
Abstract
Abstract
The rarest form of congenital diaphragmatic hernia involves a central tendon defect, which is often associated with a massive pericardial effusion. Very few of these have been reported, and they present unique challenges to the pediatric surgeon. We present a case report of our recent experience of this condition in a term neonate and the difficulties in diagnosing the condition. We also detail the first use of laparoscopy to close such a defect.
Introduction
Case Report
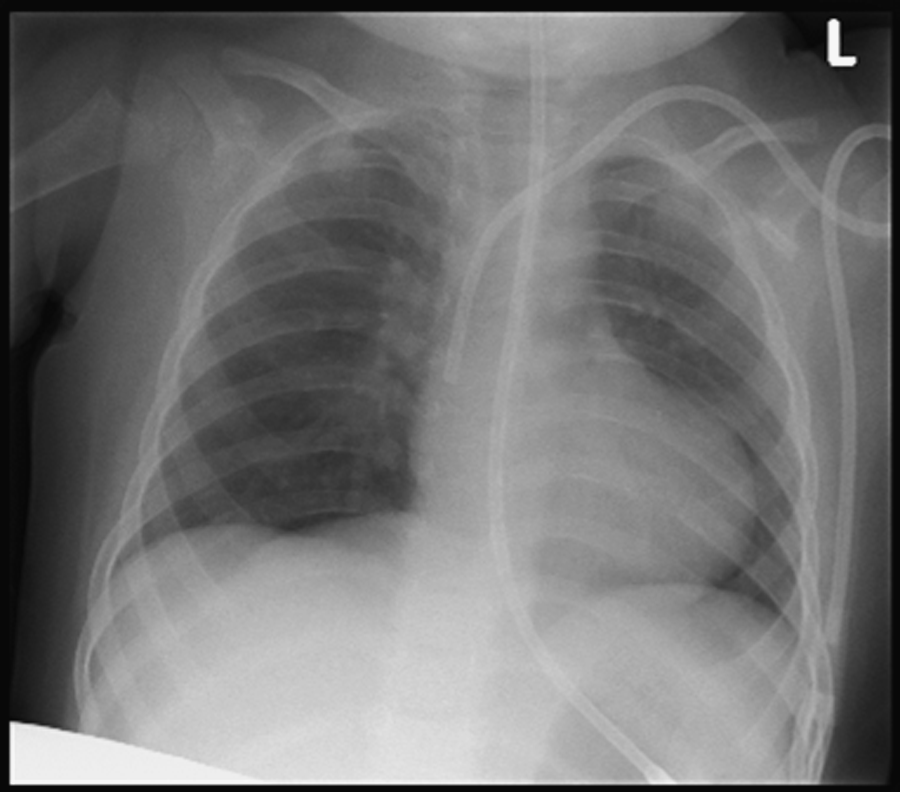
Our patient was a female infant born at term by spontaneous vertex delivery, weighing 3.52 kg. The mother had had a normal 12-week antenatal scan and the neonate initially appeared well. However, over the first few hours of life, she developed increasing respiratory distress and was therefore intubated. A chest radiograph at this time showed an almost complete whiteout of both lung fields (Fig. 1). Surfactant was given and the baby was transferred to a tertiary neonatal unit. Further investigations over the next few days raised the question of a diaphragmatic defect with extremely hypoplastic lungs, a right pleural effusion, and pericardial cyst. Surgical advice was sought, and on day 5 of life, the neonate was transferred to the pediatric surgical unit for further assessment.
