
Abstract
Abstract
Background:
Classical laparoscopic left colon resection requires a minilaparotomy. This wound can cause pain and morbidity. We describe our technique to avoid minilaparotomy by natural orifice specimen extraction.
Methods:
A four-port standard laparoscopic dissection for diverticular disease and small tumors of the left colon was performed. A silicon McCartney tube was transanally inserted into the rectum to remove the specimen and to pass the anvil of the circular stapler into the abdominal cavity. The head of the anvil was mechanically pretilted to facilitate introduction into the proximal colon. Double-stapled anastomosis was performed in the usual manner.
Results:
Eight patients with diverticular disease or small tumors were operated. There were no adverse events. Operating time ranged between 95 and 180 minutes. For malignancies, tissue margins and lymphadenectomy were oncologically adequate. Four week follow-up was uneventful.
Conclusion:
The described natural orifice specimen extraction technique has the potential to avoid incision-related morbidity of the minilaparotomy in laparoscopic left colon resections.
Introduction
Recently, the concept of natural orifice surgery has been introduced clinically to further enhance the positive effects of the minimal invasive approach.1,2 A first step toward clinical application of this idea is the use of natural orifices to get access to the intraabdominal cavity.
In this report we describe our surgical technique of avoiding laparotomy in laparoscopic left colon resections for diverticular disease and small tumors up to 4 cm. The anus, as a natural orifice, was used to insert an additional silicon working port to facilitate transanal specimen retrieval and to deliver the anvil of the circular stapler into the abdomen. Further, a novel technique of anvil insertion into the proximal colon is presented.
Patients and Methods
Patients
From November 2009 to February 2010, 8 patients (3 male and 5 female) underwent laparoscopic left colon resection for diverticular disease (5 patients) or small tumors with a maximum diameter of 4 cm (3 patients).
The preoperative work-up and patient preparation was standard as for colon resection, including complete bowel cleaning. Patients gave their written informed consent.
Technique
The patients were placed in semilithotomy position with spread legs and slightly flexed hips and a pillow was placed under the pelvis for adequate exposure of the perianal region.
Laparoscopic dissection of the left colon was done in the usual standard manner. Pneumoperitoneum was established via a Veres needle. A 10-mm 30° scope and four trocars were used (Fig. 1). For mobilization of the left colon, medial approach was carried out and the left ureter was observed. For malignant disease the inferior mesentery pedicle was isolated, and the inferior mesenteric artery and vein were coagulated and cut by a 10-mm Ligasure device (Valleylab, Boulder, CO). The plexus of the hypogastric nerves was preserved. The splenic flexure of the colon was mobilized by standard medial to lateral approach.
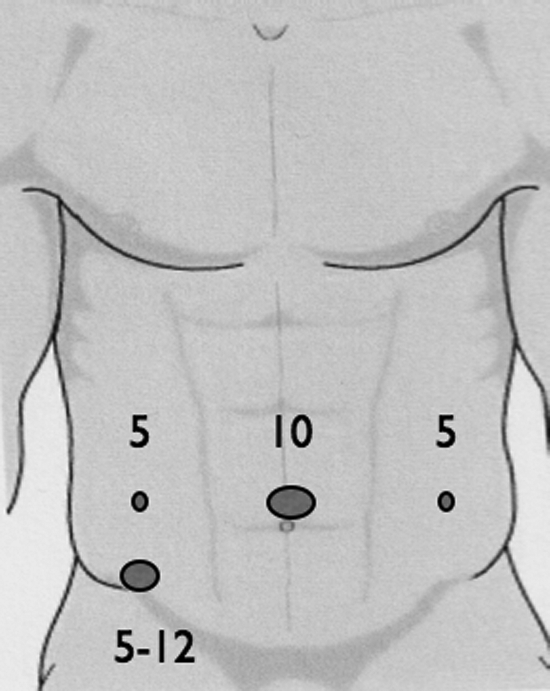
Trocar size (mm) and positions.
For diverticular disease, inferior mesenteric artery and vein were preserved and the sigmoid arteries were divided along with the mesentery with the Ligasure device.
