
Abstract
Abstract
Objectives:
The objective of this study was to describe a simple modification of the laparoscopic pelvic lymphocele marsupialization (LL) following radical prostatectomy lymphoceles (RP-LC).
Patients and Methods:
Forty-eight patients (57–76 years) with symptomatic RP-LC underwent surgery in our institute. This was through an open approach in 6 (open drainage [OL]) and LL in rest of the patients (12 with 3 [LL3] and 30 with 2 [LL2] trocars). All except 2 patients were refractory to percutaneous tube drainage and/or sclerotherapy. Pelvic ultrasound and/or computed tomography scans revealed LC size (4 × 5–11 × 12 cm) and volumes (100–1100 mL).
Results:
All surgeries were uneventful with an operative time of 15–60 minutes for LL and 35–90 minutes for OL and it became shorter with increasing experience with LL2 (15–25 minutes). Mean hospitalization time was 2.3 and 8 days after LL (LL2 and LL3) and OL, respectively. LC were at the right side in 10 patients, at the left side in 6, and at both sides in 14. Postoperative ultrasound revealed primary success in all cases. No patient developed recurrence of or had treatment for lymphocele during a mean follow-up time of 19 months.
Conclusion:
LL2 is a simple, feasible, and safe procedure that could be used as a first-line treatment for large, noninfected symptomatic or refractive RP-LC.
Introduction
Clinically relevant pelvic LC require adequate intervention to avoid complications. Treatment options depend on factors such as size, position, infection risk, loculations, and recurrence. These include percutaneous aspiration, 2 with or without sclerotherapy, percutaneous catheter drainage, 3 or laparoscopic4,5 or open surgical drainage. 6
A laparoscopic procedure achieving transperitoneal drainage of postretropubic radical prostatectomy lymphoceles (RP-LC) has been already described.7–10 This allows the same indications and surgical principles as the conventional open drainage (OL).
The aim of the present study was to describe a simple modification of the laparoscopic marsupialization of RP-LC. To our knowledge, this one-working-trocar technique has not been previously described.
Patients and Methods
Between January 2000 and August 2008, 48 patients aged 57–76 years (mean: 65.3 years) underwent LC marsupialization in our institute. Six patients had OL and the rest had laparoscopic. After our experience with the standard three-trocar technique of LC marsupialization in 12 cases (LL3), we have modified the technique using only two trocars (LL2). All patients had large symptomatic RP-LC and were refractory to percutaneous tube drainage with/without sclerotherapy. Presenting symptoms were pelvic fullness and lower abdominal pain (9 patients), lower limb edema (3), which was caused by deep venous thrombosis (DVT) in 1, urinary frequency (2), and progressive deterioration of continence (3) and were accidentally discovered in 4 patients. Ten patients had infection necessitating preoperative antibiotic therapy according to culture and sensitivity tests. All patients were evaluated clinically, with abdominopelvic ultrasound (US) (Fig. 1) and/or computed tomography scans (Fig. 2). There were no contraindications for general anesthesia.

Ultrasound examination showing a lymphocele with a diameter of >5 cm.

Computed tomography scan of a patient with a large lymphocele in the left pelvic region (diameter: >5 cm) following radical prostatectomy. White arrows show the extension of the lymphocele. Black arrows show a partial compression of the common iliac vein.