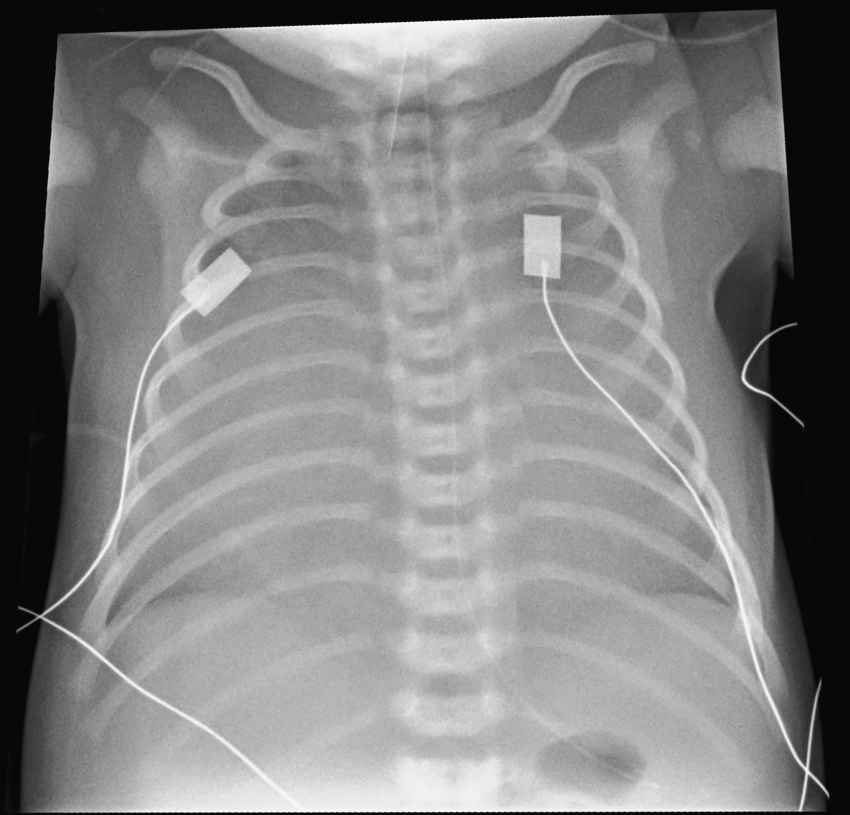
Chest radiograph showing complete opacity of both lung fields.
On arrival in our center, and in view of the bilateral chest opacities, an echocardiogram was performed and this revealed a massive pericardial effusion and a structurally normal heart—subsequent ultrasonography in the hands of a pediatric radiologist showed the liver to be lying in the chest, and the lungs to be compressed by the effusion. Magnetic resonance imaging (Fig. 2) suggested a diagnosis of a right-sided Morgagni-type hernia and a decision taken to drain the effusion slowly over a week before performing a repair.
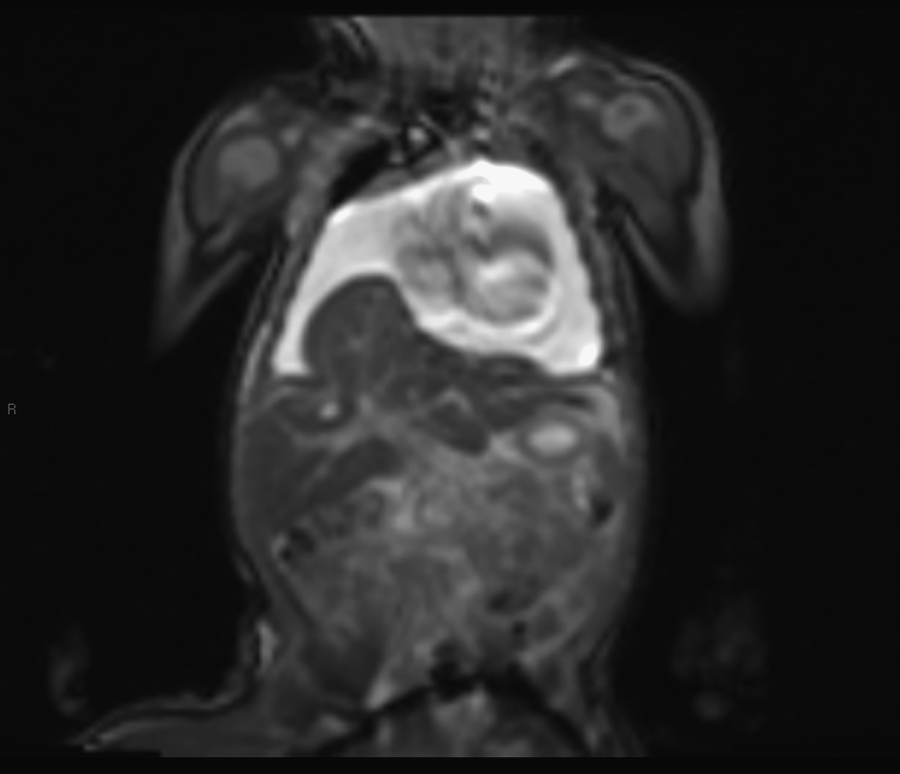
Magnetic resonance imaging scan showing coronal view of probable right-sided diaphragmatic hernia.
