
Abstract
Abstract
The standard endoscopic surgical approach in the management of laryngeal lesions is by the use of a laryngoscope, microscope, and laser. This requires the surgeon to work within the confines of the laryngoscope. At times, it requires repositioning of the laryngoscope and microscope to gain access to a specific area. The surgery also requires line-of-sight observation to complete the operation. The introduction of transoral robotic surgery in head and neck surgery brings the advantages of three-dimensional magnification, increased degrees of freedom with the effector arms, and an articulating distal end that mimics hand movements. To date, transoral robotic surgery of vocal cord surgery requires the use of a tracheostomy in patients. Here we report the use of a CO2 laser fiber and the Da Vinci robotic platform (Intuitive Surgical) for the surgical management of a T1 glottic squamous cell carcinoma.
Introduction
Transoral robotic surgery (TORS) has been documented to be safe in both cadaver experimentation and human application.2,3 The introduction of TORS in head and neck surgery brings the advantages of three-dimensional magnification, increased degrees of freedom with the effector arms, and an articulating distal end that mimics hand movements. We are presenting our case using a CO2 laser fiber and the Da Vinci robotic platform (Intuitive Surgical, Sunnyvale, CA) for the surgical management of a T1 glottic squamous cell carcinoma (SCCA).
Case Report
Patient 01 is a 73-year-old man who presented with hoarseness for 1 year. He has no other associated signs and symptoms, though he was a heavy smoker. He underwent a direct laryngoscopy and biopsy at another hospital, which revealed a moderately differentiated SCCA involving the left anterior two-thirds of the true vocal cord. His Eastern Cooperative Oncology Group (ECOG) performance status was 0 and he did not have any associated co-morbidities. He refused radiation therapy and was referred to our service for surgical management. Office nasopharyngoscopy confirmed a mobile left vocal cord with the above-mentioned findings (Fig. 1). The rest of the head and neck examination was unremarkable. Positron emission tomography–computed tomography scan showed no adenopathy or distant metastasis, and he was thus classified as T1a No Mo Stage 1. His case was presented in the multidisplinary head and neck conference at Greater Baltimore Medical Center. Given that he did not want radiation therapy, we offered the options of traditional transoral laser surgery, TORS, and open laryngeal surgery. The patient opted for TORS and consented for the procedure under an IRB-approved protocol.
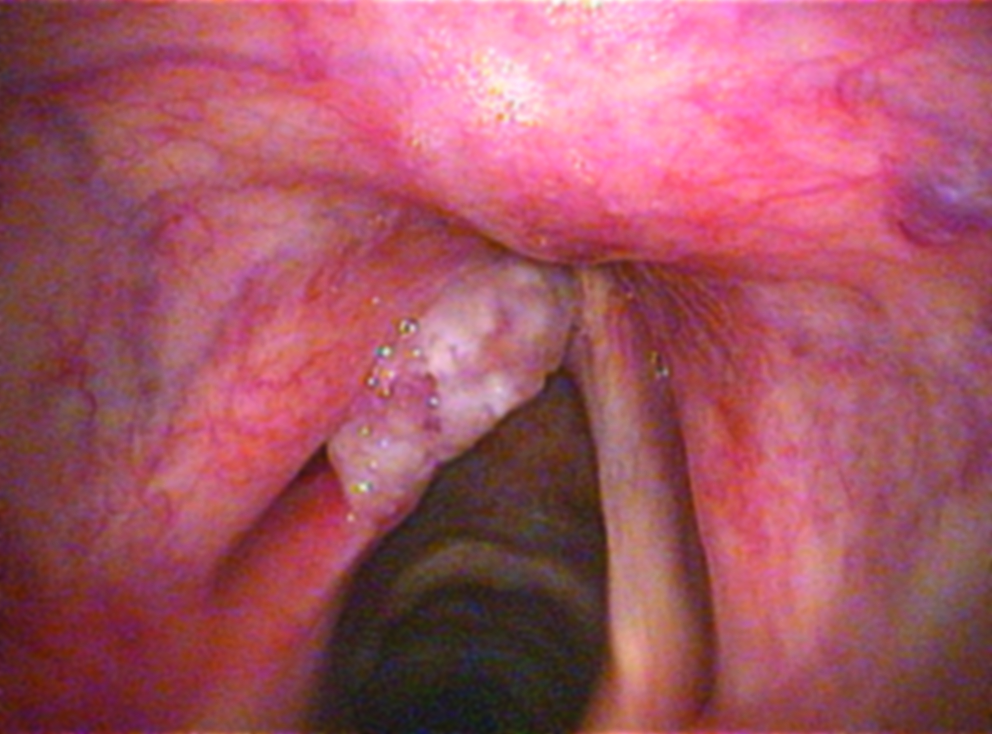
Left vocal cord squamous cell carcinoma.