Surgical technique
LL is our standard approach for RP-LC. A single-dose first-generation cephalosporin is administered preoperatively (for 3 days if infected). A 10-mm camera port is placed through a minilaparotomy at the umbilicus and the abdomen is insufflated with carbon dioxide. The abdomen is explored laparoscopically. The inguinal rings and gonadal vessels on both sides were visualized along with the patients' gallbladder, liver, stomach, colon, and appendix. One additional 5-mm port is then placed under vision in the scar of operation drain (Fig. 3), through which grasping forceps, Sonosurge, and scissor were used alternatively to make an ∼6-cm window in the peritoneum overlying LC (Fig. 4). Intestinal adhesions especially on the left side were cut first. An important landmark is the vas deferens to avoid injury of iliac vessels. Trendelenburg position allowed the intestine to fall down from field. There was no need to refill or mark LC (e.g., methylene blue solution or intraoperative US). The laparoscope was then placed within the LC cavity, the iliac vessels were visualized, and septations—if found—were disrupted (Fig. 5), followed by cauterization of incision edges and removal of internal membranes with resection or suction. The operative ports were then removed under direct visualization, followed by closure of stab wounds.
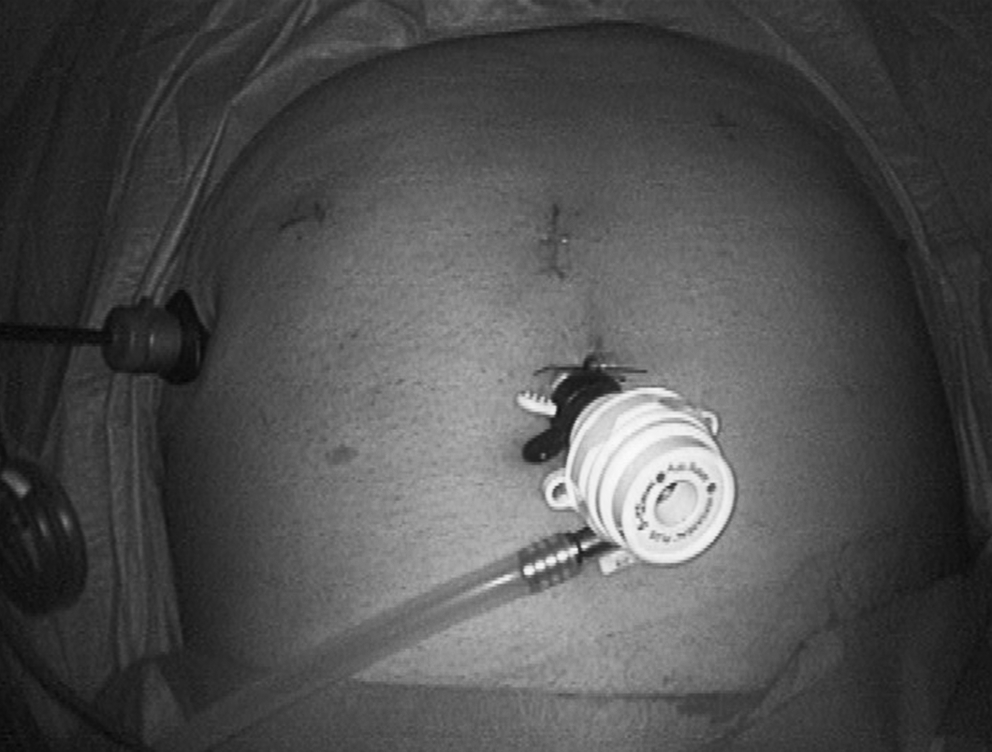
Trocars position in a patient with lymphocele at 2 weeks after nerve-sparing endoscopic extraperitoneal radical prostatectomy.