Pericardiocentesis was attempted on day 8 of life, but only a small volume of straw-colored fluid could be aspirated. However, this allowed further ultrasonographic observation of the defect, showing that the liver was actually projecting into the pericardium, confirming the diagnosis of a central tendon defect with a massive pericardial effusion.
The decision was therefore to proceed to repair this defect and a laparoscopic approach was favored. A 5-mm umbilical port was sited by an open technique and pneumoperitoneum was established to 8 mmHg. Two 3-mm working ports were sited in the left and right upper quadrants, and a 3-mm grasper was sited in the left flank, by direct puncture, to retract the liver.
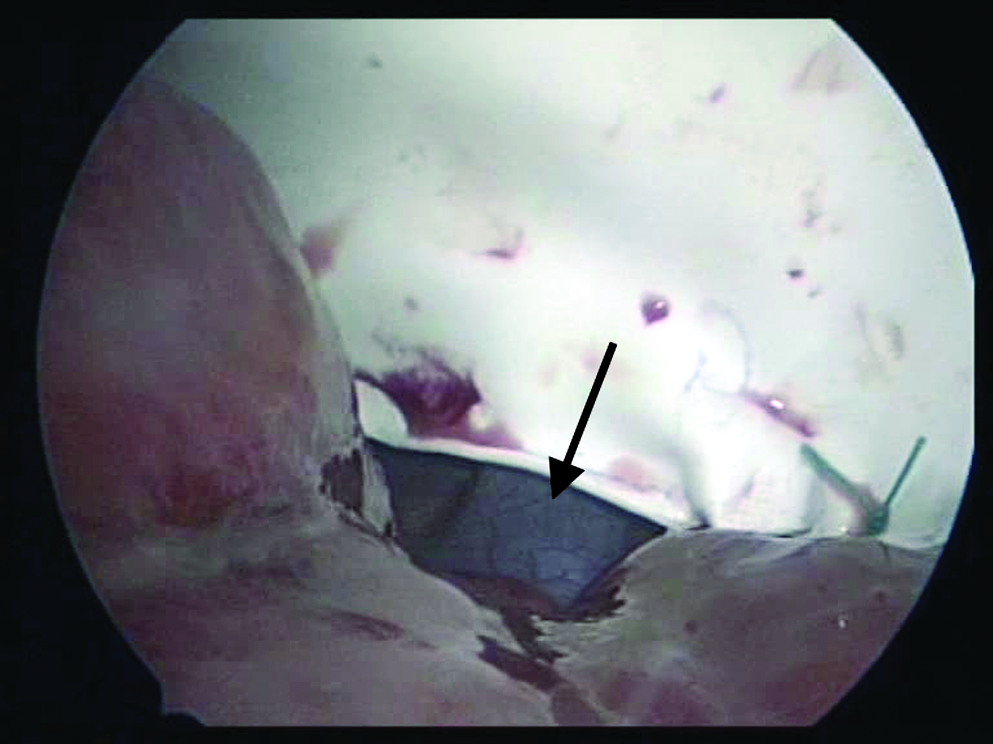
Initial observation of the abdominal cavity showed moderate chylous ascites with fatty congestion of mesenteric lymphatics and a large central defect in the diaphragm with a thin membranous sac separating the peritoneal cavity from the pericardium (Fig. 3). The left lobe of the liver was projecting into the right side of the pericardium and appeared congested and was very friable. The sac was punctured allowing some of the straw-colored pericardial fluid to be aspirated via a 3-mm sucker. The rest of the sac was then circumferentially opened using diathermy. Once this had been completely removed, it was apparent that there was little substantial diaphragmatic muscle, the largest part being a 1-cm rim on the left side of the defect. On observation into the pericardium, the cavity extended to both sides of the chest wall, and the small lungs were visible posteriorly (Fig. 4). Where the left lobe of the liver was protruding into the defect, the inferior vena cava (IVC) was partially compressed; on release of the sac, it was clear that there was no diaphragmatic muscle between this and the defect.
