
Abstract
Abstract
Introduction:
We present our single-center contemporary experience with laparoscopic radical nephrectomy (LRN). LRN is an established minimally invasive approach comparable to open radical nephrectomy for the treatment of renal cortical neoplasms. Technical advancements and surgical experience with LRN mandate a re-evaluation of contemporary outcomes.
Methods:
Between June 2005 and July 2009, 74 patients underwent LRN for an enhancing renal mass. Six of these patients underwent a cytoreductive nephrectomy for metastatic renal cell carcinoma. Patient demographics, perioperative data, tumor characteristics, complication rates, and outcomes were retrospectively collected and analyzed from our prospectively established renal database.
Results:
The mean follow-up for patients undergoing nephrectomy without metastasis was 17.4 months (1–52 months). The mean estimated blood loss was 93 mL (0–600 mL) and the overall complication rate was 5.9%. Two patients developed metastatic disease after surgery, both of whom had high-stage (pT3a) tumors. No death was caused by renal cell carcinoma. In the cytoreductive cohort, the mean estimated blood loss was 592 mL (200–1200 mL). Four were high stage (pT3a/pT3b). The mean follow-up was 4.7 months (1–15 months), with an overall survival of 50%.
Conclusions:
With contemporary technology and increased laparoscopic surgical experience, LRN and, in selected cases, cytoreductive LRN can be performed safely and effectively for the majority of renal tumors. Experience has resulted in a reduction in operative time and blood loss complication rates. LRN remains the approach of choice for the management of renal cortical neoplasms not amenable to nephron-sparing surgery.
Introduction
Materials and Methods
We retrospectively reviewed our prospectively established IRB-approved database for patients undergoing LRN. All patients had evidence of an enhancing renal mass on abdominal cross-sectional imaging (CT or MRI), and all underwent a standardized evaluation for metastatic disease, including a chest X-ray or CT scan and liver function tests. Before surgery, patients were counseled regarding alternative treatment options, including active surveillance, open or laparoscopic partial nephrectomy, laparoscopic or percutaneous renal cryoablation, ORN, and LRN. LRN was performed using a standard 3–5 trocar technique with complete renal hilar dissection to obtain excellent vision before transection of the renal vessels. Temporary occlusion of the dissected renal artery combined with intraoperative ultrasound evaluation using the continuous flow monitoring system is performed in all cases. This is done to determine a single arterial source before renal vein transection. All specimens underwent intact extraction after entrapment with a 10-mm Endo catch bag (Covidien, Mansfield, MA). Thirty-one cases (45.6%) included concomitant ipsilateral adrenalectomy.
Medical records were reviewed to collect baseline and perioperative information, including patient age, American Society of Anesthesiologists score, operative time, estimated blood loss (EBL), conversions to open nephrectomy, complications, length of hospital stay, time to oral intake, time to ambulation, and analgesic requirements. Pathological characteristics included tumor size (based on cross-sectional imaging), specimen weight, histology, and pathologic stage. All pathologic data were determined by the Department of Pathology at Columbia University Medical Center. Patients were followed at 3 and 12 months after surgery with chest x-ray and routine blood work, including liver function tests. Abdominal cross-sectional imaging was obtained at 12 months after surgery, and annually thereafter.
Results
Between June 2005 and July 2009, 74 LRNs were performed by a single surgeon (J.L.) for an enhancing renal mass, including 6 patients undergoing a cytoreductive LRN. In the nonmetastatic cohort, the mean patient age at the time of surgery was 64.0 years (range 26–93 years). Mean American Society of Anesthesiologists score was 2.2 (range 1–3). The mean operative time was 138.7 minutes (range 77–240 minutes) with a mean EBL of 93 cc (range 0–600 cc) (Table 1). The mean tumor size and specimen weight were 5.9 cm (1.6–18.0 cm) and 657.7 g, respectively. Sixty-four (94%) tumors were found to be RCC variants. Of the RCC variants, 46 (71.8%) were conventional (clear cell), 8 (12.5%) chromophobe, 4 (6.3%) papillary type I, 4 (6.3%) papillary type II, and 2 (3.1%) unclassified tumors (Table 2). Pathological stage was pT1a in 13 (20.3%) patients, pT1b in 26 (40.6%), pT2 in 8 (12.5%), pT3a in 10 (15.6%), and pT3b in 7 (10.9%) tumors. Histopathology revealed 3 (4.4%) oncocytomas and 1 (1.5%) cystic nephroma.
