
Abstract
Abstract
Aim:
The aim of this study was to assess the efficacy, reliability, and performance of the Lapra-Ty clip (LTc) during intracorporeal Roux-en-Y gastrojejunostomy in a totally laparoscopic distal gastrectomy (TLDG).
Materials and Methods:
Between May 2009 and October 2009, we performed TLDG on 25 consecutive early gastric cancer patients. Two-bowel anastomosis was done intracorporeally in the side-to-side fashion using Endo-GIA, and closure of the entry hole was done by LTc with a running suture.
Results:
There were no postoperative leakages, bleeding, or strictures in the gastrojejunostomies and jejunojejunostomies. We had a single intraoperative complication where the Levin tube was jammed at the gastrojejunostomy site, so a revision was done. Total mean operation time was 254.4 minutes (range, 170–485) and mean anastomosis time was 49 minutes (range, 30–110). Mean hospital stay was 7.9 days (range, 5–17), and mean time to liquid diet was 2.6 days postoperatively (range, 2–5).
Conclusion:
The usage of LTc is safe and efficient for bowel anastomosis, especially TLDG in humans, and adoption of LTc may help to reduce overall operative times. Perhaps, most importantly, it can cover the disadvantages of TLDG by making TLDG more easily executable in gastric cancer.
Introduction

Lapra-Ty absorbable suture clips.
Materials and Methods
Patients
This study was approved by the Institutional Review Board for human investigation of Soonchunhyang University Hospital. Twenty-five patients with gastric cancer who underwent TLDG using LTc between May 2009 and October 2009 were enrolled in this study. The indications for TLDG in patients with gastric cancer were as follows: the depth of tumor invasion was less than the submucosa layer of the stomach wall on endoscopy and endoscopic ultrasound, the tumor was located in the middle or lower third of the stomach, and there was no evidence of lymph node metastasis on computed tomography and endoscopic ultrasound.
Operative procedure
After duodenal transection and regional lymph node dissection (D1+α or β), the stomach was transected with an adequate margin (>3 cm) under aid of intraoperative endoscopy. First, we removed the specimen through the umbilical trocar and then we checked the resection margin by frozen biopsy. After recreating a pneumoperitoneum, about 10-cm jejunum was resected at 25–30 cm distal to the ligament of Treitz. We then made a jejunal Roux limb and bilio-pancreatic limb without division of the mesentery. A small hole was made on the antimesenteric border of the biliopancreatic limb and the Roux limb from 30 cm distal to the gastrojejunostomy site. A side-to-side jejunojejunostomy was performed using a linear stapler (ETS 45; Ethicon Endosurgery), and the entry hole was closed by the following method: the LTc was prepared at the terminal end of the suture and the suture was passed as a running suture, and an additional clip was used to cinch it down and secure the suture. A gastrojejunostomy was performed by the same method as the jejunojejunostomy on the posterior wall of the stomach. The jejunal mesenteric defect was closed by a running suture using LTc (Fig. 2). Before closure of the trocar site, we performed a leak test with air and blue dye on the gastrojejunostomy site.
