
Abstract
Abstract
Endoscopic treatment of walled-off pancreatic necrosis is becoming more prevalent in clinical practice, although perforation may complicate 5% of cases, and efficient management of this complication is imperative. In this report, we present a case of necrosis cavity perforation successfully managed by a combined laparoscopic–endoscopic approach, with a novel method of luminal defect closure.
Introduction
Case Report
A 38-year-old woman was referred for surgical management of walled-off pancreatic necrosis and a large abdominal wall hernia. Six months prior, she experienced necrotizing gallstone pancreatitis resulting in a 15-cm pancreatic fluid collection that contained solid debris (Fig. 1).
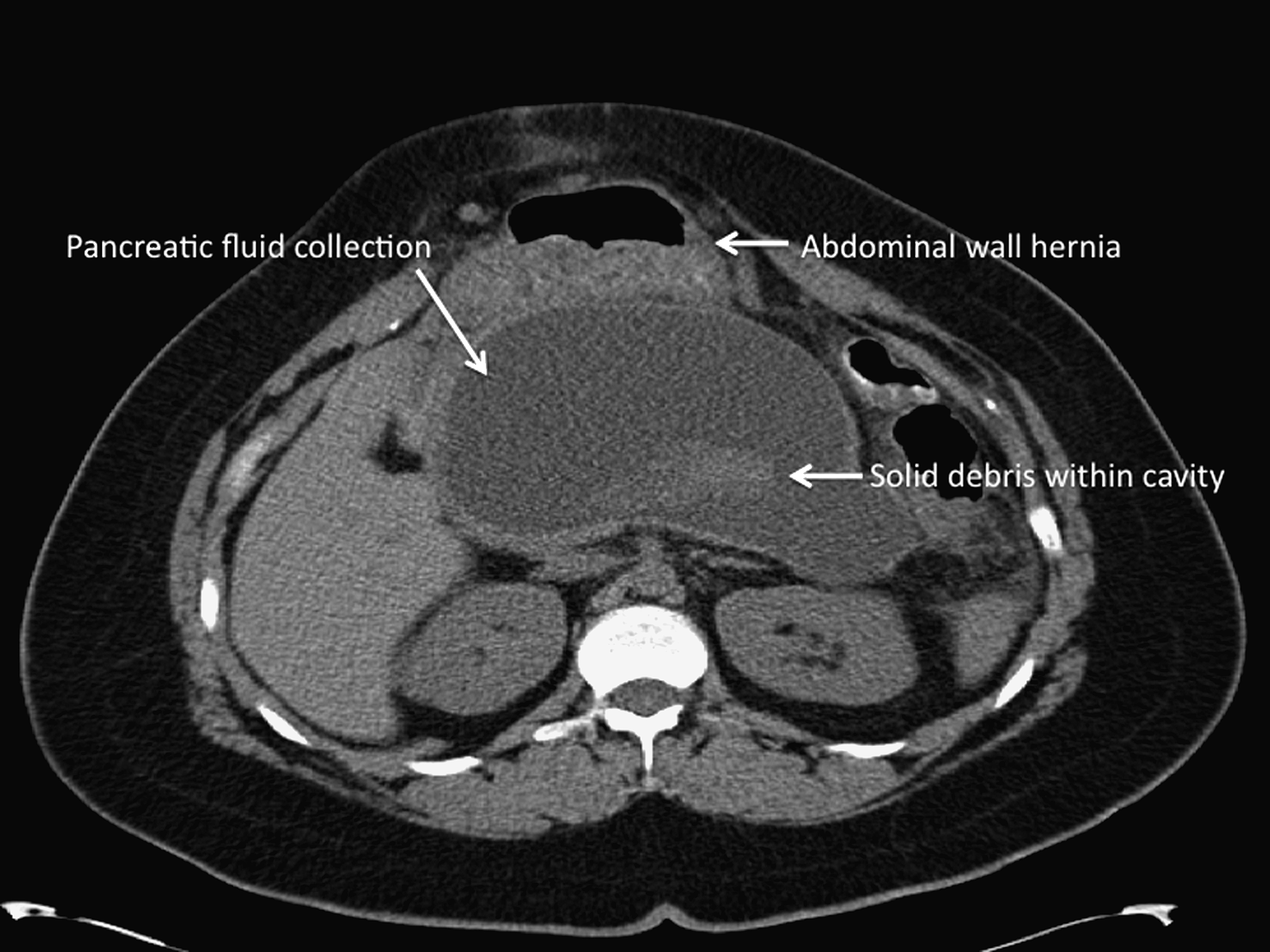
Computed tomography scan revealing a large pancreatic fluid collection containing necrotic tissue as well as a large abdominal wall hernia.
Concurrent operative necrosectomy and hernia repair would have predisposed to infection of the prosthetic mesh necessary to seal her fascial defect. She was therefore referred for an endoscopic necrosectomy before hernia repair. This procedure was performed over two sessions as previously described 3 (Fig. 2). Three double-pigtail stents were placed across the cyst-gastrostomy tract to maintain patency between sessions. After the second session, all necrotic tissue had been removed from the cavity and transgastric stents were not replaced.