The rectosigmoid and upper rectum were mobilized by creating a dorsal mesorectal window and cutting the lateral ligaments toward the distal resection line of rectum. Then, the mesorectum was dissected and the rectum wall was completely freed from fatty tissue at a length of 3 cm to define the distal resection line. The proximal resection line was placed 5 cm above the tumor or inflamed bowel segment. Then, the bowel was transected at the defined proximal and distal resection lines by linear blue cartridge ENDO-GIA (Tyco Healthcare, Norwalk, CT) to gain the colorectal specimen.
In the next step the rectal stump was washed out with betadine solution and a McCartney tube (MT; Tyco Healthcare) was placed through the anus. On the backtable the anvil of the 28-mm circular stapler (Premium Plus CEEA; Tyco Healthcare) was prepared with the aim to simplify the insertion into the proximal colon. The spring of the anvil was removed, allowing the anvil head to tilt. A shortened gastric tube of 10-cm length was connected to the shaft of the anvil, and a 2-0 monofilament suture was used to hold the head in the tilted position (Fig. 2).
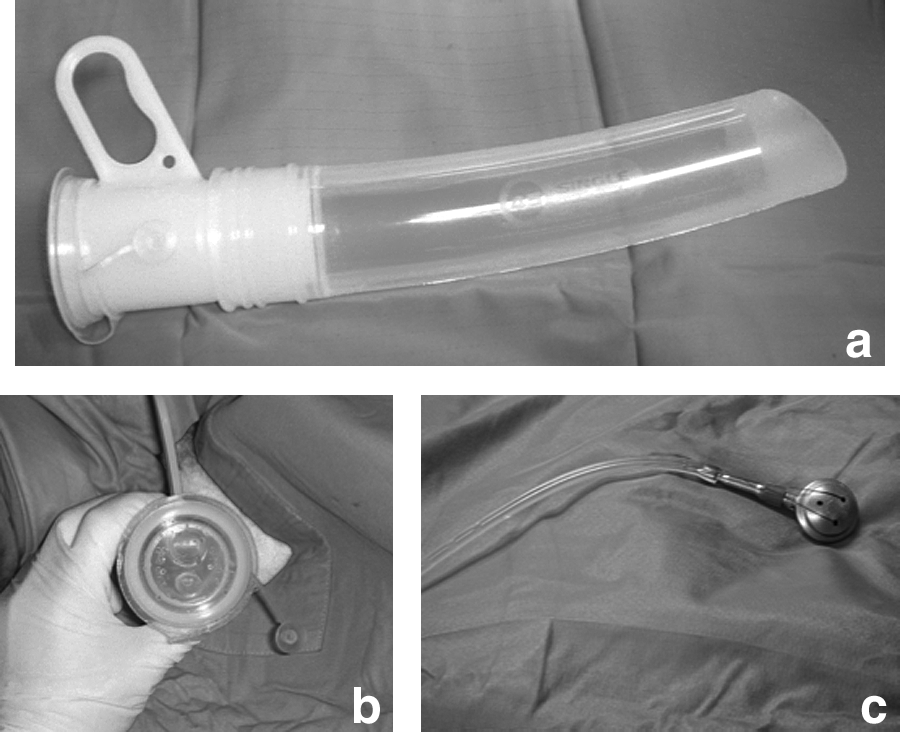
(
Then, the laparoscopic surgeon opened the rectal stump widely along the stapleline. The complete bowel specimen was grasped by a babcock clamp that was inserted through the anal port. With three 5-mm laparoscopic forceps the rectal stump was kept open and the colon specimen was pulled through the rectum and the MT (Fig. 3). In case of diverticulitis the inflamed mesentery of the specimen can be too bulky to fit through the rectal stump. In this situation we separate the mesentery tissue from the bowel wall, resulting in two or more separate specimens. Through this maneuver, removal through the rectum was made possible.
