
Abstract
Abstract
Objectives:
The Habib 4 × radiofrequency-assisted bipolar hemostatic device (AngioDynamics) was used during select open partial nephrectomies to minimize blood loss and prevent warm renal ischemia. The article and video demonstrate this novel technique for partial nephrectomies in select renal masses.
Methods:
Patients with large renal tumors requiring partial nephrectomy where avoidance of warm ischemia was deemed imperative underwent open partial nephrectomy at our institution utilizing the Habib 4 × radiofrequency ablation device to avoid prolonged warm ischemia time and prevent blood loss.
Results:
We have used the device successfully in 4 partial nephrectomies (2 patients with solitary kidneys, 2 patients with bilateral large masses). The mean age was 65 years. Mean tumor size was 6.4 cm. All tumors were located either in the upper pole or lower pole of the kidney. Mean hospital stay was 4.6 days. No patient received an intraoperative blood transfusion. Two patients required long-term ureteral stenting and surgical drainage for urine leakage.
Conclusions:
Bipolar radiofrequency ablation offers avoidance of hilar clamping in carefully selected large partial nehrectomies.
Introduction
Materials and Methods
Radiofrequency device
The Habib 4 × radiofrequency-assisted bipolar hemostatic device (Habib) is a hand-held, disposable radiofrequency (RF) energy device (Fig. 1). 7 It consists of a 2 × 2 array of needles arranged at the corners of a 6 × 7 mm rectangle with an active end of 6 or 10 cm in length. The needles are made of stainless steel with a polished titanium nitride nonstick coating to facilitate insertion and removal from tissue. 8 The device is connected to a 500-kHz generator (Rita Medical Systems, Inc.) that produces up to 250 W of RF power. A pneumatic foot pedal turns the RF energy on and off. 6 The device also measures generator output, tissue impedance, temperature, and time. 7

The Habib 4 × radiofrequency-assisted hemostatic device. The Habib 4 × radiofrequency-assisted bipolar hemostatic device (AngioDynamics). The hand-held, disposable radiofrequency (RF) energy device consists of a 2 × 2 array of needles arranged at the corners of a 6 × 7 mm rectangle with an active end of 6 or 10 cm in length.
The device operates via RF energy, creating coagulative necrosis and hemostasis by generating iconic friction within tissue that results in heating.8,9 The heating occurs between the electrodes and can reach 100°C. This heating causes cellular dehydration and leaves a coagulated zone between the electrodes (Fig. 2). The bloodless plane of division is situated between the lines defined by the two electrodes, and sharp cutting in this zone should provide a homogeneous avascular plane.

Coagulation zone created by the electrodes. The heating between the bipolar electrodes causes cellular dehydration and leaves a coagulated zone between the electrodes that acts as a bloodless plane of division. Sharp cutting in this zone should provide a homogeneous avascular plane.
Patient selection
Any patient suitable for partial nephrectomy is a candidate for Habib utilization. Patients with solitary kidneys and small renal masses (<3.5 cm) should be considered for percutaneous or laparoscopic thermal ablation. Laparoscopic partial neprectomy can also be considered for smaller masses in solitary kidneys or those with chronic renal insufficiency.
We utilized the Habib in instances where we deemed avoidance of warm ischemia imperative. Patients with solitary kidneys or chronic renal insufficiency with large or centrally located (peri-hilar) tumors were considered good candidates.
Technique
The patients were placed in the standard flank position utilized for a majority of open renal surgeries. A retroperitoneal flank or subcostal incision was used to mobilize the kidney, the renal hilum, and tumor. Gerota's fascia was incised and the peri-renal fat was cleared from the tumor and surrounding kidney margin.
Once the tumor was exposed and intraoperative ultrasonography delineated the margins of the mass, the mass margins were lightly marked with cautery. The Habib device was then inserted into the margin of the mass circumferentially around the tumor. The Habib device must be inserted into tissue at a direct perpendicular angle to prevent renal parenchyma tearing or entry into the mass (Fig. 3). The device is activated with a foot pedal and the machine will notify the surgeon when the coagulation is complete with a beeping noise. The slow 75-W setting was used for the renal parenchymal tissue. Care should be taken at this step to avoid thermal spread of energy near the ureter.