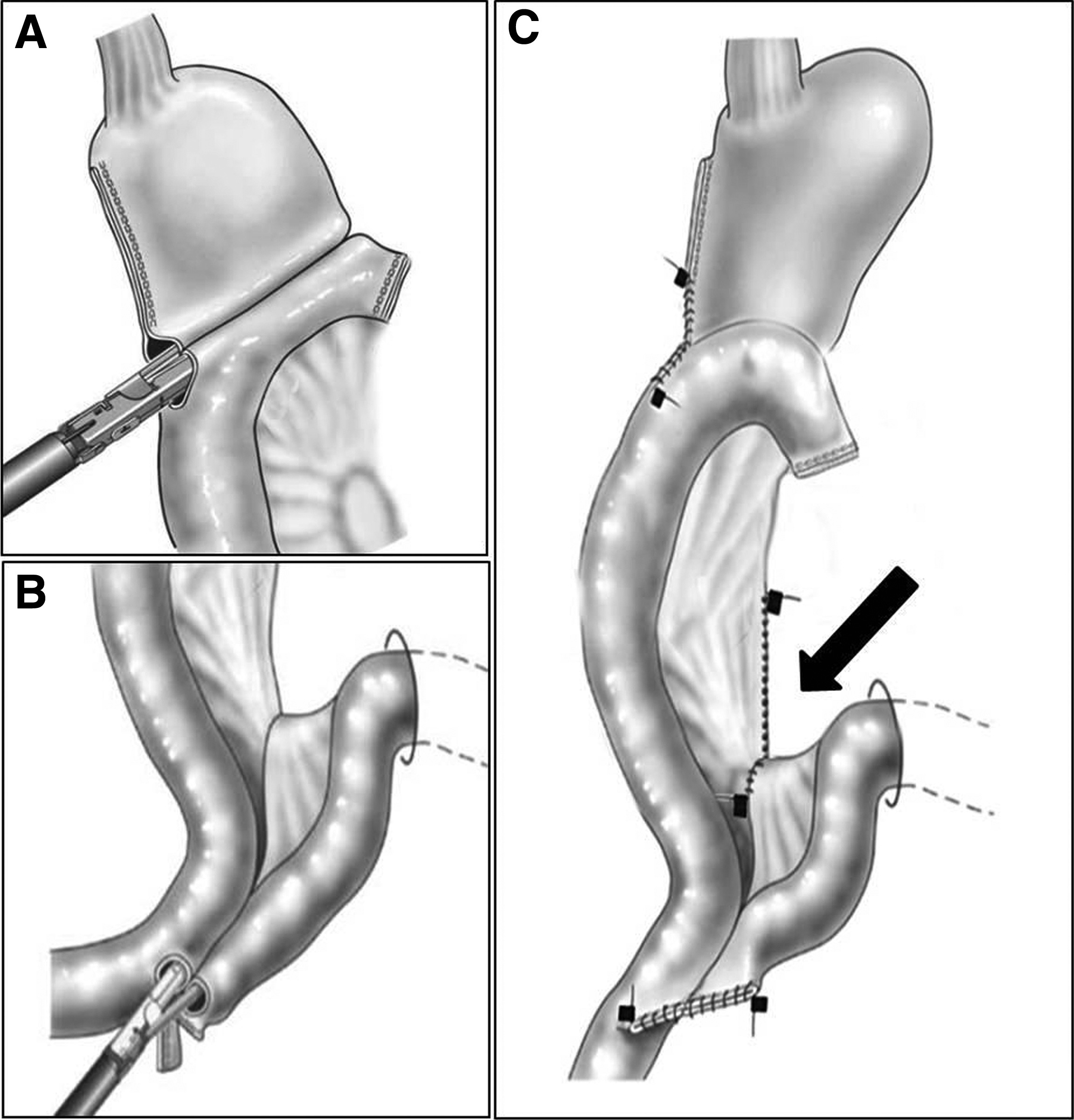
Schematic illustration of laparoscopic intracorporeal Roux-en-Y gastrojejunostomy.
Postoperative assessment
The integrity of the anastomosis was checked on postoperative day (POD) 1 by the use of a water-soluble contrast medium (Gastrografin; Bayer Schering Pharma). Anastomosis-related complications were defined as follows: leakage—air-containing fluid collection around the anastomotic site on computed tomography scan, or confirmed leakage on an upper gastrointestinal series with corresponding symptoms; stenosis—narrowing of the anastomotic site confirmed by upper gastrointestinal series or endoscopy; bleeding—condition requiring transfusion or other postoperative interventional procedure.
