
Abstract
Abstract
Objective:
To define the role of laparoscopic ureterolithotomy (LU) as a primary modality for large proximal ureteral stones, we compared the outcomes of primary LU with those of ureterorenoscopy (URS), the currently established modality in this circumstance.
Materials and Methods:
Among 71 patients who underwent LU in our institution between February 2005 and January 2010, 32 patients with stone size over 1.5 cm who underwent LU as a primary modality without prior shockwave lithotripsy or URS and for whom LU was conducted as a separate procedure were exclusively enrolled. Based on preoperative characteristics of patients and stones, this patient group was matched with the URS group (n = 32, rigid pneumatic lithotripter) during the same period.
Results:
The LU group and the URS group were similar in age, gender distribution, body mass index, stone size (18.1 ± 4.2 versus 17.9 ± 3.6 mm; P = .88), and stone location. Members of the LU group required a longer operative time (118 ± 53 versus 59 ± 41 minutes; P < .001) and hospital stay (5.9 ± 2.1 versus 3.4 ± 2.4 days; P < .001) and had greater blood loss (155 ± 62 mL). However, stone clearance rate (no remnant stone in postoperative X-ray of the kidney, ureter, and bladder) in a single session was marginally higher in the LU group (93.8% versus 68.8%; P = .06). Total complication rate was not significant and was slightly higher in the URS group (12.5% versus 21.9%, P = .51). Stone migration into the kidney (n = 2 versus 5), ureteral perforation (n = 0 versus 3), open conversion (n = 1 versus 2), and ureteral stricture (n = 1 versus 2), as long-term complications, occurred more frequently in the URS group.
Conclusions:
For large proximal ureteral stones, LU can be conducted safely as a first-line procedure without increase of complication rate, compared with conventional URS. Although LU required a prolonged operative time and a longer hospital stay and blood loss was greater, our data showed an advantage of LU in high clearance rate in a single procedure.
Introduction
Laparoscopic ureterolithotomy (LU) has recently emerged as a novel option for replacement of open surgery in the management of large proximal ureteral stones. Compared with open surgery, a stone can be nearly removed during one procedure using LU, while maintaining advantages over open surgery in terms of analgesia, recuperation, hospital stay, and cosmetics. 6 However, in most of the series using LU, the indication was restricted in selected circumstances. Most indications were shared with that of open surgery, which is generally reserved as the final surgical modality. These include failure with a prior SWL or endoscopic approach, large, impacted stones, or anatomic anomalies, which might require simultaneous surgical correction. 1 From our experience with over 70 cases of LU, we recognized the potential of this modality, combining the previously reported advantages of open and minimally invasive approaches. If these advantages were manifested similarly for proximal large ureteral stones treated with LU as a primary surgical approach compared with URS, the current standard treatment of choice, the indication for LU could be widened. However, lack of a large amount of comparative data hinders our ability to reach a conclusion regarding this issue. As a preliminary study, we present our data on LU compared with URS as a primary procedure.
Materials and Methods
Patients enrolled and data analysis
From February 2005 to January 2010, 71 LUs were conducted in our institution. The initial indication of LU in the initial 30 cases was restricted to patients with prior failure with URS or SWL, distal ureteral stricture, a large (more than 1.0 cm), impacted stone, concomitant laparoscopic surgery for a separate indication, and social or economic necessity for stone removal in a single treatment session. Through these experiences, we recognized that LU can be conducted safely without open conversion while maintaining an acceptable success rate in almost all cases. This encouraged us to carefully expand our indications for LU from January 2007, as a primary procedure for treatment of larger (more than 1.5 cm) upper to mid ureteral stones, if there is no absolute contraindication for laparoscopic surgery. Before conducting LU, all treatment options, including SWL, URS, and PLN, were preoperatively explained and the final treatment decision was made based mainly on the preferences of surgeons and patients after discussion of the advantages and disadvantages of each procedure. From retrospective reviews, 32 patients who chose LU as a primary treatment without prior history of SWL, URS, or PNL, with stone size over 1.5 cm, and for whom LU was conducted as a separate laparoscopic procedure were exclusively enrolled in this series. All patients who underwent LU at our institution were registered prospectively in a specific database that included all important information, such as age, body mass index (BMI), stone location, size, and distance from the intrarenal pelvis. This allowed us to match the parameters of patients who had undergone LU against those of patients who underwent URS during the same period. For equal comparison of the two groups, match-paired analysis was performed with respect to the entire variables mentioned above.