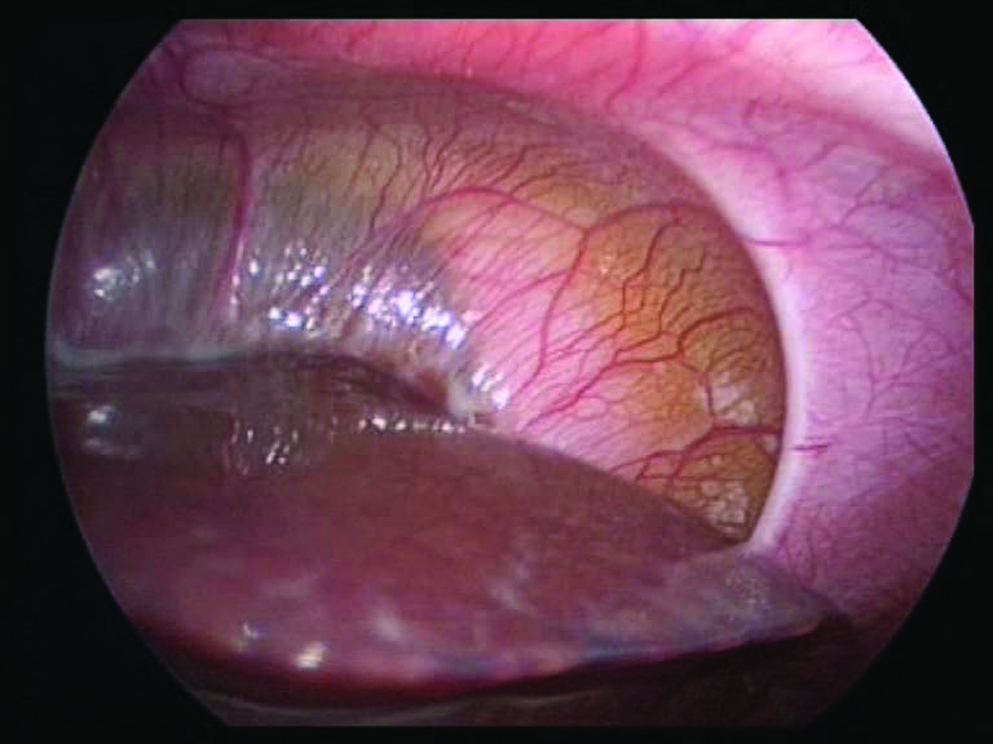
Central defect in diaphragm with thin membranous sac.

Pericardium extending to both sides of the chest wall with small lungs posteriorly.
The defect was roughly measured using a grasper. The left upper quadrant port was changed to a 5-mm port, and a 6-by-3-cm Gore-Tex patch was rolled up and inserted through this port. Unfortunately, it was apparent that this patch would not be big enough and so an 8-by-4.5-cm Gore-Tex patch was used. It was anchored to the posterior rim first using 5/0 ethibond mattress sutures. Further interrupted sutures were placed along the posterior rim of the defect. Care was taken to avoid damaging the IVC, and in fact a small 2–3-mm gap had to be left either side of this (Fig. 5). The patch was then sutured circumferentially to the lip of diaphragmatic muscle.