Endoscopic view within the pancreatic cavity revealing the presence of necrotic tissue.
This procedure was complicated by abdominal pain and pneumoperitoneum, prompting exploratory laparoscopy. Evaluation of the upper peritoneum revealed a small amount of murky fluid, but no gross enteric contamination or unexpected bowel perforation. The upper abdomen was filled with saline, and insufflation of the stomach during concurrent gastroscopy revealed bubbling in the left upper quadrant emerging through the greater omentum above the splenic flexure, consistent with air transmitted through the lesser sac. It was concluded that the pneumoperitoneum was the result of cyst wall perforation.
The gastric defect was sealed endoscopically by placing six endoscopic clips along the periphery of the cyst-gastrostomy opening and subsequently cinching two endoloops around the clips, thereby approximating the edges of the defect (Figs. 3 and 4). This intervention resulted in cessation of air bubbling into the peritoneal cavity. Without exposing the lesser sac, a surgical drain was placed in the left upper quadrant. The abdomen was copiously irrigated and subsequently evacuated.
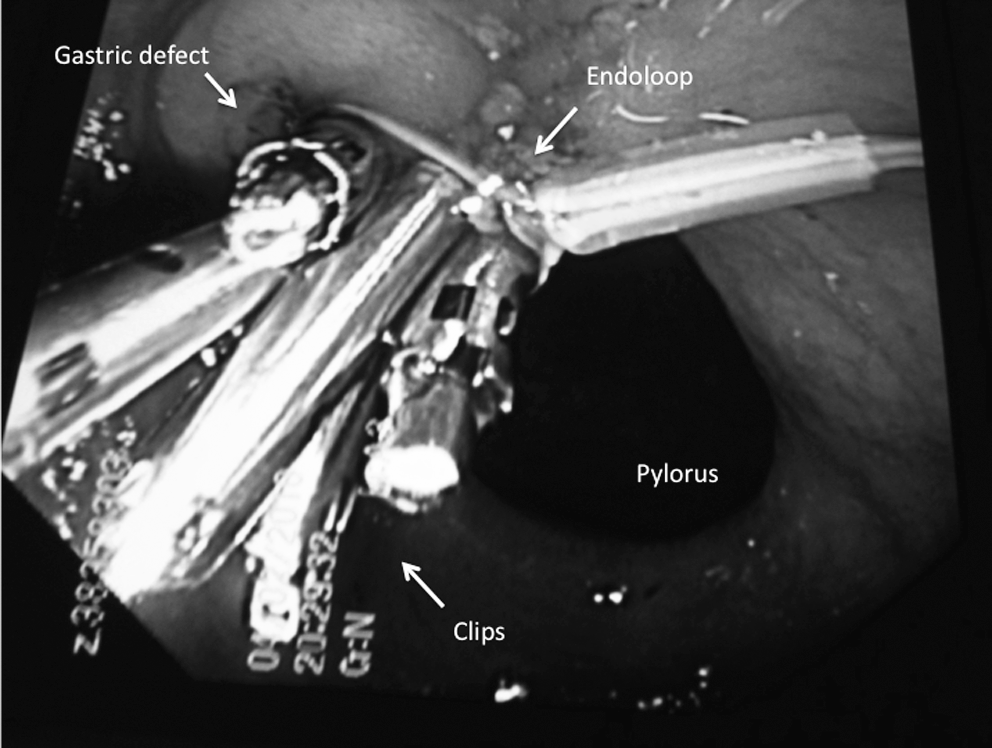
Endoscopic image showing necrosectomy tract closure by cinching an endoloop around six clips that had been deployed at the periphery of the defect.
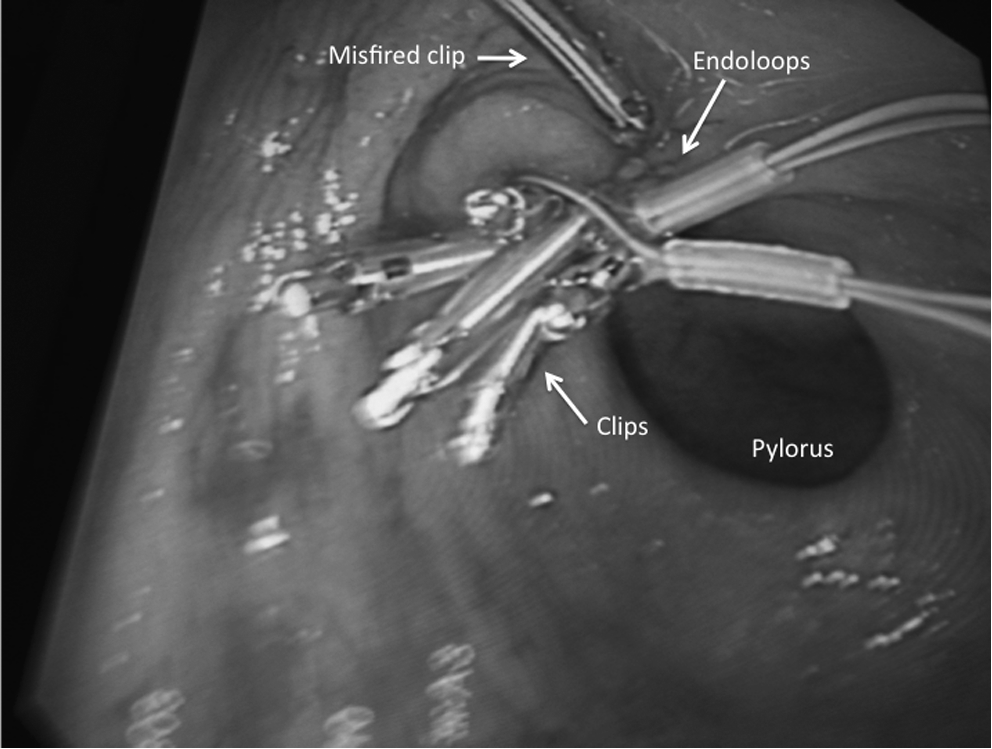
Endoscopic image revealing complete endoscopic closure of the gastric defect.