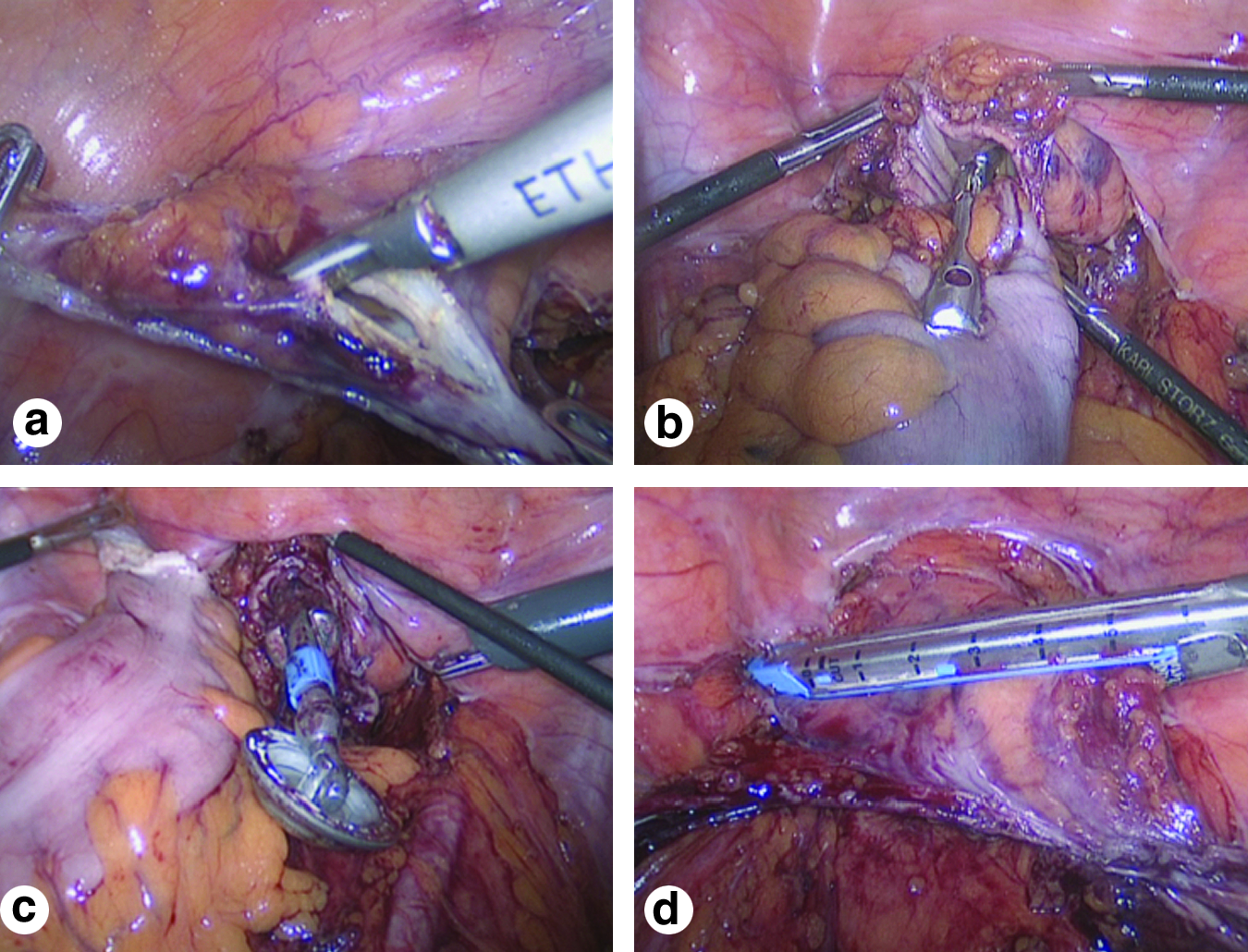
(
The next step was to open the proximal colon along the staple line. Then, the pretilted anvil was brought through the anal port into the abdominal cavity. The tip of the gastric tube was pushed through the bowel opening. A small hole was made approximately 3 cm above the bowel opening, and the gastric tube was pulled through to insert the tilt anvil. Cutting the tube and the thread allowed the anvil to untilt. The proximal bowel opening was then transected with the ENDO-GIA to close the opening (Fig. 4). The gastric tube and the small transected bowel segment were then removed through the anal port. At this point the rectal stump was closed with two firings of the ENDO-GIA. A standard double-stapled anastomosis was performed. The spike of the stapler and the tiny rectal remnant were removed in a plastic bag through the 5–12-mm trocar. Then, the anastomosis was checked by colonoscopy before the fascial layers of the 10- and 12-mm trocar sites were closed. The skin incisions were closed by intracutaneous sutures. Drains were not required.