Small gap left either side of inferior vena cava when suturing patch in place.
Postoperatively, the patient did extremely well. Initial chest radiograph showed the presence of a pneumopericardium, which resolved over 24 hours. Because of the chylous ascites and possible liver congestion, the patient was kept nil by mouth for 5 days. She was extubated on the 2nd day postoperatively and reached her full quota of feeds within 15 days and discharged home the next day.
Initially, she made good progress, with adequate weight gain. However, at 8 weeks postoperatively, her weight gain leveled off and she was noted to be very pale. At this point her hemoglobin was found to be 68 g/dL and her platelet count was 20. Further investigation by the hematology team uncovered a diagnosis of hemophagocytic lymphohistiocytosis, for which she is currently receiving chemotherapy.
Discussion
This is the 14th case of central tendon diaphragmatic hernia with a massive pericardial effusion to be reported. 5 However, to our knowledge this is the first recorded laparoscopic repair of such a defect in a neonate. Paci et al. presented one case of a laparoscopic repair of a central tendon defect, but this was in a man aged 58 who had been thought to have a Morgagni type hernia preoperatively. 6
The outcome for patients with central tendon defects appears to be good. Of the 14 cases in the literature (including our own), 1 was aborted antenatally, 1 died shortly after birth, and 1 died 2 days postoperatively. The other 11 (79%) all survived. 5 This places the mortality of central tendon CDH with pericardial effusion on a par or better than that for the more common Bochdalek-type hernia. 3 We postulate that a central defect has a better prognosis because of a lesser degree of hypoplasia of the lungs, as they will only have only been compressed by the low pressure fluid in the effusion, not by the more solid bowel or liver components of a Bochdalek hernia. It is also worth noting that only one case in the literature was found to have significant problems associated with cardiac tamponade by the pericardial effusion, 7 and we would surmise that the slow build up of fluid in the pericardial sac allows the heart to adapt, and does not compromise it.
The defect lends itself well to repair using the laparoscope in experienced hands. The procedure itself is challenging because of the proximity of the heart and IVC and the size of the defect and lack of diaphragmatic tissue (as well as the small size of a 3.5 kg baby). However, the observation provided by the laparoscope is excellent, allowing very close approximation of the patch around the IVC, and also producing an excellent cosmetic result as seen at 6 weeks (Fig. 6).

The patient's abdomen at 6 months of age.
Although the repair was sound, the size of the defect did necessitate leaving a small gap either side of the IVC. We postulate that this is unlikely to lead to an increased risk of recurrence as the gap was very small and was immediately covered by the liver once this was no longer being retracted. At almost 2 years of age, the patient has no evidence of recurrence on chest X-ray (Fig. 7). Of the 13 cases described in the literature before, 11 proceeded to surgery, 10 of these had a successful repair with no documented recurrence, while 1 died from sepsis on the second postoperative day.
Chest X-ray at 21 months of age.
Unfortunately, our patient subsequently developed hemophagocytic lymphohistiocytosis at 2 months of age. This condition involves severe hyperinflammation caused by uncontrolled proliferation of activated lymphocytes and histiocytes and is characterized by prolonged fever, hepatosplenomegaly, and pancytopenia. There is a familial and an acquired form, both of which appear to be triggered by infection. The acquired form may have an autoimmune cause. There is no documented association with a central tendon defect in the literature, and it may simply represent an unfortunate spontaneous event. 8
In conclusion, a central tendon diaphragmatic hernia should be considered in a neonate referred with a CDH who appears to have a complete whiteout of the lung fields or a difficult to interpret chest radiograph. Laparoscopic repair of central tendon CDH with drainage of effusion is a feasible and safe procedure and we would recommend its use in suitable centers.
Footnotes
Disclosure Statement
No competing financial interests exist.