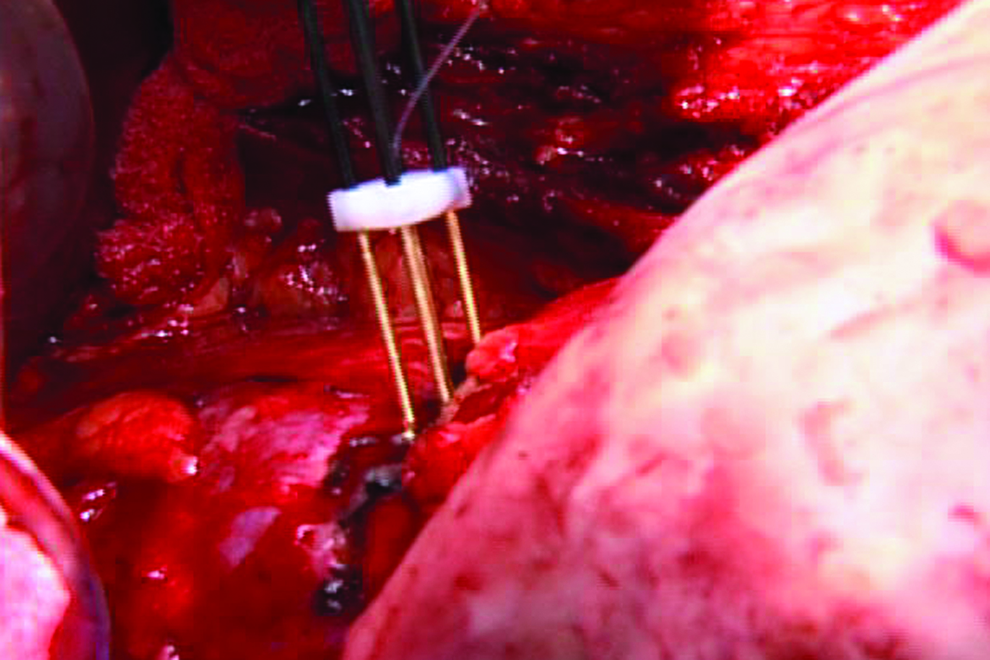
Habib device insertion. The Habib device is inserted into the tissue perpendicular to the tissue plane to prevent parenchymal tearing and entry into the tumor.
Once the coagulative zone is complete circumferentially around the tumor, the tumor is cut away from the kidney with a scalpel (Fig. 2). If done properly, a homogeneous avascular plane should be noted. The depth of necrotic tissue left behind is <10 mm. 8 Active bleeders in the resected bed should be oversewn with absorbable suture. Obvious collecting system violation should repaired with absorbable suture and a ureteral stent left in place as needed. A drain should remain in the retroperitoneum and removed once absence of urine leakage is confirmed. Postoperative care is similar to that of a standard open partial nephrectomy.
Results
We have used the device successfully in 4 partial nephrectomies (2 patients with solitary kidneys, 2 patients with bilateral masses). The mean age was 65 years. Mean tumor size was 6.4 cm. All tumors were located either in the upper pole or in the lower pole of the kidney. Mean hospital stay was 4.6 days. No patient received an intraoperative blood transfusion. Two patients required long-term ureteral stenting and surgical drainage for urine leakage.
Patient #1 was a 70-year-old man with a 6.6-cm right-sided tumor and chronic renal insufficiency. A preoperative renal scan demonstrated a poorly functioning left kidney (30% contribution). Surgical pathology demonstrated a 7-cm grade-2 papillary RCC with negative margins. The patient required no transfusions with an overall drop in his hemoglobin from 12.4 to 10.7. His JP drain was removed and he was discharged on POD 5.
Patient #2 was a 65-year-old man with a 7.8-cm left renal mass and a 10-cm right renal mass not amendable to partial nephrectomy. The final pathology showed a 6.5-cm grade-3 clear cell RCC with positive microscopic margins. The patient's hemoglobin went from 14.2 to 12.7 and no transfusions were required. The patient had to be taken to the operating room for left ureteral stenting secondary to a nonhealing urine leak. The patient was discharged POD 5. The patient's JP drain was removed 2 weeks after surgery. After right radical nephrectomy, the patient was noted to have metastatic disease. His left ureteral stent was exchanged, and he died 1 year after left partial nephrectomy.
Patient #3 was a 57-year-old woman with a 4-cm left lower pole renal mass and a right renal mass. The patient had numerous abdominal surgeries and was not considered a candidate for laparoscopic partial nephrectomy. Surgical pathology revealed a 4-cm grade-2 clear cell RCC with negative margins. No transfusions were required as her hemoglobin went from 14.3 to 9.9. Her JP drain was removed POD 3, and the patient was discharged home on postoperative day 4.
