
Abstract
Abstract
Background:
Recent reports on laparoscopic surgery for urachal anomalies have not described any techniques to restore the natural appearance of the umbilicus. In this report, we present a simple technique that enables complete resection of urachal anomalies while preserving the natural appearance of the umbilicus.
Materials and Methods:
Laparoscopic excision of symptomatic urachal anomalies was performed for 4 men and 2 women. After dissecting the urachal lesion along the preperitoneal plane toward the umbilicus, the cephalic side of the lesion was ligated and the skin at the base of the umbilicus was divided while compressing the anterior abdominal wall to ensure complete removal of the lesion.
Results:
The laparoscopic procedure was successfully completed with minimal blood loss, and the umbilicus could be restored to its natural appearance in all the cases.
Conclusions:
This is the first report to describe a procedure for restoring the natural appearance of the umbilicus. This simple, alternative approach yields better cosmetic results and, therefore, will be useful, especially in younger patients.
Introduction
Several recent reports on laparoscopic excision of urachal anomalies have stated the association of laparoscopic surgery with less postoperative pain and a shorter convalescence period.5–7 Many authors recommend an infraumbilical incision for the complete excision of the urachal tissue. However, an incision along the umbilical ring (∼3 cm) 5 and excision of the urachal anomaly through this incision leaves an obvious postoperative scar or an umbilical deformity. Further, residual urachal tissue, if any, can cause recurrence of the lesion. 8 Cutting et al. reported a case of persistent postoperative umbilical discharge, observed during the follow-up period, that required open exploration of the umbilicus and removal of the residual urachal tissue; in this case, since the subcutaneous part of the urachus, just below the umbilicus, was particularly difficult to be excised, it was not resected during the laparoscopic excision. In our opinion, the principle of surgery for excision of an inflammatory mass must be en bloc removal of the lesion without dissemination of its contents; however, this principle cannot be overemphasized.
Another aspect worth considering is that most urachal anomalies observed in young patients are benign; therefore, the cosmetic outcome of surgery is very important to these patients and their parents. In this report, we describe our experience of laparoscopic excision of urachal anomalies and describe a new approach to restore the natural appearance of the umbilicus; we avoided periumbilical incisions and yet successfully achieved complete removal of the urachal tissue, including the subcutaneous part of the urachus.
Materials and Methods
Patient demographics
Between August 2003 and March 2010, 4 men and 2 women (age range 16–37 years) with symptomatic urachal anomalies underwent laparoscopic excision (Table 1). Patient charts were retrospectively reviewed. All the patients had symptomatic urachal anomalies for years before the surgery. Two patients had undergone drainage of the abscess cavity before the laparoscopic excision. Preoperative diagnosis of the urachal anomalies was established in all the patients using a combination of abdominal ultrasonography, magnetic resonance imaging, and computed tomography findings.
PMP, pseudomyxoma peritonei.
