
Abstract
Abstract
Laparoscopic repair of ventral or incisional hernia is among the most commonly performed minimally invasive procedures. Different modes of recurrence have been reported in literature, including missed defects, mesh migration, mesh infection, etc. Transfascial suture fixation in addition to tackers is an established method to prevent recurrence due to mesh migration. We report possibly the third case of recurrent ventral hernia with multiple defects at transfascial suture sites of previous laparoscopic ventral hernia mesh repair. The patient was treated by laparoscopy with a large intraperitoneal PROCEED mesh, covering the new hernia defects and older mesh.
Introduction
Case Report
A 49-year-old female patient presented with lower abdomen swelling since 7 months, with a history of laparoscopic umbilical hernia repair performed 18 months back. Clinically there was a reducible swelling in the suprapubic region, with positive cough impulse. Abdominal ultrasonography revealed a 2.7-cm defect in the anterior abdominal wall in the suprapubic region, with herniation of bowel loops through it. Previous operative record revealed placement of a Gore Tex mesh of size 15 × 10 cm. Mesh fixation was performed with multiple transfascial fixation sutures at its borders and at center.
Endoscopic view after adhesinolysis revealed multiple hernial defects near the inferior border of mesh at the sites of transfascial fixation sutures (Fig. 1). Three defects varying in size from 5 × 7 mm to 2.7 × 1.5 cm was noted, showing transfixation sutures passing through the cranial border of the defects.
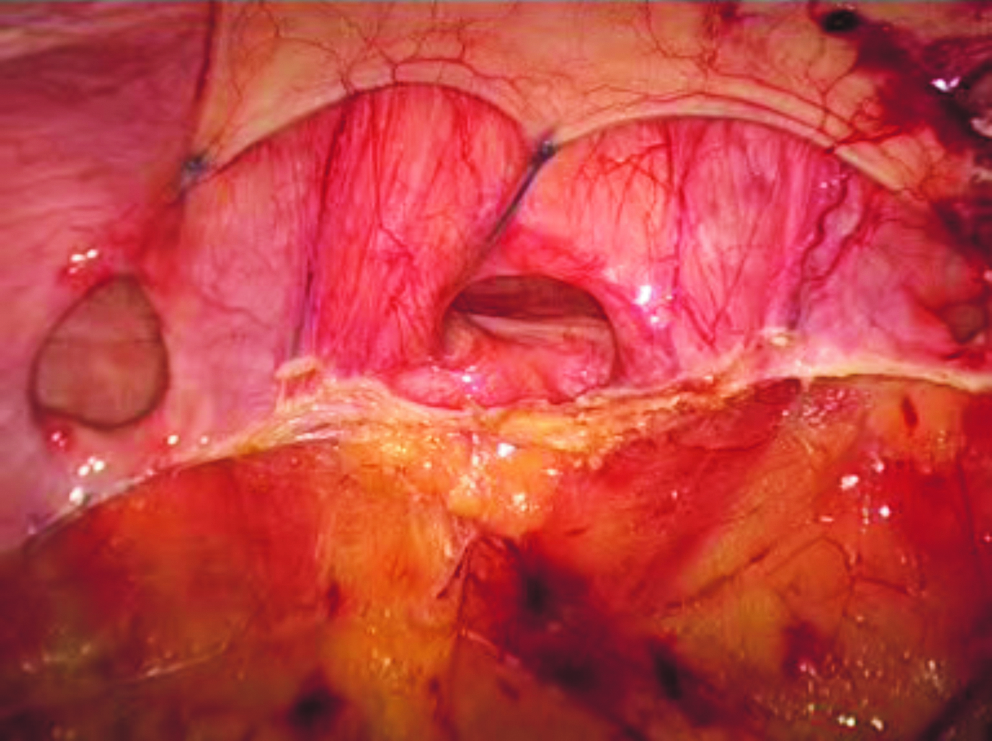
Laparoscopic view after adhesinolysis depicting multiple hernial defects. Transfascial sutures at the caudal borders of the mesh are seen passing through the cranial border of the defects.
After adhesinolysis, laparoscopic repair was performed using a PROCEED mesh, covering the previous mesh and hernial defects with sufficient overlap of recurrent hernial sites. Fixation was performed using only spiral tackers in double crowning configuration.