Patient #4 was a 65-year-old man with a solitary right kidney containing a 7-cm upper pole renal mass. Final pathology was a 7.0-cm clear cell RCC. The patient required no blood transfusions in the perioperative period but required ureteral stenting for urine leakage not amendable to conservative drainage. The ureteral stent was removed 3 months after surgery following retrograde pyelography confirming absence of urine leakage.
Discussion
Preservation of renal parenchyma via nephron sparing resection for RCC has been demonstrated to prevent long-term chronic renal insufficiency. 1 Cancer-specific survival rates of nephron sparing surgery have been demonstrated to be equivalent to radical nephrectomy. 10 Partial nephrectomy is widely considered the gold-standard nephron sparing treatment for RCC, but widespread utilization remains low, secondary to technical difficulty and increased risk of treatment-related morbidity such as blood loss. 2 The technical demands of partial nephrectomy such as renal artery clamping and increased operative time may influence physician treatment choice. Percutaneous cryoablation and RF ablation carry less short-term risk than partial nephrectomy, but their long-term cancer control data are still ill-defined and their use is limited to smaller renal masses (<3.5 cm). 11 Our series and Supplementary Video demonstrate the technique of partial nephrectomy for large renal masses not otherwise amendable to radical nephrectomy utilizing the Habib device for avoidance of warm ischemia. This is extremely beneficial in patients with solitary kidneys or in patients with bilateral renal masses, especially if one mass is not amendable to partial nephrectomy.
Bipolar RF energy has been utilized for other organ systems in the human body, mainly the liver. 6 Thus far, all studies looking at RF technology for partial nephrectomies have shown both efficacy and safety to be adequate.12–15 The generated temperature of 100°C by bipolar RF devices ensures tissue destruction, but it remains unknown if this increased temperature confers a treatment advantage over standard resection. 9
A recent prospective study comparing open partial nephrectomies with and without the Habib RF device found that use of the Habib RF device provided significantly less blood loss, avoided arterial occlusion, and decreased operative time due to the avoidance of arterial occlusion. 9 Although their average tumor size was only 3.31 cm, these benefits certainly should confer to larger tumors as operated at our institution. None of the operative complications noted in the study were definitively attributed to the RF device. We did not note any operative complications attributable to the Habib RF device, although we acknowledge that direct thermal spread to bowel or contiguous organs could be extremely dangerous if the technology is not used in a controlled fashion. The bowel should be dissected well away from the operative field before Habib application. The kidney should also be completely mobilized before device activation to avoid injury to structures behind the activation zone.
Two of our patients required long-term ureteral stenting for urine leakage that was not responsive to conservative management. Urinary fistulae are a known complication of partial nephrectomies with a reported incidence of 3%–6%. 16 A previous study has linked RF ablation energy with being a contributor to urinary fistula formation. 14 Resections of tumors over 2.5 cm are more than twice as likely to develop urinary fistulae postoperatively. 17 It is unclear if the coagulated tissue present in the resection bed prevented collecting system healing although it would contribute a strong theoretical risk.
The disposable Habib device costs $3,000 per case. 18 It is unclear how much cost advantage the Habib provided in our series with avoidance of blood transfusions or how much cost was added by the requirement of ureteral stenting secondary to urine leakage. Long-term savings may be noted if the nephron sparing procedures performed saved the cost of hemodialysis or subsequent kidney transplant assuming a radical nephrectomy had been performed.
We used this device successfully for select large partial nephrectomies to avoid prolonged periods of warm ischemia. Our indications for use are large bilateral tumors or large tumors in solitary kidneys where we believe that prolonged ischemia time may be harmful to the patient. Several recommendations can be made based on our experience. First, the electrodes should be inserted at right angle. The shaft of the instrument is rigid, so it is necessary to manipulate the kidney to achieve the optimal insertion angle. Second, certain vascular regions should undergo multiple heating cycles. Small arterial and venous bleeders are quickly and effectively coagulated, but larger arterial branches may require multiple coagulation cycles to control bleeding. Third, the ureter should always be protected to avoid potential damaging thermal spread. Lastly, we set the power to 75 W for kidney resections. While 125 W seals the smaller vessels faster, the slower 75 W setting promotes more meticulous hemostasis required for larger resections.
Conclusions
The Habib 4 × radiofrequency-assisted bipolar hemostatic device provides resection of select large renal masses without renal hilar clamping while demonstrating very little blood loss. Patient and tumor selection are of the utmost importance, and this technology may be beneficial in certain instances where warm ischemia is undesirable. Large areas of devascularization may contribute to an abnormally high urinary fistula rate.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.