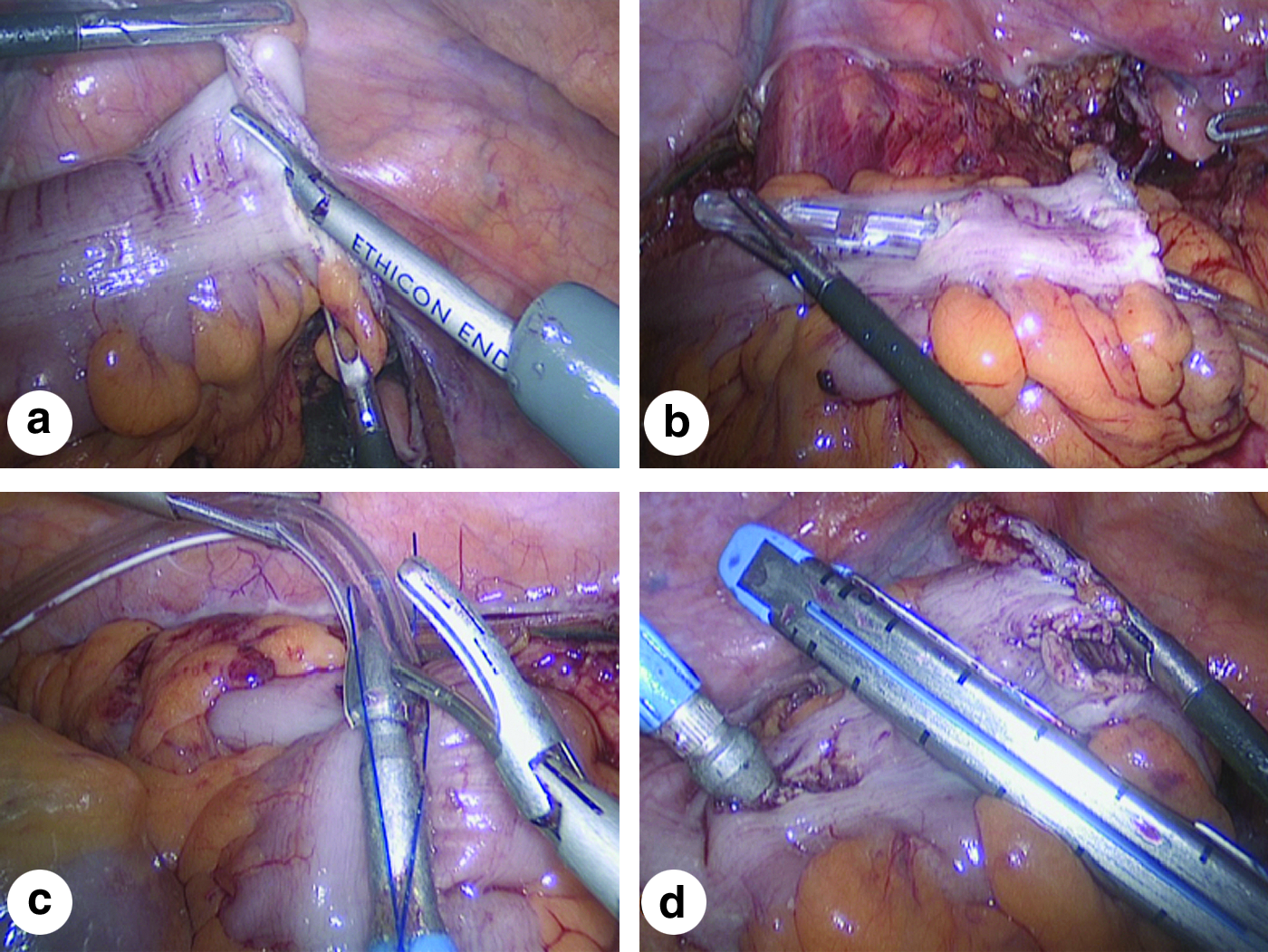
(
Results
During the operations no adverse events occurred. Operating time ranged between 95 and 180 minutes. Postoperative pain was very low and could be controlled by acetaminophen application; only 1 patient needed additional opioid analgesia. Length of the specimen ranged from 16 to 34 cm. Negative margins and adequate lymph node dissection were achieved in all malignant tumor cases. Continence and anal sphincter function were normal. Postoperative hospital days were between 4 and 8 days. Follow-up after 1 and 4 weeks showed uneventful recovery.