Stone size, which was defined as the maximal diameter, and location of the stone were identified by abdominopelvic computed tomography or intravenous pyelography (IVP) in all patients (Fig. 1A). Distance from the intrarenal pelvis in this series was defined as the shortest distance from the transverse line at the base of the intrarenal pelvis to the superior tip of the stone in an IVP or reconstructed coronal plane image in cases of abdominopelvic computed tomography (Fig. 1B). Postoperative X-ray of the kidney, ureter, and bladder was taken on the day of surgery. For patients with LU, IVP was taken routinely at 3 months after surgery for identification of dilated complications on the ureter. In the URS group, postoperative IVP was taken only if the patient complained of suspicious symptoms, including flank pain or unidentified fever.
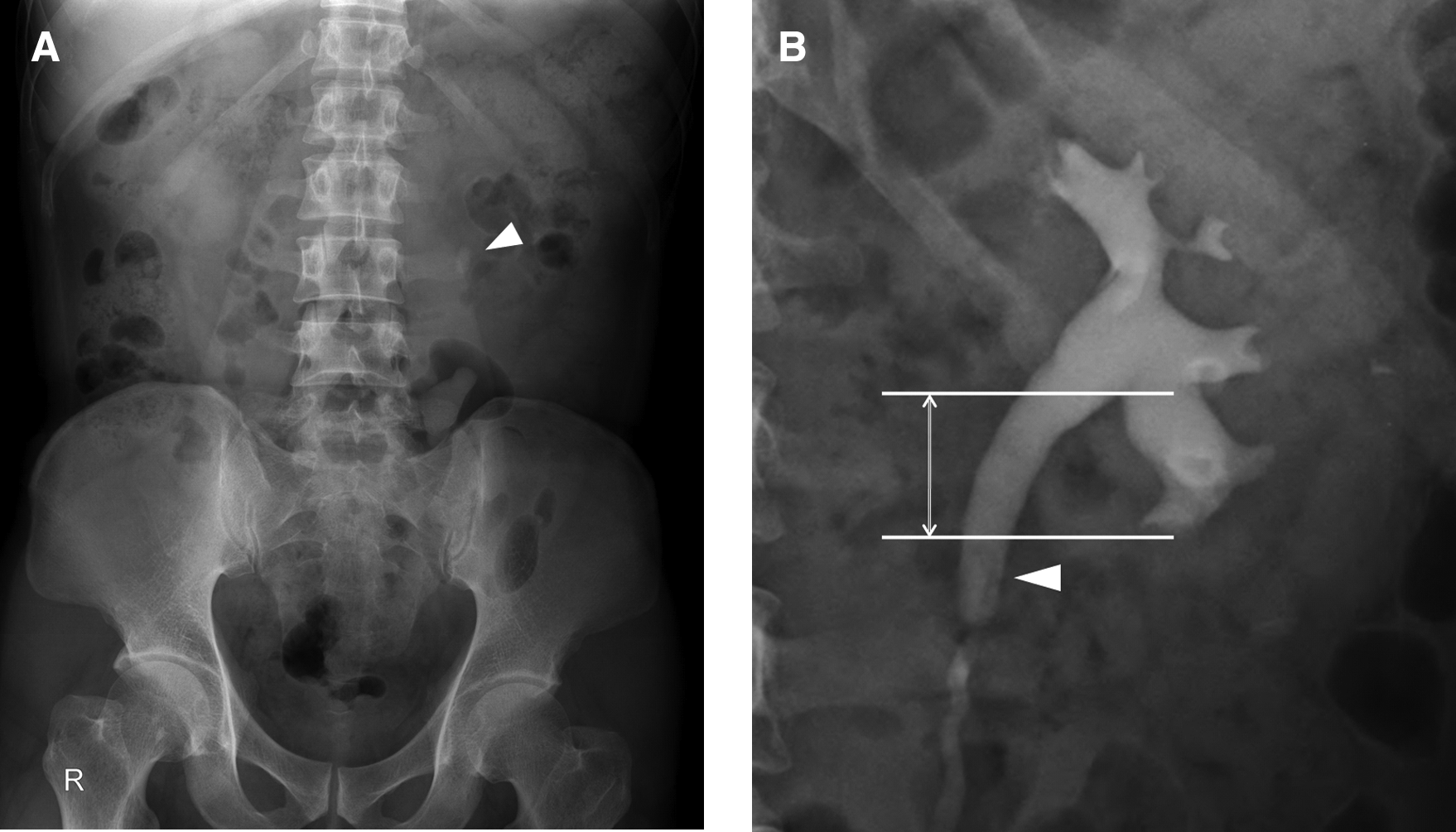
Preoperative and postoperative images.
