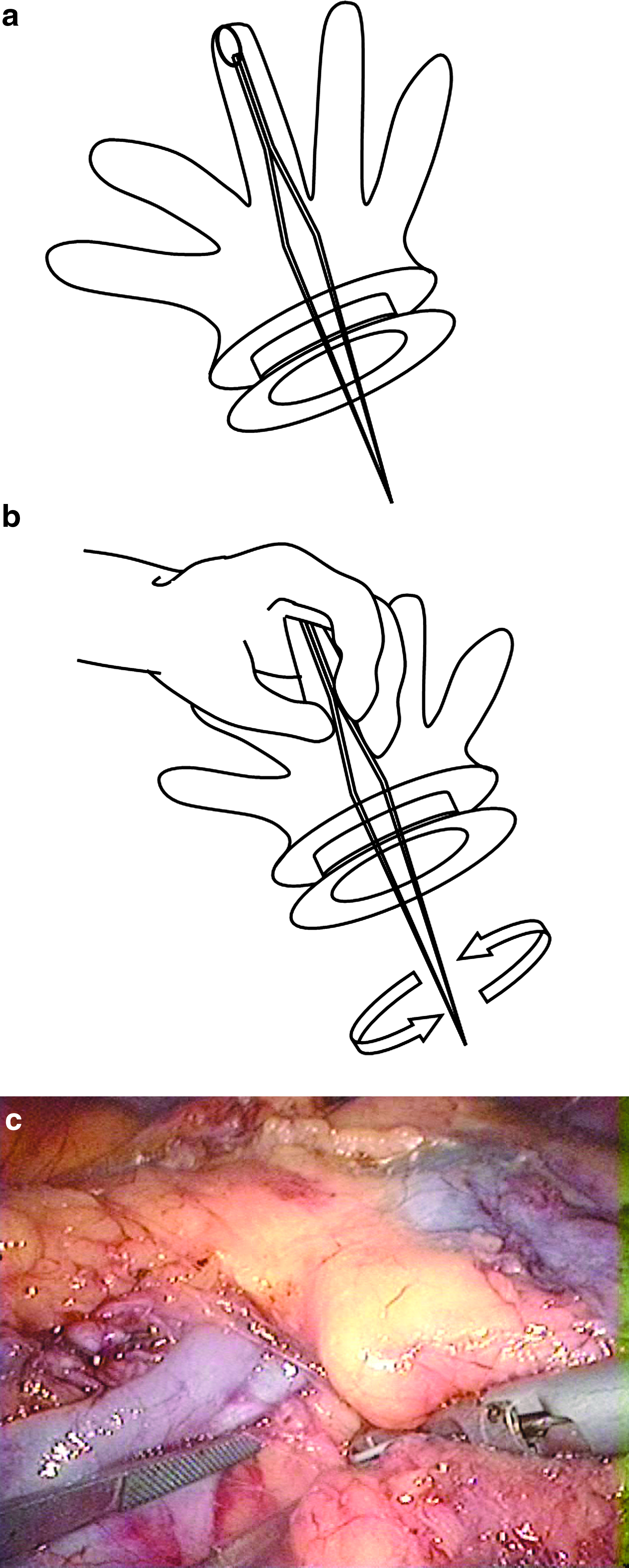
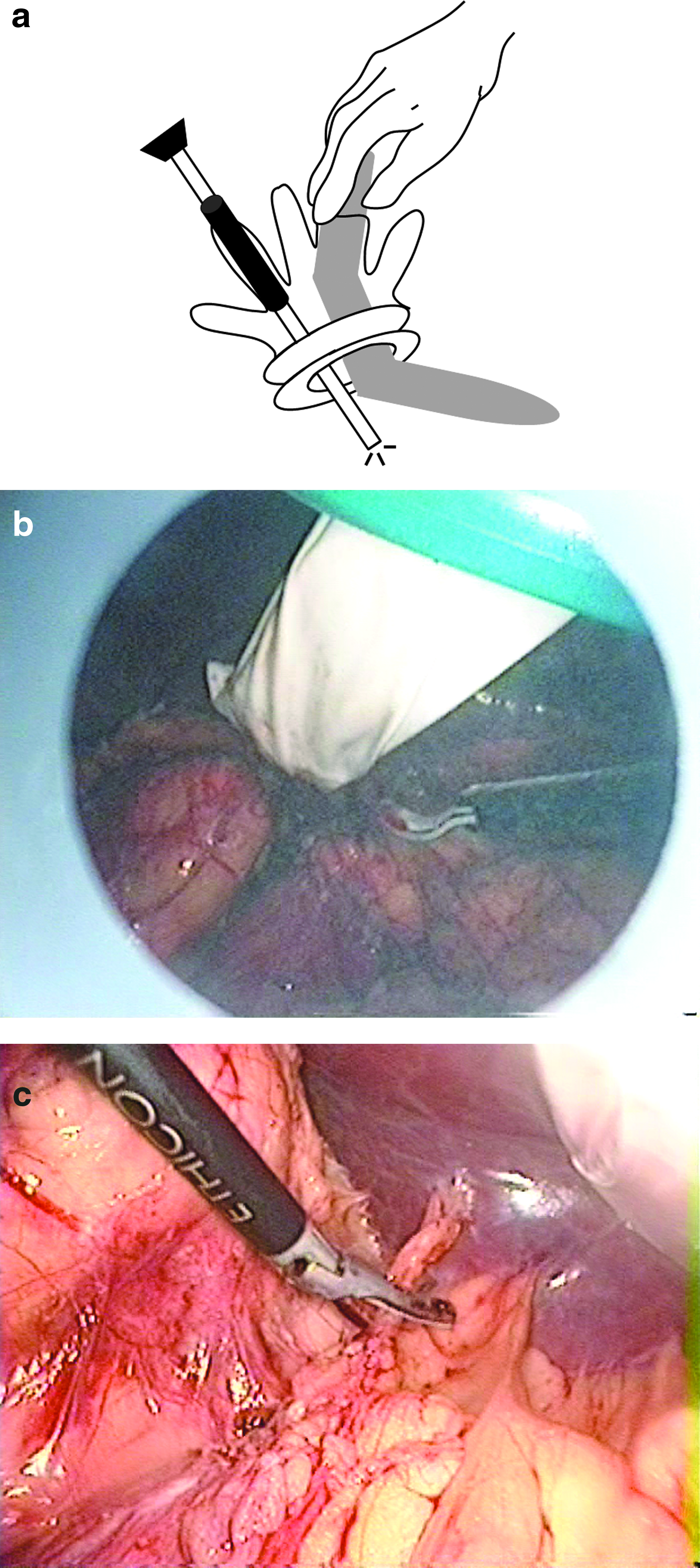
Each patient was put under general anesthesia and placed in a 70-degree lateral decubitus position. A 5 cm skin incision was made at the beginning of the operation. An Alexis wound retractor S (Applied Medical) and a surgical glove (size 8-0) were used as the GALS technique. The wound retractor was set up through the small incision, which was maximized to pass the surgical instruments into the abdominal cavity. The surgical glove was turned inside out, and the forceps was attached to the fingertip with 1-0 silk. Again, the glove was turned outside in and covered the wound retractor. The wrist portion of the surgical glove was used to cover the outer ring of the wound retractor to prevent carbon-dioxide gas leakage during the operation (Fig. 1a). The surgeon grasped the forceps over the surgical glove (Fig. 1b). The forceps allows easy introduction through the wound retractor while maintaining fully mobilization in the abdominal space as in open surgery (Fig. 1c). In addition, the fingertip of the glove was cut off, and a relatively large size of flexible retractor, which had been originally designed for open laparotomy, was used through the fingertip to obtain optimal visualization (Fig. 2a). The retractor spade was bent in the desired direction before use for optimum positioning. The part of the retractor spade that actually displaces the tissue was introduced into the abdominal cavity, and the middle part of the