Discussion
Twenty years after the introduction of minimal invasive surgery, new technical innovations are emerging. Operations through natural orifices have been used in hybrid techniques like transvaginal cholecystectomy. 1 Aside from cosmetic aspect, this new approach aims to further improve postoperative recovery and quality of life.
The minilaparotomy used in the classical laparoscopic left colon or sigmoid resection can be a source of postoperative pain that counteracts the typical advantages of the minimal invasive approach. Wound complications after laparoscopic colorectal surgery are not uncommon. Infection rate at the extraction site of 10.8% and incisional hernia rates of 17.6% are reported.3–5 In the light of these arguments, avoidance of a laparotomy wound is a reasonable goal. Further, the cosmetic result after surgery is nowadays an important aspect to patients.
Our technique for laparoscopic left colon and sigmoid resection combines the classical laparoscopic dissection of the colon for either benign or malignant disease with a transanally inserted natural orifice working port. The MT was originally developed as a single-use plastic transvaginal tube to carry out laparoscopic hysterectomies. 6 Two channels allow the use of instruments for intraabdominal manipulations, while pneumoperitoneum is maintained. In our setting it can be used to remove the colon specimen and to deliver the anvil into the abdominal cavity. In this aspect it is a step forward to natural orifice surgery. Intraabdominal insertion of the anvil into the proximal colon can be cumbersome and difficult. The tilt top anvil technique reduces the transverse profile of the anvil head and makes the anvil insertion into the proximal colon quick and easy. In bariatric surgery the tilt top anvil technique has been successfully used for the laparoscopic gastric bypass procedure. 7
Clinical experience with natural orifice specimen extraction in colorectal surgery is limited to a few case reports or small series. Franklin et al. showed that the transvaginal route for specimen extraction is a way to avoid laparotomy, although it is only applicable in female patients. 8 Knol et al. used a modified proctoscope via the anus to extract the specimen after sigmoid resection for endometriosis. 9 Cheung et al. have recently described the use of an operating proctoscope to facilitate the removal of the specimen. 10 In their technique the placement of the anvil into the proximal colon is somewhat complicated compared to our technique. In their article they have limited this technique on situations with small tumors of the left colon below 4 cm. We showed that this technique can also be used in diverticular disease of the left colon, because even in the presence of peridiverticulitis and a bulky mesentery, the specimen can be separated intraabdominally to fit through the rectal stump.
Of course, this technique has limitations. Malignancies in the mid or lower rectum require total mesorectal resection where insertion of the MT would be counterproductive, although transanal specimen removal would still be possible. Anal strictures or stenosis preclude the use of the MT as well as a rectum with a small diameter. Bacterial contamination of the abdominal cavity leading to postoperative abscess formation is another concern, because the colon and rectum are intraabdominally opened. Therefore, we believe that good preoperative bowel preparation is necessary. Further, the rectal stump should be washed out before the rectum is opened. Laparoscopic bowel clamps can be used to avoid stool leakage through the opened proximal colon. For safety reasons we gave antibiotics for 5 days. So far, we have not experienced adverse effects while using these precautions.
Conclusion
Although clinical experience is still limited, the described natural orifice specimen extraction technique has the potential to further improve patient outcome after laparoscopic left colon surgery, because morbidity of the minilaparotomy can be avoided.
Footnotes
Disclosure Statement
No competing financial interests exist.