Perioperative outcomes, including stone-free rate in a single session, operation time, and complications, were analyzed in the two groups. The stone-free rate in a single session, which is the primary end point in this series, was defined as a no residual stone on postoperative X-ray of the kidney, ureter, and bladder taken at 1 day after procedure. If a residual stone was identified in a postoperative image, the case was then designated as a failure in this series, whether the identified stone was removed spontaneously or required axial procedures, including SWL or URS (Fig. 1C).
All data were collated using SPSS ver. 12.0 (SPSS, Chicago, IL) and evaluated by the Mann-Whitney U test, logistic regression test, and chi-square test. A P value of less than .05 was considered statistically significant.
Operative technique
LU in this series was performed by five surgeons (D.Y.C., J.H.B., S.H.K., Y.H.K, and J.Y.P.). All of the surgeons had undergone a minimum of 2 years of training in a laparoscopic fellowship, and each surgeon was familiar with various transperitoneal or retroperitoneal laparoscopic urologic procedures, including radical nephrectomy, partial nephrectomy, and marsupialization of renal cyst. All of these operators had performed a minimum of 10 LU procedures, among a total of 71 cases. Before LU or URS procedure, susceptible antibiotics were applied based on urine culture report to diminish risk of exposure to virulent bacteria. For prophylactic purposes, a single dose of fluoroquinolone was administrated intravenously for all patients, 30 minutes before procedure.
LU was conducted using the conventional three laparoscopic ports under flank position. Using a retroperitoneal approach, a 1.5-cm muscle-splitting incision was made between the tip of the 12th rip and anterior superior illiac spine, depending on the location of the calculi. The peritoneum was pushed forward by an index finger, and a self-made expansion balloon was introduced into the space to create a working space. After insertion of a 10-mm Hasson trocar, the other two trocars (10 and 5 mm) were inserted under laparoscopic vision, parallel to the first trocar in an equilateral triangle fashion. Using the transperitoneal approach, the trocar for the camera was made on the periumbilicus; the positions of the other two trocars were then adjusted depending on the location of the calculi for better surgical performance.
The ureter was generally identified on the major psoas muscle. In an attempt to prevent migration of the calculi, efforts were made to avoid touching the ureter directly, and dissection was carried out cephalocaudally, generally from the renal hilum. The location of the stone was identified by a conspicuous bulge on the ureter. Over the bulging of the stone, a longitudinal incision was made using a cold knife, and the stone was carefully extracted.
The ureter was then routinely catheterized using a standard 6F Double-J stent that was closed at both ends. In earlier cases, it was inserted by the method described by Fan et al. 7 Briefly, the Double-J stent was inserted into the bladder through the ureteral incision site, with the help of a guidewire, which was inserted through the one side hole of the stent. Following removal of the guidewire, the proximal end of the Double-J stent was inserted into the renal pelvis through the incision site. From July 2008, we have applied the method originally described by Khan and Khan. 8 To facilitate the insertion procedure by making it straight, a short guidewire, which was 1 cm greater than the stent, was passed from the two side holes of the stent, making the stent “V” shaped. This V-shaped stent was then inserted through the ureteral incision site; the guidewire was then removed. Using 4-0 vicryl, the incision was closed with three to four interrupted sutures. A drain was inserted in all patients and removed routinely 2 days after LU after confirmation of no urine leakage via check on drain creatinine level. The ureteral stent was extracted 2 weeks later, on an outpatient basis.
URS was performed with a 7.5F semirigid ureteroscope, using a Swiss lighoclast (Richard Wolf) with a 2.4F, 668-mm-long probe. A Double-J stent was placed in patients with large residual stones, significant mucosal edema, stone impaction, or probable ureteral trauma.
Results
Preoperative characteristics are summarized in Table 1. Preoperatively, the LU and URS groups were similar in age, gender distribution, BMI, stone size, and location. During the procedure, blood loss for LU, measured as the amount of blood in the suction device, was 141 ± 24 mL. LU required more operative time (118 ± 53 versus 59 ± 42 minutes; P < .001) and a longer hospital stay (5.9 ± 2.1 versus 3.4 ± 2.4 days; P < .001). However, stone clearance rate in a single session was marginally higher in the LU group (93.8% versus 68.8%; P = .06). In an attempt to identify factors affecting the clearance rate, several variables, including BMI, stone size, and distance from UPJ, were analyzed by logistic regression; however, none of these variables showed predictability (P = .98, 0.71, and 0.52, respectively).