ASA, American Society of Anesthesiologists; EBL, estimated blood loss.
RCC, renal cell carcinoma.
In the perioperative period, the mean analgesia requirement was 35 mg of morphine. Average time to ambulation and oral intake was 22.8 and 19.6 hours, respectively. Thirty-nine patients (59%) were discharged home on postoperative day 1 and 20 (30%) were discharged on postoperative day 2. The mean hospital stay was 2.1 days (range 0.67–8.0 days). Overall, four complications occurred (5.9%) with two intraoperative and two postoperative complications. One patient required an intraoperative blood transfusion of one unit of packed red blood cells. The case was eventually converted to an open approach secondary to tumor size. The kidney was found to be adherent to both the spleen and pancreas causing mobilization to be quite difficult. Another patient experienced from a trocar injury to the right colon during laparoscopic access. A 1-cm colotomy was closed with intracorporeal suturing technique, and the patient did not suffer any postoperative sequelae. Postoperatively, 2 patients presented with a port or extraction site hernia with only one requiring surgical repair. This consisted of a laparoscopic incisional hernia repair with mesh performed electively.
The mean follow-up for the cohort was 17.4 months (1–52 months). Two patients developed metastatic disease during follow-up. The first patient presented initially with a 4.5-cm endophytic renal tumor, which on final pathology was found to be a high-grade pT3a-conventional RCC. After a 50-month follow-up, he presented with bone metastasis. The second patient presented 11 months after radical nephrectomy (high-grade pT3a-conventional RCC) with bilateral pulmonary nodules. This patient underwent a thoracotomy and wedge resection of the nodules, which demonstrated RCC with negative margins. At this time, with 21 months of additional follow-up, the patient has bilateral sub-centimeter pulmonary nodules that have remained stable over the last 11 months. Two recorded deaths have occurred since radical nephrectomy (Fig. 1). Both were patients with pT3a at final pathology. Both patients are currently alive with recurrent RCC.
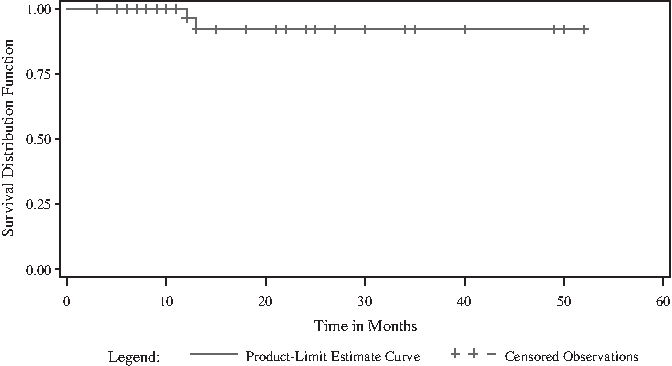
Kaplan–Meyer curve for nonmetastatic laparoscopic radical nephrectomy series.
Six patients were found to have metastatic RCC and underwent a cytoreductive radical nephrectomy before adjuvant therapy. The mean age in this cohort was 62 years (49–67 years). The mean tumor size was 9.2 cm and mean EBL was 592 mL (200–1200 mL). Five patients demonstrated conventional clear cell tumors and 1 patient had papillary RCC histology. Pathologic stage included pT2 (2 patients), pT3a (2 patients), and pT3b in 2 patients. One patient resulted in an open conversion secondary to significant hemorrhage (1200 mL) and received transfusion in the immediate postoperative period. This patient had a 10-cm tumor and was high stage (pT3b). There were no postoperative complications. Location of metastatic disease included pulmonary (6 patients), bone (4 patients), brain (2 patients), and spleen (1 patient). At a mean follow-up of 4.7 months (1–15 months), the overall survival was 50%.