retractor spade was simply stuck to the remaining fingertip with sterile drape tape (Fig. 2b). The distal part of the retractor spade can be hand-held by the surgeon or an assistant. The retractor spade retained the shape of the bend made by the surgeon. The surgeon or assistant grasped the retractor in his or her palm; therefore, this technique restores the tactile sensation to the surgeon. The traction of the organs in the appropriate direction was quite easy and precisely changed in a timely fashion (Fig. 2c). Moreover, the commonly used laparoscopic port was simply stuck to the fingertip with sterile drape tape serving as “multichannel-port” (Fig. 2a). The laparoscope, laparoscopic forceps, or shear were used directly through the fingertip port in the standard manner. These maneuvers were used to mobilize the kidney within Gerota's fascia, and the Gerota's fascia was incised to expose the renal pedicle. The renal artery was clipped and divided. The renal vein was controlled and divided with an endo-GIA applier (ETSFlex 35 mm; Ethicon Endosurgery). The endovascular stapler was introduced through the cutting hole of the fingertip without the intervention of the port. The surgeon grasped the shaft of the endovascular stapler over the fingertip to maintain pneumoperitoneum and then introduced it into the abdominal cavity. The direction and angle of the blade was easily and precisely changed at will. The used fingertip was tied tightly after using the instruments to maintain pneumoperitoneum.