Procedure
The patient was intubated using a size-6 laser endotracheal tube that was anchored at the nasolabial fold. The patient's head was hyperextended using a soft shoulder gel. Eye pads were placed over both eyes, and a head drape was secured. The patient was edentulous and the lips were protected with mouth guards. Direct laryngscopy revealed no other associated mucosal lesions. The tongue was retracted anteriorly using a silk 2-0 U stitch. The Da Vinci robotic platform was positioned 30° to the right of the patient. An Omni-Guide (Cambridge, MA) laser fiber was anchored to the left 5 mm effector arm without cautery tip using a French 16 cut red rubber. This was attached to the tip of the instrument. The right effector arm was a 5-mm Maryland dissector. The tongue was retracted anteriorly, and using a malleable blade, we retracted the tongue base until we could observe the tip of the epiglottis. Both arms were docked at 45° with both robotic arms placed beside the laser tube with both articulating segments of the arm at the supraglottic area. We then used a Lindholm laryngoscope to retract the epiglottis. Both articulating segments of the right and left arms were observed, and the Lindholm scope was suspended. The camera was placed through the Lindholm scope. Of note, both the effector arms were situated outside and lateral to the Lindholm scope. It took us 35 minutes to set up and dock the robot. We proceeded to resect the left false cord for better observation (Fig. 2). The left vocal SCCA was then resected using the laser fiber at 14w (Fig. 3). The resection time was 10 minutes. The frozen section and final pathology report of the margin was negative for tumor (Fig. 4). The patient tolerated the procedure well, and he was admitted for a 23 hours of observation and subsequently discharged. On postoperative day 5, a nasopharyngscopy examination was done, which showed the expected degree of wound healing (Fig. 5).
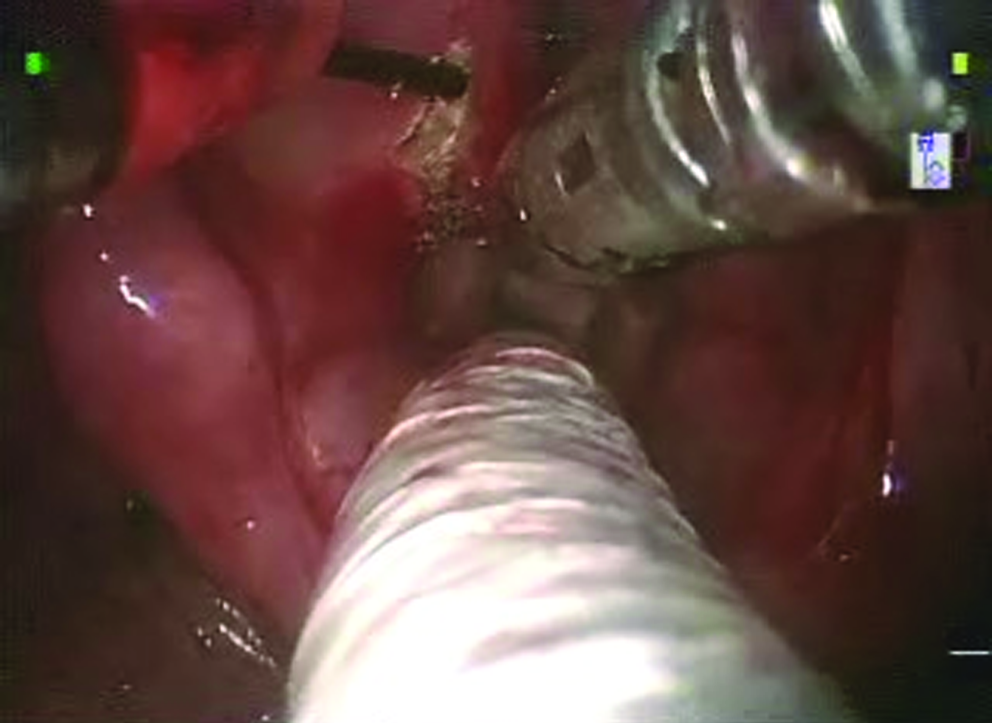
Resection of left false cord.