Discussion
LRN is well established as a standard-of-care approach for renal cortical neoplasms, which are not amenable to nephron-sparing approaches. Early experience with LRN demonstrated the technique to be an inefficient procedure due to lengthy operative times. In an earlier series, McDougall et al. originally reported a mean operative time of 6.9 hours. 7 More recent series of LRN demonstrate an improvement in perioperative parameters such as operative time (105–256 minutes) and blood loss (147–287 mL).9,11–16 In the current study, the mean operative time and blood loss were 138 minutes and 90 mL, respectively, indicating the trend toward progressive improvement with an extended experience. Burgess et al., in a randomized controlled trial, compared transperitoneal LRN and ORN. 11 The authors examined outcomes such as blood loss, operative time, hospital stay, pain scores, complications, and return to normal activity. The mean visual analog pain scores were significantly lower in the LRN group than in the open group. No statistically significant differences were found in the remaining parameters. Two patients in the LRN group underwent open conversion and 1 patient developed a port-site dehiscence that required surgical repair. 11
Complication rates have also decreased in recent series (Table 3). The British Association of Urological Surgeons reported a complication rate of 16.8% and a conversion rate of 6.8% for LRN. 17 Gong et al. reported a 19% major and 18% minor complication rate. 12 In our series, we had a overall complication rate of 5.9%, and a conversion rate of 1.4%. The low complication rate and conversion rate are most likely the result of our team's surgical experience. During and before this study, a substantially larger number of more complex nephron sparing renal procedures were performed. The experience gained from these more challenging cases likely resulted in the ability to avoid intraoperative complications. Additionally, our postoperative care aggressively emphasizes patient mobilization such that many common complications such as atelectasis and its associated fevers and vascular complications such as pulmonary embolus are avoided.
LRN has also been shown in multiple series to provide equivalent oncologic control compared with ORN in T1 and T2 RCC.13,14 Permpongkosol et al. reported long-term oncologic efficacy in 121 patients after LRN (67 patients) and ORN (54 patients). Patients were all clinical stage T1 or T2. Follow-up of 73 months in the LRN group and 80 months in the ORN group revealed that the 5- and 10-year cancer-specific survival rates were not significantly different. 15 Long-term (≥10 year) oncologic outcomes after LRN have been reported in a multi-institutional study of 73 patients who underwent LRN by two surgeons. The mean tumor size on CT was 5.0 cm. High-grade (Fuhrman ≥3) tumors were present in 28% of the cohort, and pathologic stage T3 and T4 existed in 13% and 1% of patients, respectively. Ten-year overall, cancer-specific, and recurrence-free survival rates were 65%, 92%, and 86%, respectively. 16
New technology and an improved technical proficiency among surgeons have expanded the indications for LRN to include large-diameter and higher stage tumors. Bird et al. performed LRN on patients with T2 and T3 RCC and examined perioperative outcomes and complications. Two-hundred fifty-two laparoscopic nephrectomies were performed (97.6% for RCC), with 55 (21.8%) being pathologic stage T2 or T3. Higher stage tumors were associated with a greater blood loss and a postoperative complication rate that was significantly higher compared with lower stage (T1) tumors. 9 In the current series, 36% of cases were pT2 or higher tumors.
Renal vein and caval thrombi have also been managed laparoscopically. Desai et al. presented a small series of 8 patients with gross renal vein thrombi managed laparoscopically. One patient required open conversion secondary to hemorrhage. 18 In the absence of metastatic disease, surgery provides a long-term disease-free survival in over 40% of these patients. 19 In the current series, 4 (6.2%) patients had evidence of renal vein involvement. One of these patients developed pulmonary metastasis while on surveillance following LRN. In cases involving a tumor thrombus in the renal vein, the renal artery is first ligated and divided and the vein fully exposed and isolated. An articulating gastrointestinal anastomosis (GIA) stapler is placed proximally against the wall of the vena cava. In patients with a level I thrombus (≤2 cm above the renal vein), the jaws of the GIA stapler can be used to milk the thrombus distally into the renal vein before transection. 10
Conclusions
LRN is the approach of choice for the management of renal cortical neoplasms not amenable to nephron-sparing surgery. New developments in equipment and the experience level of laparoscopic surgeons have led to improved intraoperative and perioperative outcomes. Contemporary experience has allowed LRN to have broader application and currently allows for the minimally invasive treatment of patients with clinical stage T3 as well as selected patients requiring cytoreductive nephrectomy for metastatic disease. This contemporary series provides another baseline measure for which new standards of care can be compared.
Footnotes
Disclosure Statement
No competing financial interests exist.