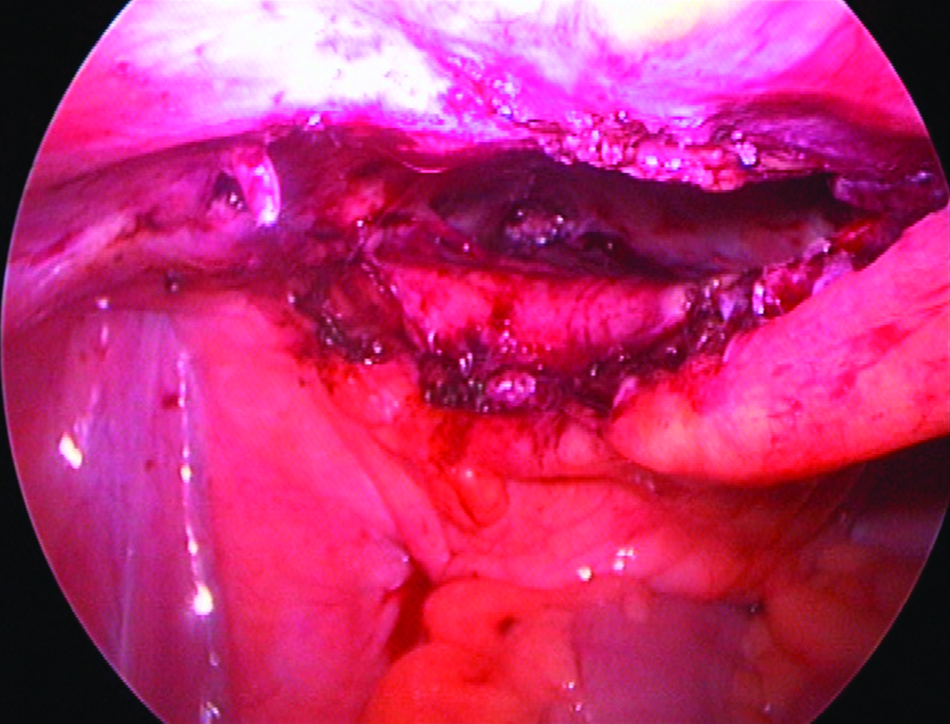
Ellipsoid incision of a lymphocele.
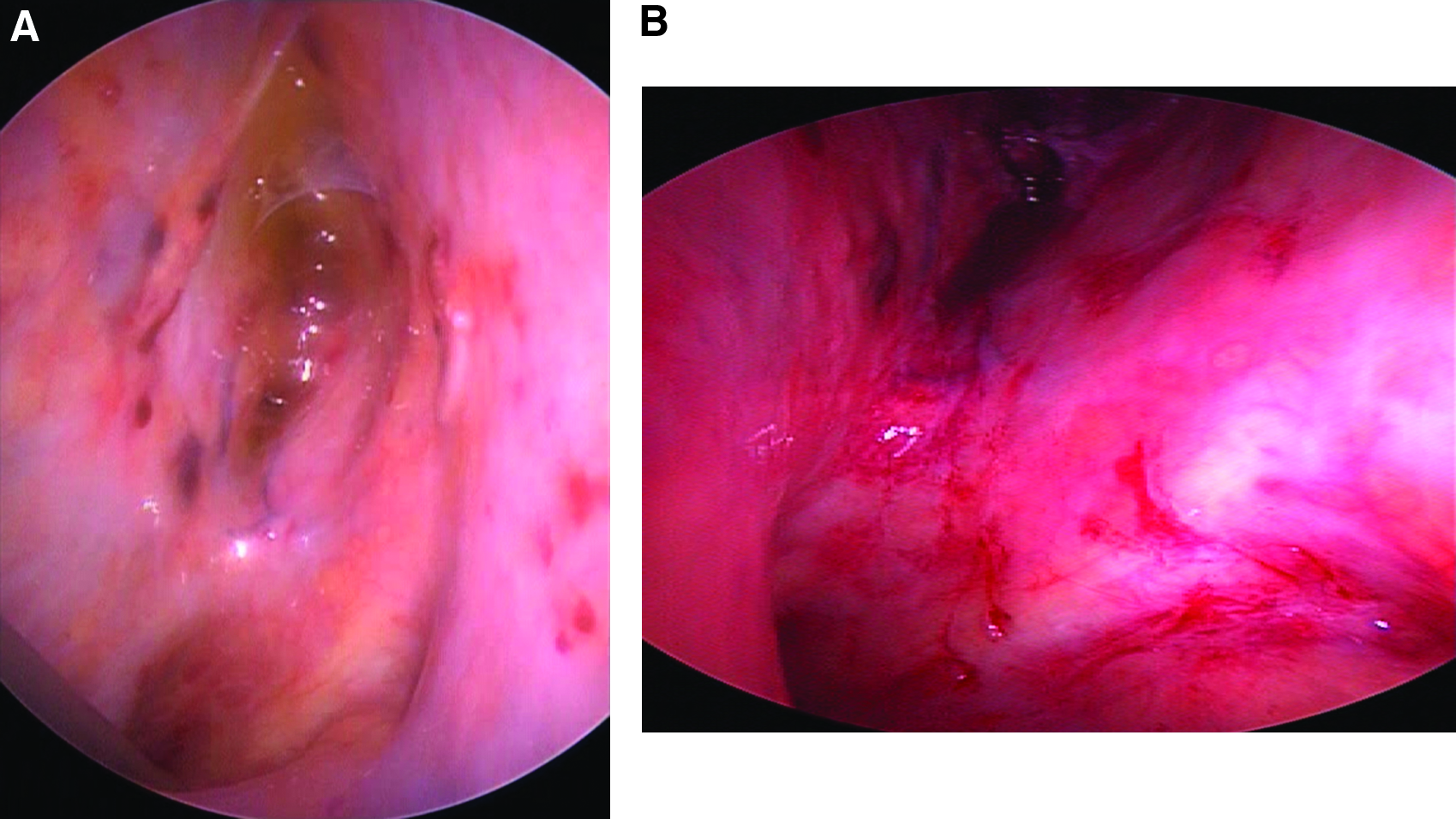
Internal view of a multilocular lymphocele:
Results
Indications for surgery
LCs or its symptoms were refractory in all cases. Presenting clinical symptoms have been mentioned earlier. Sclerotherapy was done in 15 patients with aminoglycoside (tobramycin) local irrigation at 6–21 days before procedure. Laparoscopy followed as the standard intervention; open surgery was only indicated in patients with previous multiple abdominal surgeries and deep small LC where laparoscopy is relatively contraindicated. We resort to laparoscopy as the first-line treatment in 2 cases, huge lymphocele in 1 patient (1100 mL) and rapidly accumulating in the other (1 week postoperatively).
Operative results
In all except 3 patients, the initial treatment included percutaneous diagnostic aspiration and insertion of an 11F nephrostomy tube under US guidance. The time between lymphadenectomy and catheter drainage was 12–188 days. LC size ranged from 4 × 5 to 11 × 12 cm with fluid volumes of 100–1100 mL. Lymphorrhea persisted in all patients with drainage volumes of ≥100 mL/day for at least 1 week (range: 7–21 days). Thus, a peritoneal drainage was planned.
Both OL and LL were uneventful with an operative time of 35–90 and 15–60 minutes, respectively, and negligible blood loss. With increasing laparoscopic experience, we have modified the technique as mentioned earlier. The operative time became progressively shorter (∼15 minutes for one side and 25 minutes for both sides) for the whole procedure. This was at the right side in 10 patients, at the left side in 6, and at both sides in 14. There were no conversions or perioperative complications. The tube drainage was removed under vision intraoperatively.
Postoperative results
Oral intake and ambulation after LL started at same day as soon as the patient can. Postoperative regular analgesics was necessary only after OL, whereas it was administered on need in only 5 LL patients. The average scar length was 8, 4, and 3 cm for OL, LL3, and LL2, respectively. Antibiotic therapy, when indicated, was stopped before the patient left hospital (average: 2 days). Patients were discharged at 8 days (after OL) and 2–4 days (mean: 2.3 days) after LL. Postoperative abdominal US revealed primary success in all cases. The patients have done well in early postoperative period, with disappearance of presenting symptoms and normalization of laboratory findings. No abdominal or intestinal problems, infection, or recurrence was encountered.