A contrast study revealed no extravasation through the closure site (Fig. 5) and the patient recovered uneventfully. The surgical drain had minimal output and was removed before discharge on postoperative day 4. A computed tomography scan 3 weeks later revealed resolution of the fluid collection. Her hernia repair is pending.
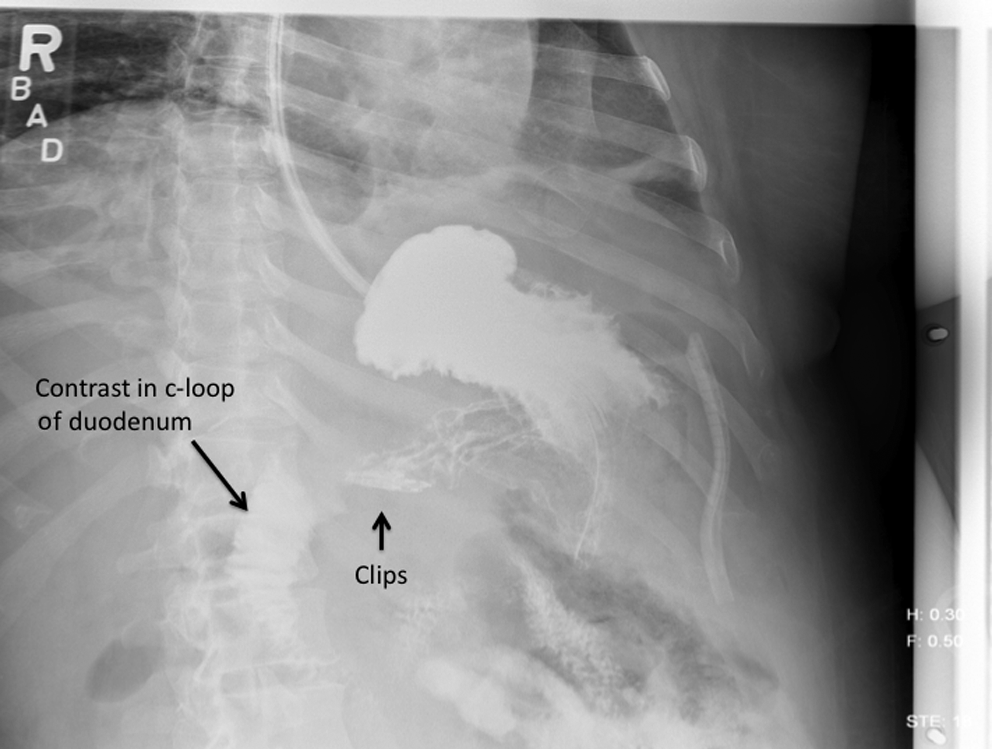
Upper gastrointestinal series revealing absence of contrast extravasation through the closure site.
Discussion
We believe that cyst perforation occurred during removal of the transgastric stents that had become adherent to the cyst wall between sessions. Even though the patient required an operation, the procedure she underwent was substantially less complex and morbid than a surgical necrosectomy. This case demonstrates two important clinical points.
First, surgical management of iatrogenic cyst perforation does not necessarily require exposure of the lesser sac and definitive management of the fluid collection in real-time, particularly if the cyst has been adequately debrided endoscopically. This type of perforation is perhaps less likely than visceral perforation to produce peritonitis and systemic inflammation if there is limited contamination of the peritoneum with pancreatic necrosis. In similar situations, initial laparoscopic assessment appears reasonable to determine the necessity of an open operation.
Second, endoscopic closure of the gastric defect at the time of laparoscopy may prevent additional contamination of the peritoneum in the early postoperative period, potentially reducing the risk of late peritonitis and shortening hospitalization. The closure technique we used is slightly different from the previously reported endoloop-clips method, which requires a dual channel scope.4,5 Our technique may be useful in closing large perforations not amenable to clipping alone, without exchanging for a therapeutic scope.
Footnotes
Disclosure Statement
No competing financial interests exist.