Surgical procedure
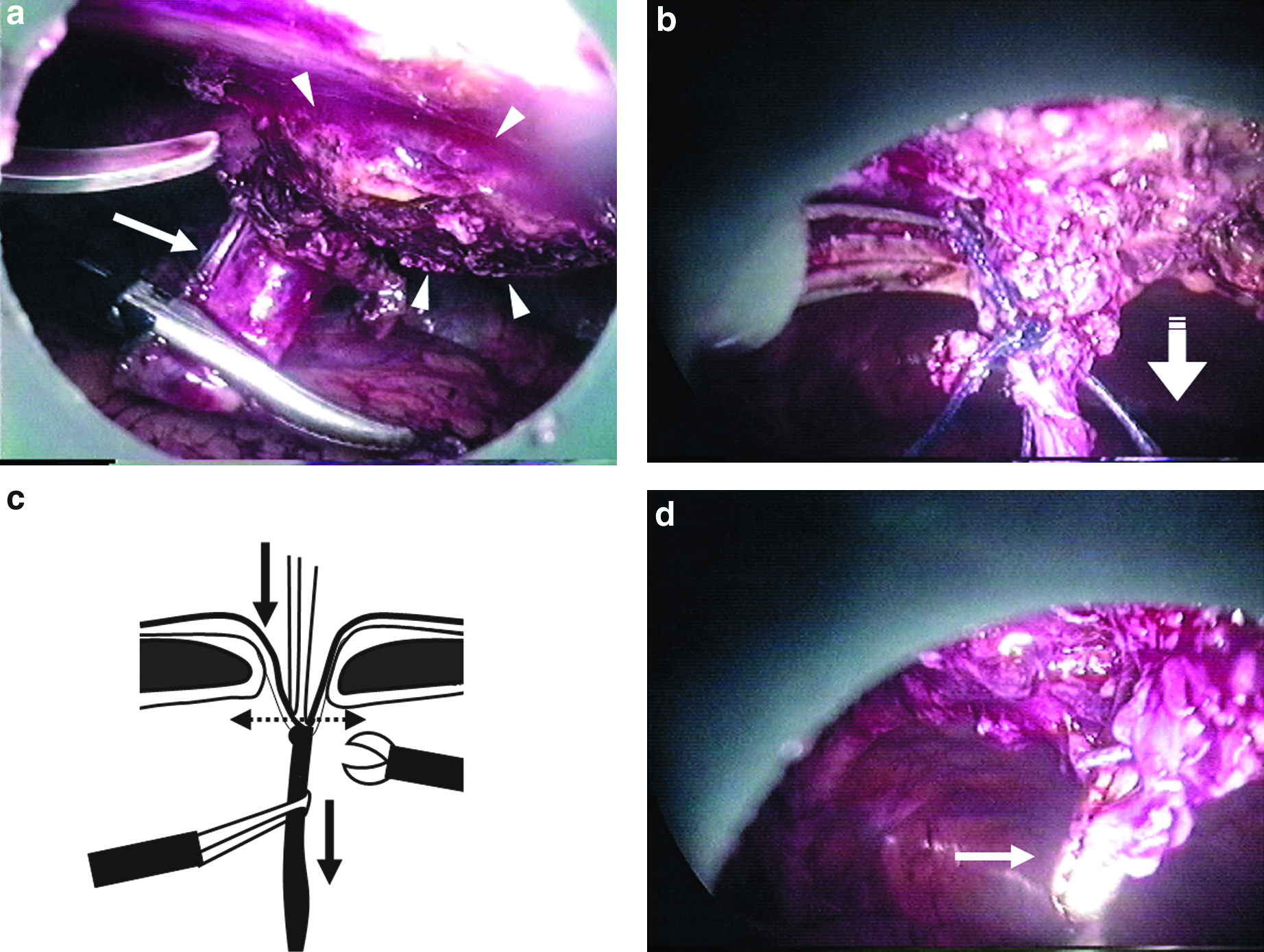
After the induction of general anesthesia, each patient was placed in the supine position, and three trocars were inserted into the peritoneal cavity (Fig. 1). In all the patients, on inspection of the abdominal cavity, the omentum was found tightly adhered to the peritoneum around the umbilicus. The adhering part of the omentum was dissected with laparoscopic scissors. Adhesiolysis allowed an excellent panoramic view of the whole lesion and, therefore, the extent of each infection could be appropriately assessed. Both the umbilical arteries were clipped and divided. The medial umbilical ligament was dissected from the anterior abdominal wall. At this point, physiological saline was infused into the bladder, and the medial umbilical ligament was ligated and resected across the dome of the bladder. Dissection around the abscess was then resumed (Fig. 2a). The lesion was dissected from the anterior abdominal wall along the preperitoneal plane toward the umbilicus. At the umbilical base, the fascial layer around the medial umbilical ligament was circumferentially cut with laparoscopic scissors. In some cases, dissection was performed using an Endoshear roticulator (Roticulator Endo Mini-Shears; Autosuture), to obtain the necessary operative angle. The umbilical base was pushed toward the peritoneal cavity by compression of the anterior abdominal wall. The cephalic side of the lesion was pulled down with laparoscopic forceps and ligated with an endoloop (Fig. 2b). The skin at the base of the umbilicus was sharply cut with laparoscopic scissors (Fig. 2c), thus reducing the skin defect to the size of a pinhole (Fig. 2d). The entire specimen was extracted from the peritoneal cavity through the 12-mm trocar site. After the operation, the skin defect receded into the umbilicus and was hardly visible.