Results
Table 1 shows patient demographics and postoperative outcomes. Mean age was 54.68 ± 12.45 years, and 16 male and 9 female patients underwent TLDG using LTc. Their mean body mass index was 24.35 ± 3.03 kg/m2. The patients tolerated a liquid diet at 2.6 days after operation, and mean hospital stay was 7.9 days. Despite no postoperative mortality and no anastomosis leaks, there were three cases of major complications: a 62-year-old woman suffered from gastric stasis at 5 days after operation, and she was discharged on POD 17; there was one wound infection in a 73-year-old male patient, and wound revision was performed on POD 7; and in another case, the Levin tube was jammed at the gastrojejunostomy site intraoperatively, so anastomotic revision was performed.
SD, standard deviation.
The details of the clinical and pathological findings of cancer are shown in Table 2. Mean number of harvested lymph nodes was 31, three patients (12%) had lymph node metastasis, and mean length of the proximal resected margin was 6.2 cm. Figures 3 and 4 show the total operation time and the anastomosis time in each case. The mean operation time was 254 minutes and the mean time for intracorporeal anastomosis was 49 minutes. In three cases, partial gastrectomy failed, so conversion to distal gastrectomy occurred and operation time was delayed (arrow in Fig. 3). There was one anastomosis revision because of a jammed Levin tube, and the anastomosis time reached 110 minutes in the 23rd case. Except for that case, the anastomosis time stabilized at 40 minutes after 10 cases of experience (Fig. 4).

The total operative time in each case. The operation was delayed because of intraoperative conversion from wedge resection to distal gastrectomy (black arrow).
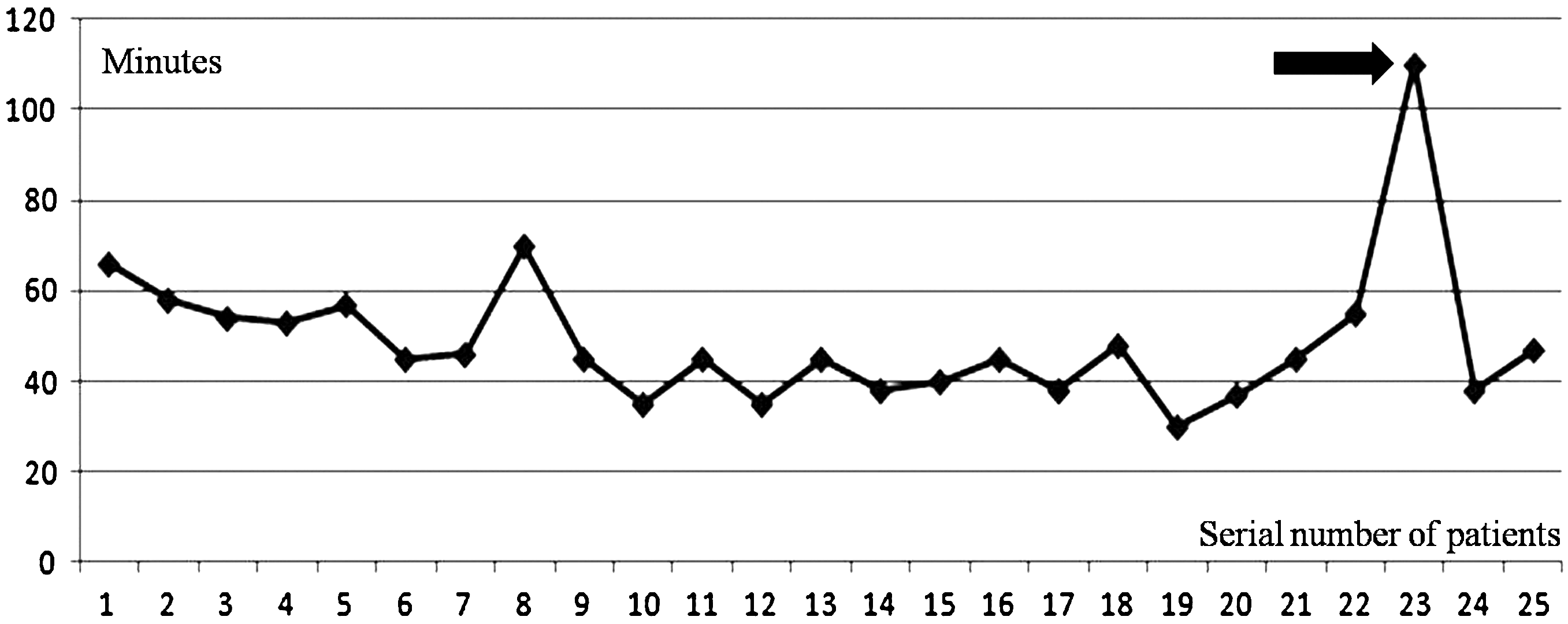
The anastomosis time in each case. A revision was needed because of accidental jamming of the nasogastric tube in the linear stapler used in the side-to-side gastrojejunostomy (black arrow).