Postoperative period was uneventful and the patient was discharged on first postoperative day. After 3-month follow-up, clinical examination was normal.
Discussion
A tension-free repair with adequate overlap of fascia with mesh comprises the basic tenet of a successful hernia repair. In last few years, laparoscopic ventral or incisional hernia repair has become the surgery of choice with advantages of lower complication rate, shorter operative time, shorter hospital stay, lower recurrence rate, and lower postoperative abdominal pain due to ease of intraabdominal adhesinolysis. To accomplish tension-free repair to reduce recurrence rates, use of prosthetic material has been recommended for the repair of incisional or ventral hernia larger than 4 cm. 1 Overlap of mesh over the hernia defect of at least 3 cm is considered essential.2,4–6 Fixation of mesh to anterior abdominal wall is mandatory to keep sufficient overlap and avoid recurrences by mesh migration.
Several mechanisms of recurrence after ventral hernia have been reported. 3 Recurrence of abdominal hernia after mesh repair can be caused by a missed hernia or insufficient overlap of the defect by mesh.
The ideal method of fixation of the prosthesis to the abdominal wall remains a controversial issue. Heniford et al. 2 stated that suture fixation of the mesh is mandatory in laparoscopic ventral hernia repair to avoid higher recurrence rates. Leblanc et al. 4 also emphasized the use of transfascial sutures for effective fixation of the prosthetic biomaterial.
On the contrary, Carbajo et al. 5 reported lower surgical time, less incidence of parietal visceral injuries, and less postoperative pain with similar recurrence rate in total intraperitoneal mesh fixation using double crown of tackers only.
Absorbable tackers and fibrin sealant alone as a method of fixation remains investigational for laparoscopic incisional ventral hernia repair.
Recurrence of abdominal hernia after any repair can be caused by a hernia that was missed at the previous surgery. If the implanted mesh does not cover all the abdominal wall defects, a missed hernia outside the area covered by the mesh can progress to become clinically apparent, thus presenting as a recurrent hernia.
Therefore, many authors propose covering the whole primary incision of a patient presenting with an incisional hernia. 7 Adequate exploration of the whole incision is often mentioned as an advantage of the laparoscopic technique. One of the adverse effects of laparoscopic hernia repair is that the technique used can cause a new hernia of the abdominal wall. Trocar site hernias are sometimes present and might need repair. Approximating the fascia using sutures at all trocar sites larger than 5 mm avoids trocar site hernia.
“Tacker hernia” has also been reported as a cause of recurrent abdominal wall hernias after laparoscopic repair of ventral hernias. 8
Transfascial sutures as the cause of recurrent hernia after laparoscopic ventral hernia repair have been reported in 2 patients. 9 Our case is possibly the third case of this type of recurrence and the first after the laparoscopic incisional ventral hernia repair. Whether this is caused by using too much tension on the sutures or by an improper tissue healing mechanism in these patients is not clear.
One way to avoid this complication of “suture hernia” would be to avoid using these sutures for fixation of the mesh. Some experimental data question the need for the use of transfascial sutures, compared with a tackers-only technique. 10 Sutures can be avoided by using the “double crown” technique as proposed by Carbajo et al. 5 In this technique, no transfascial sutures are used, and the mesh is fixed by two rows of spiral tackers. Whether this technique can be performed without compromising the recurrence rates is not clear. 11
This does not eliminate the risk of the previously described “tack hernia.” 8
Maybe avoiding tightening the sutures too forcefully and covering the suture entry points with mesh during placement can lower the risk for a “suture hernia.”
Transfascial sutures for fixation of mesh have been used in traditional open techniques for ventral or incisional hernia repair. But, only laparoscopic approach allows the identification of this type of recurrence.
Conclusion
Transfascial suture hernia is a very rare cause of recurrent hernia after laparoscopic ventral hernia repair. The identification of this new entity as a cause of recurrence further raises the issue of ideal method for fixation of mesh to prevent its migration during laparoscopic ventral hernia repair. At present, we believe that combined suture and tacker fixation is best, provided sutures are applied with no tension and suture entry points are covered by mesh.
Footnotes
Disclosure Statement
No competing financial interests exist.