Resection of left vocal cord squamous cell carcinoma using transoral robotic surgery with laser fiber.
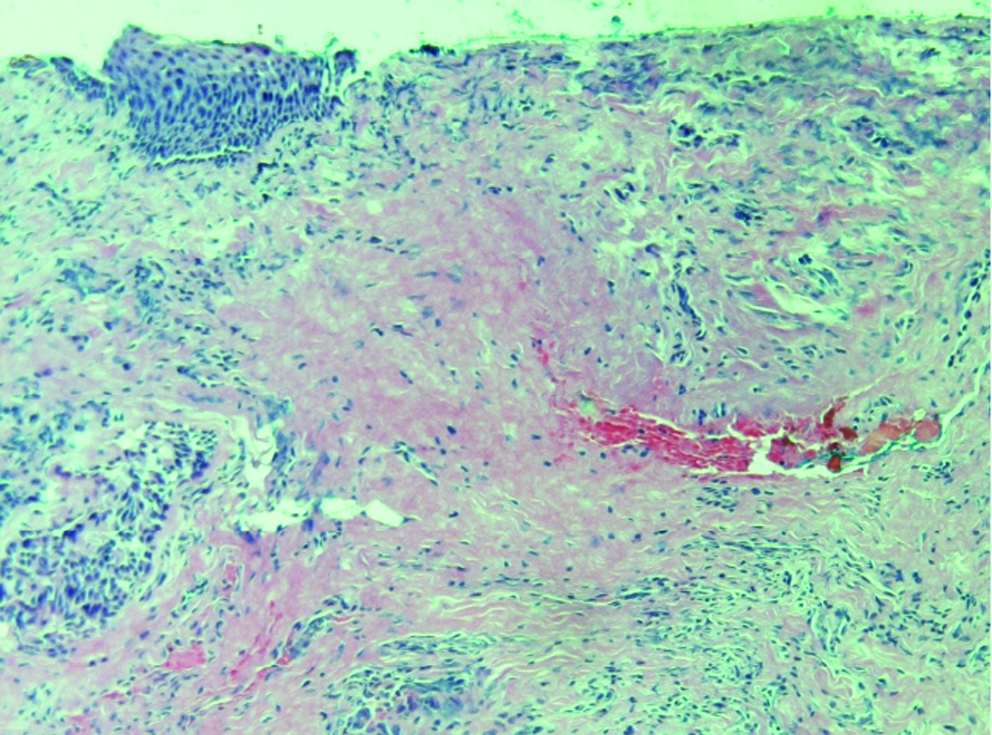
Hematoxylin and eosin stain. Negative margin on final pathology report.