Port placement. Three trocars were inserted into the peritoneal cavity. The first 12-mm trocar () was placed at a distance of three fingers above the umbilicus in the left pararectal area. The other two ports (•) were placed lateral to the left rectus muscle. In case 5, an additional 5-mm working port (▴) was placed lateral to the left rectus muscle to reconstruct the bladder cuff.
Talking about specific cases, case 2 was incidentally diagnosed as an urachal mucinous tumor associated with pseudomyxoma peritonei. The entire area of the peritoneum covered by a gelatinous material was resected, a pool of yellowish mucoid material was aspirated, and then, the operated area was thoroughly irrigated with physiological saline using a laparoscopic suction cannula.
Case 5 was diagnosed as an infected urachal cyst situated close to the bladder dome. The junction of the medial umbilical ligament and the bladder dome was determined, and the dome portion of the bladder was circumferentially resected (Fig. 2e). The bladder was reconstructed using two-layered freehand intracorporeal suturing and then filled with physiological saline to identify points of leakage, if any.
Results
The urachal lesions were successfully resected using our laparoscopic approach in all cases. The mean operative time was 182 minutes (range 108–381 minutes), and the blood loss was minimum. The postoperative course was uneventful, except in case 5, in which postoperative paralytic ileus developed on postoperative day 8; the condition, however, resolved without any surgical intervention. The umbilicus was restored to its natural appearance (Fig. 3). Pathological examination of the specimens confirmed benign urachal anomalies in 5 patients and a mucinous borderline tumor with low malignant potential in 1 patient. The mean follow-up time was 33.6 months (range 4–59 months). All the patients are currently asymptomatic without any local signs of recurrence.

Postoperative appearance of the umbilicus.
Discussion
Laparoscopic excision of urachal anomalies minimizes surgical morbidity and achieves the same surgical outcome as the open procedure. Observation through the laparoscope offers an excellent panoramic view of the whole lesion, thereby enabling appropriate assessment of the extent of infection. 9 In addition, since the urachus is not close to any vital organ or major vessel, laparoscopy is considered an easy and safe method to mobilize all the urachal remnants up to the umbilicus. Further, this approach is designed to restore the natural appearance of the umbilicus. Since most urachal anomalies in young patients are benign, the cosmetic outcome is very important to these patients and their parents. 10
In this report, we described a simple approach to restore the natural appearance of the umbilicus in cases of urachal lesions. Ligation of the cephalic side of the lesion and division of the skin at the base of the umbilicus along with compression of the anterior abdominal wall ensures complete removal of the lesion. The tissue at the base of the umbilicus is a thin and relatively weak structure. In addition, the abdominal muscle layers are absent at this site. Therefore, dissection of the medial umbilical ligament around the umbilical base is not difficult.
This technique does not involve manipulation of the umbilicus; therefore, the natural appearance is preserved despite the postoperative scars. In cases of umbilical inflammation, initial surgical drainage and antibiotic treatment of the infection are required; such cases are managed by extraperitoneal drainage of the abscess followed by further excision of the urachal anomaly; and thus, complete resection of the umbilicus by neo-umbilicoplasty is avoided. The umbilicus is an important aesthetic component of the abdomen; therefore, surgeons should maximize the use of laparoscopy to excise urachal anomalies and, consequently, preserve the natural appearance of the umbilicus.
To the best of our knowledge, this is the first report that describes a procedure to restore the natural appearance of the umbilicus during laparoscopic resection of an urachal lesion. This simple, alternative approach enables complete resection of the entire urachal tissue while restoring the natural appearance of the umbilicus. Thus, it is thought to be a promising intervention, especially in younger patients.
Footnotes
Disclosure Statement
No competing financial interests exist.