Follow-up
None of our patients developed recurrence of or had treatment for RP-LC during a follow-up period of 2–24 months (mean: 19 months). Regular abdominal US examinations revealed no evidence of LC recurrences even subclinically.
Discussion
LC were first described by Mori after gynecological tumor operations. 11 As the peritoneal surface is absorptive, LC occurs rarely following intraperitoneal operations 12 and its therapy could be in establishing a connection to the peritoneal cavity. Small portion of RP-LC requires intervention necessitating high clinical suspicion to detect and properly treat symptomatic LC.12,13 US is a sensitive diagnostic method for detecting intraabdominal fluid collections including LC. 14 This diagnosis could be confirmed by computed tomography scan or puncture to rule out other fluid collections (hematoma, urinoma, or pus).
Lymphoceles could have serious sequelae such as secondary infection, thromboembolic events, DVT, and pulmonary embolism. 15 Further, 50% of all reinterventions after RP were for LC management. 16 Available managements include single or recurrent percutaneous aspiration 17 or drainage, 18 sclerotherapy, 17 OL, and LL. OL gives >90% success after peritoneal marsupialization. 18 Disadvantages include general anesthetic, longer hospitalization, and surgical trauma. 19 In the other hand, percutaneous lymphocele drainage is protracted and associated with high recurrence (25%) and infection (50%) rates. Therefore, early LL for patients with sterile symptomatic LC is recommended. LL3 is accepted as a standard laparoscopic procedure.7–10,20
Varga et al. 10 reported the technique in 13 patients after methylene blue injection. Operative time was 25–70 minutes (2 were both sides). The tubes were removed at 1st or 2nd postoperative day. Mean hospitalization time was 3 days, which is longer than ours. Otherwise, rest of the parameters were comparable, favoring our modification.
In comparison to our initial LL3 experience, the new modification is accompanied with same postoperative analgesics, shorter operative time, and hospitalization. The latter two points could be also in part due to our laparoscopic experience. Some surgeons deny the cosmetic advantage of the technique as these patients had already laparoscopic or open scars which could all be used. In our opinion, this is not true in terms of postoperative analgesics and patients' preference. Further, why more, if a one-port procedure is feasible?
Some surgeons emphasize the use of a nephroscope through a 10-mm trocar, where the inbuilt channel enables doing small incisions. We believe that both procedure safety and the ability to perform ellipsoid incision are compromised.
LL2 is not just a personal achievement or a technique that could be done. It is an addition to the current minimally invasive surgery armamentarium. Using the existing scar of the drain and an umbilical scar made the technique scarless adding more to the laparoscopic minimal invasiveness. The short operative time (about 20 minutes), less pain, and less morbidity provide better results comparable with other managements—such as puncture or OL—especially in terms of procedure simplicity, treatment period, and infection rates. Additionally, using a single port has neither added difficulties to the procedure nor affected its safety.
Generally, there are precautions to avoid complications, especially with the use of LL2. Trendelenburg position is mandatory. LC must be identified with certainty (ballooning, soft consistency, and transparency; otherwise, laparoscopic needle aspiration or methylene blue injection). Urinary bladder should be kept empty. Excision of wide ellipse beginning from lateral to medial alleviates the need for second instrument to support the flap and avoids vascular, ureteric, or urinary bladder injuries. Then, inspection of the LC cavity and division of septae should always follow. This ensures adequate drainage and prevents recurrence.
LL may not be feasible in small, deep, or extremely lateral symptomatic LC, which are difficult to distinguish from iliac vessels or those with extensive adhesions or bowel interposition. The standard LL3 seems not to add any advantage over our modification in this matter.
Conclusion
The one-working-trocar laparoscopic drainage is a simple, feasible, and safe procedure that could be used as a first-line treatment for large, noninfected symptomatic or refractive RP-LC by laparoscopists.
Disclosure Statement
No competing financial interests exist.