Discussion
Gastric cancer is one of the most common malignancies in the Republic of Korea, and the incidence of early gastric cancer is about 50%. 6 In Korea, 1086 cases of laparoscopic gastric surgery were performed in 2004, 7 and in Japan, 22.5% of distal gastrectomies were performed laparoscopically in 2005. 8 However, LADG was still performed in most laparoscopic gastrectomies, which requires a mini-laparotomy incision for anastomosis. The rate of postoperative complications after laparoscopic distal gastrectomies was reported as 9.2%, and 54% of them were related to the anastomosis, including leaks, stenosis, and passage obstruction of the anastomosis site. 8
TLDG is considered to have several advantages over LADG. In LADG, extracorporeal anastomosis via a mini-laparotomy incision may cause forceful tension and injuries to the structures around the anastomosis because the anastomosis has to be performed in a limited, narrow, and restricted space, especially for obese patients with thick abdominal walls and patients with a small remnant stomach. In contrast, the entire anastomosis can be performed in clear view in TLDG, so such tension and injuries can be obviated. However, TLDG also has some disadvantages: difficulty in intraoperative localization of the tumor because early gastric cancer is not visible or palpable, so other methods are needed such as intraoperative endoscopy to figure out the location; and longer operation time because intracorporeal anastomosis is a difficult laparoscopic skill.
Several devices have been introduced to simplify laparoscopic suturing and knot tying.9–11 LTc has been used to reduce warm ischemia time knot tying for laparoscopic partial nephrectomy. 4 The use of LTc for bowel repair has been reported only in porcine models. 5 To our best knowledge, no report has been published in humans. Orvieto et al. 5 reported that there was no abscess or significant narrowing of the enterotomy site after enterotomy and bowel closure using LTc in necropsies. Also, there was no evidence of clip migration or erosion into the epithelium, and though some capsule thickness was noted, it was similar at 2, 4, and 8 weeks postoperatively on histologic findings. Also, the inflammatory reaction around the LTc was less pronounced than the reaction around the sutures. In our study, there were no anastomosis complications such as leaks or narrowing after repairs using LTc.
Benway et al. 4 reported that the technique for renorrhaphy after robotic partial nephrectomy using LTc provides a highly efficient and effective repair that is quickly learned and easily implemented. As Figure 4 shows, the learning curve for using LTc required only 10 cases in this study; it seems that the use of LTc is not difficult to learn.
Although there are no confirmed data, using the LTc may help to shorten the operative time and it is easy to learn compared with simple suturing. Also, the price of one clip is 17 U.S. dollars, and 6 clips are used in TLDG procedure, which costs only extra 102 U.S. dollars; it has an advantage over Endostich and stapler, as their cost is more than LTc. A well-designed study is needed to evaluate the use of LTc for anastomosis time compared with other techniques such as LADG, the use of Endostich or stapler, and just simple suturing.
Conclusions
The use of LTc is safe and efficient for bowel anastomosis, especially TLDG in humans. Adoption of LTc may help reduce overall operative time and need only less extra cost. Perhaps, most importantly, it can cover the disadvantages of TLDG by making TLDG more easily executable in gastric cancer.
Footnotes
Disclosure Statement
No competing financial interests exist.