The completely freed kidney was retrieved manually through the wound retractor by removal of the glove without enlarging the primary skin incision and the use of the laparoscopic endopouch bag. Saline irrigation was performed after specimen removal. The drainage tube was introduced though the port site, and the wounds were sutured.
Results
These procedures were successfully conducted in all cases without open conversion. The mean operative time was 287.8 + 69.4 minutes. The mean estimated blood loss was 31.6 + 37.1 mL (range from 10 to 100 mL), and no patient received a blood transfusion. Histopathology confirmed renal cell carcinoma in 4 patients and oncocytoma in 2 patients. All patients resumed oral intake and were ambulatory within 2 days. No postoperative complications were observed.
Comments
A 5 cm skin incision is generally made for the removal of the resected kidney at the end of a laparoscopic radical nephrectomy procedure. However, this incision is performed at the beginning of the operation of the GALS technique. The GALS technique has several unique merits. (1) It used an Alexis wound retractor and surgical glove as a multichannel port. The conventional laparoscopic nephrectomy uses four or five ports of entry into the abdomen. The multiple puncture sites of a conventional laparoscopy may decrease the cosmetic satisfaction of patients and increase trocar-associated complications, such as bleeding, hernias, and wound infection. 1 The number of skin incisions could be minimized to three sites, because the surgical glove can function as a multichannel port. 2 (2) The range of motion was wide with the GALS technique. The use of the wound retractor increases the size of incision, which simplifies the introduction of several surgical instruments simultaneously without coupling. The movements of the laparoscopic instruments are limited by the fixed port in conventional laparoscopic surgery. An endoscopic stapler is sometimes difficult to use through the port in the narrow cavity, because the movement is restricted by the fixed port site. However, the endo-GIA can be introduced through the wound retractor in the GALS technique. The direction and angle of the blade were easily and precisely changed in a timely fashion at will. (3) Various surgical instruments can be used through the wound retractor not only for laparoscopy but also for an open laparotomy. The GALS technique permits the use of larger surgical instruments commonly used in open surgery and can be introduced through this 5 cm in diameter hole. An open flexible retractor was used through the fingertips to obtain a good operative view. In general, a flexible 5 mm laparoscopic snake retractor (Genzyme; Surgical Products) is utilized for retraction of the kidney, liver, or bowel to obtain a good operative view. However, precise and appropriate counter traction by the laparoscopic snake retractor from numerous angles was sometimes technically difficult and dilemmatic. The application of an “open” retractor implies that the surgeon grasps the surgical retractor in his or her palm and introduces it into the intraperitoneal space. The traction of the organs in the appropriate direction was quite easy and precisely changed in a timely fashion without stress. Moreover, this technique restores the sense of touch to the surgeon and thereby avoids the organ damage by excessive and insufficient traction. (4) The same incision was used for kidney retrieval without an additional incision. The resected specimen was retrieved manually through the wound retractor by removing the glove without causing an enlargement of the primary skin incision. Manual retrieval was advocated, because the technique is easy in comparison to the use of the entrapment. This avoids using an ENDOCATCH™ bag (US Surgical) saving about $150. The wound retractor also protects wounds from infection, fascial tear, or skin maceration and avoids port-site metastasis while performing oncologic procedures.3,4
Laparoscopic surgery remains technically challenging and has not become routine for many urologists. Laparoscopic surgery must be simplified to gain widespread acceptance. Hand-assisted laparoscopic surgery (HALS) has been established to perform complex laparoscopic abdominal procedures with tactile sensation.5–8 A hand-access device allows for more facile performance of some procedures in urological procedures, such as a radical nephrectomy, 9 donor nephrectomy, 10 and nephroureterectomy. 11 However, this device is expensive and requires a larger incision. Although the traditional HALS requires a 7 to 8 cm incision, a 5 cm is sufficient in the present procedure. Moreover, HALS restricts the operator's or assistant's hand during the operation, whereas GALS does not. In addition, it is difficult to maintain an adequate working space because of the large size of operator's or assistant's hand, especially using the retroperitoneoscopic approach. The GALS technique maintains an adequate view by using various instruments, such as open flexible retractor. The GALS technique will allow both the surgeon skilled in open surgery and the beginner laparoscopic surgeon to feel comfortable trying laparoscopic surgery with a minimal training period. This may remove the barrier between laparoscopic and open surgery and allow established techniques in open surgery to be utilized in laparoscopic surgery.
Conclusions
The report presents the initial clinical experience with the GALS technique, which provides a simple, reliable, flexible, cost-effective approach to perform a laparoscopic radical nephrectomy. This technique does not require advanced laparoscopic skill while maintaining the advantages of minimally invasive surgery. This procedure can be practical not only for urological surgery but also for the other types of abdominal laparoscopic surgeries.
Footnotes
Disclosure Statement
No competing financial interests exist.