Complications of each procedure are summarized in Table 2. Total complication rate was not significant and was slightly higher in the URS group (12.5% versus 21.9%; P = .51). Stone migration into the kidney and ureteral perforation occurred more frequently during URS. One patient required open conversion in LU because of stone migration into the kidney. In URS, 2 patients required open conversion, one for ureter perforation and another for migration of large stone fragments into the kidney. During a minimum follow-up period of 3 months, 1 and 2 patients with ureteral stricture were found in each treatment group. Of them, 2 patients, 1 from each group, required endoscopic dilatation at 4 and 5 months after surgery, respectively.
Dividing the LU group into subgroups by the method of approach used, blood loss, stone clearance rate, hospital stay, ureteral catheterization period, and complication rates were similar (Table 3). However, the retroperitoneal subgroup required more operative time than its retroperitoneal counterpart (128 ± 54 versus 92 ± 47 minutes; P < .04). Dividing by stenting method, blood loss and operative time were significantly shorter when the modified technique was used (P value = .03 and < .001, respectively).
Discussion
Urinary calculi are the third most common affliction of the urinary tract; recurrence of the condition is observed in routine urological practice. 9 The advent of various new techniques, such as URS, SWL, and PNL, has revolutionized the treatment of ureteral calculi and rendered a need for open surgical lithotomy. 10 Each treatment modality has particular rates of complete stone elimination, additional operational requirements, and complications. Currently, SWL and URS have become the standard treatments for ureteral calculi and offer considerable advantages over conventional open ureterolithotomy. 11 However, for larger ureteral stones over 1.5 cm in maximal diameter, there is still controversy over which modality can obtain the best clearance, minimizing morbidity in nature. Success of SWL in ureteral stone removal is dependent on the size of the stone; thus, the stone-free rate after a single SWL session decreases from 84% to 42% when the stone is larger than 1.0 cm. 12 For proximal ureteral stones, based on a promising stone-free rate in a single session, URS is currently established as the first choice. 13 However, as the majority of upper ureteral stones were near the renal pelvis, the stones tend to be brushed easily into the renal pelvis, leading to URS surgical failure, 14 particularly when a pneumatic lithotripter was used. Currently, according to recent available guidelines, no clear-cut mention of treatment modality was made when the size of the calculus is greater than 1.0 cm. 15 Although the 2007 AUA/EAU Ureteral Stones Guideline Panel reported that PNL is an acceptable first-line treatment in selected cases with large, impacted stones in the upper ureter, 16 it is associated with a relatively high morbidity and a potentially large degree of bleeding, despite its high stone-free rate, because it requires access through the renal parenchyme. 17
Although the advantages of LU as a treatment modality for large proximal ureteral stones have been reported, LU has been used as a feasible alternative for treatment of these difficult stones. 18 Reported indication of LU includes a salvage procedure for failed SWL or an endourologic approach, selected patients with large chronically impacted ureteral stones, a need for a concomitant laparoscopic operation for a separate indication, and lack of the appropriate technological facilities. 19 However, these indications have not been clearly defined and may vary from center to center depending on the available expertise. Indeed, because of excellent results with the new endourologic technology, most data from developed countries demonstrate a considerable population for whom LU is applied as a salvage procedure. In contrast, recent data on LU as a primary procedure were mainly released in developing countries, which do not have easy access to endourologic facilities and SWL.20,21 Considering this, to obtain the actual benefit from the laparoscopic approach, we focused on the patient group in whom LU was applied as a primary procedure, without prior trials using endoscopic or SWL treatment.