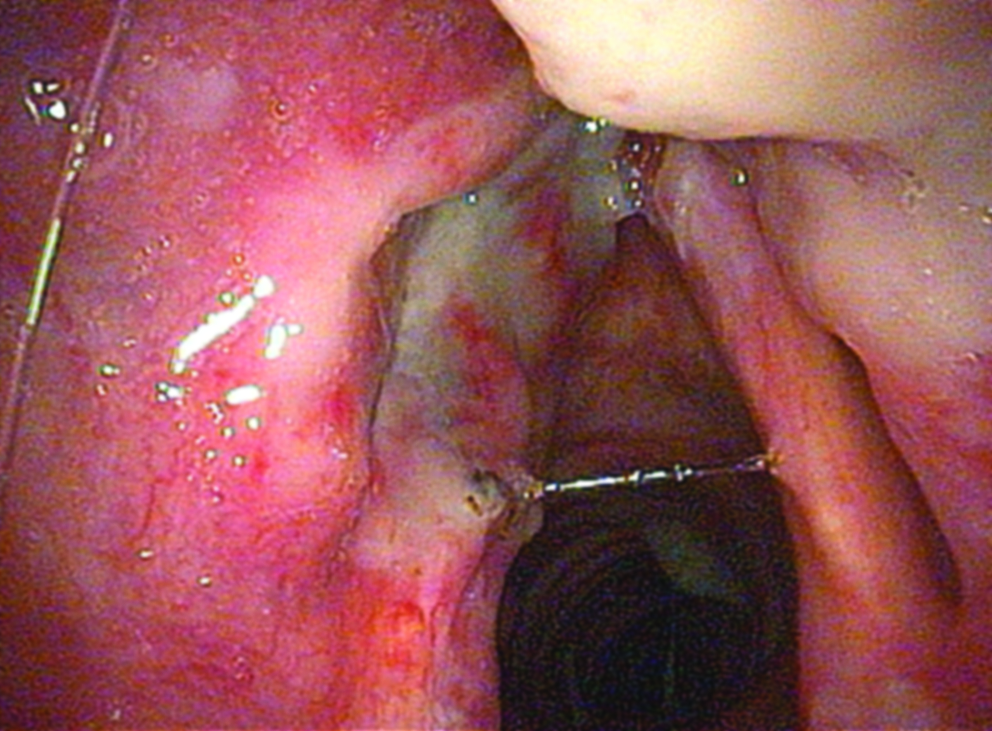
5th postoperative day.
Discussion
Adequate exposure and instrumentation remain significant challenges in transoral surgery for head and neck tumors. Although the applicability of TORS in vocal cord surgery remains debatable, Weinstein and O'Malley reported on the use of TORS in the vocal cord in canine models. 4 Park and associates used cautery-assisted TORS in the resection of vocal cord lesions in 3 patients, securing their airway with a tracheostomy. 5 In our case the airway was secure and did not require tracheostomy. There has also been documentation of the applicability of TORS of in a pediatric airway case. 6
The FK retractor has been used in exposing both the supraglottic and glottis area for TORS.7,8 We opted not to use this because the FK frame can limit the 45° entry of the effector arms and we needed an instrument to retract the epiglottis. Although the new generation of a wider FK retractor and accessory for TORS could also obviate the above-mentioned concern, we preferred the Lindholm scope because of this configuration. It can be adapted to retract the epiglottis and have enough distal working space for the articulating 5-mm robotic arms. Rahbar et al. had reported the use of laryngoscope with TORS on pediatric airway. 6 We did not find any visual limitation when the camera was inserted into the Lindholm scope since it exposed the operative area and provide an excellent path for the camera to be inserted. With the magnification of the Da Vinci three-dimensional camera, we rarely needed to change camera to a 30° scope or make gross movements for improved observation. We noted that a change of a millimeter of movement of the camera was sufficient to observe the area of interest. Further, we did not encounter any collision with the Lindholm scope. Our other observation was that once the distal articulating arms were in the field, there was little need for gross lateral or medial movements of the arms to successfully complete the case. We were able to easily change the angulation of our laser beam without difficulty with laser fiber attached to the effector arm. Because of the tremor filter built into the system, our movements and laser aiming on the vocal cord were very fine. With the second assistant performing the suctioning and retracting, we able to use the right arm to retract and expose the anterior commissure without changing position or instrumentation.
As TORS technology and instrumentation continues to improve, the use of TORS on glottic tumors is increasingly feasible. Improvement of distal articulating instruments for microlaryngeal work will increase the precision in laryngeal surgery. Microvascular robotic instruments were also reported to be feasible and have been tested in animal models. 9
The reported acceptable margin is 1–3 mm in vocal cord cancer. 10 In this case our margin was 2 mm from the tumor. With this technique we were able to resect the tumor in one piece rather than in a piecemeal fashion. Different laser fibers with their respective advantages are now available and can easily be adapted to one of the robotic arms as reported by Solares and Strome 11 and Desai et al. 12
With the increased degree of mobility of the TORS instrumentation, no line-of-sight limitation, improved instrumentation, and flexible laser fibers, TORS will continue to develop and be one of the significant tools in the surgical armamentarium in the treatment of laryngeal tumors.
Footnotes
Acknowledgments
James J. Scuibba, DMD, PhD
Richard Hirata, MD, FACS
Disclosure Statement
No competing financial interests exist.