As is evident from many clinical series, the greatest advantage of LU is the high probability of removing a large stone in one session without need for additional procedures. A success rate of greater than 95% has been described by various researchers, 22 and it was also regenerated in our data. This benefit can be particularly maximized for patients with a solitary kidney or functional renal disease, or a social or economic necessity for stone removal in a single treatment session. This high success rate, which is comparable with that of URS using a laser, can be advocated in centers where a facility with laser equipment is not available or in centers where ureteroscopy devices are not readily available. In contrast, laparoscopy is currently available at many centers, which makes it an alternative option than the endoscopic approach. 23 In SWL, retreatment is necessary in up to 36% of patients, 24 and auxiliary procedures, including ureteral catheter insertion or endoscopic manipulation, are required in about 46% of cases. 3 Particularly large proximal stones also pose a significant challenge for modern endoscopic techniques, often requiring several endoscopic procedures. 3 For stone fragments brushed into the renal pelvis, acceptance of SWL as a further treatment remains to be obtained. 25
Although obvious advantages are associated with a high success rate, a general reluctance still exists with regard to use of LU for larger upper ureteral stones, 26 mainly because of prolonged operative time and EBL, compared with URS. Disadvantages of laparoscopy also include a longer hospital stay, risk of injury to intra-abdominal structures inherent in the laparoscopic approach, and the inherited risk of conversion to open surgery. Regarding this point, our data show how the surgical outcome of LU can be improved. In the conduct of LU, the access can be carried out via the transperitoneal or retroperitoneal approach. The retroperitoneal approach has advantages over transperitoneal access by obviating compromise of the peritoneum and mobilizing the viscera, which could reduce the occurrence of complications. 27 However, the retroperitoneal approach offers a limited working place and finding the ureter is often difficult because of lack of anatomical landmarks. In fact, Harewood et al. 28 reported in their series that two of three retroperitoneal approach cases were converted to transperitoneal laparoscopy because of a limited working place. In a prospective study 29 comparing transperitoneal and retroperitoneal approaches during the learning curve, significant differences were demonstrated in favor of the transperitoneal procedure in terms of time for access to the operating field, time for suturing of the ureter, and total operative time. Similar to these observations, the transperitoneal approach in our series required significantly less operative time than the transperitoneal approach, with the same complication rate.
Post-LU stenting of the ureter is mandatory if the morbidity of the procedure has to be kept low. However, one of the difficulties encountered during this procedure is the placement of a stent after stone extraction, which, in our experience, was the most time-consuming procedure. The standard Double-J stent is soft and pliable and curls at both ends because of inherent memory, necessitating both great expertise and considerable patience to ensure its placement in the correct position inside the ureter. However, placement of the stent by the standard technique also adds considerably to the operating time. Gaur et al. 30 reported a mean operating time of 92 minutes when the ureter was stented and sutured and only 66 minutes when the ureter was left open. Moreover, the narrow space of the retroperitoneal cavity made it difficult to operate when the Double-J stent twisted in the operating field. To facilitate this procedure, modifications to standard stenting techniques have been invented by several authors.7,8 By application of those methods, we observed obvious improvement in terms of operative time and blood loss.
We recognized several limitations in this study. The first drawback is that the data were collected from different surgeons without randomization. LU procedures were performed by five different surgeons with different surgical experience. This difference in cases of LU may affect the learning curve of each surgeon, resulting in a difference in operative time, blood loss, and complication rate. In addition, considering the relatively small number of cases with primary LU, it was not possible to perform a randomized study. Second, the relatively high complication rate in the pneumatic URS group in this series should be interpreted with care. Along with advances in the flexible URS, its ability to access the upper urinary tract, combined with laser-based lithotripsy, particularly using holmium YAG laser, made the flexible ureteroscopic laser lithotripsy more attractive to treat complicated ureteral stones with high success rate and low morbidity. Although stone size and location were variable, considering reported stone-free rates over 90%31,32 and complication rates below 10%,31,33 this novel device may offer a more effective and definitive treatment. In particular, stone migration, which was the most common complication of pneumatic URS in this series, may be reduced using the flexible URS with laser lithotripsy. Finally, the prolonged patient hospitalization of 3.4 days in the URS group compared with that of other published data deserves to be explained here. This prolongation is mainly caused by the characteristics of Korean Health Care system, which is national and mandatory. Because of this national coverage, the hospital admission cost can be maintained at a minimum compared with the costs of other nations; therefore, the patients and doctors alike are not aggressive in scheduling an early discharge. Despite these limitations, our data show that LU may be considered as the first-line management for large impacted ureteric stones, especially to ensure that patients become stone-free within a single operation. Prospective, randomized trials comparing these modalities for treatment of large ureteric calculi may prove the efficacy of one modality over the other.
Conclusions
For large proximal ureteral stones, LU as a primary procedure can be conducted safely as a first-line procedure without increase of complication rate, compared with the conventional URS. Although LU required a prolonged operative time, greater blood loss, and a longer hospital stay, operative time can be decreased by application of a transperitoneal approach and modification of the stenting method. Our data show an advantage of LU regarding high clearance rate in a single procedure, implying its clinical efficacy particularly in the absence of flexible ureteroscopes or laser-based lithotropic equipments.
Footnotes
Disclosure Statement
No competing financial interest exists.