
Abstract
Abstract
Introduction:
The antegrade continence enema procedure offers convenient enema administration for patients with fecal incontinence and can be performed by a minimally invasive approach that provides shorter hospital stay, less analgesia requirement, and better cosmesis. We present our experience using this approach for fecal incontinence patients and technical modifications to reduce complications.
Methods:
Following successful management of fecal incontinence through bowel management using a daily rectal enema, 44 patients underwent a laparoscopic-assisted Malone appendicostomy procedure. We reviewed the diagnosis underlying the fecal incontinence, operative technique, duration of surgery, length of hospital stay, and postoperative complications.
Results:
The mean age at surgery was 8.6 ± 1.0 years. The diagnoses included anorectal malformations (31), idiopathic constipation (6), Hirschsprung disease (3), and others (4). All the patients underwent a V-V umbilico-appendicoplasty. The cecum was plicated around the base of the appendix in 34 patients (77%); this step was omitted in 10 (23%). The median follow-up was 21 months (range: 3–51 months). Twelve complications were recorded in 9 patients (20.5%)—leakage from the stoma in 1 (2.3%), stomal stenosis in 5 (11.4%), and a combination of both in 3 (6.8%)—with an overall stricture rate of 18.2% (8/44) and leakage rate of 9.1% (4/44). Strictures were managed with minor operative revision. Plicating the cecum was associated with a lower leakage rate compared with the nonplicated group (0/34, 0% versus 4/10, 40%; P = .002). All patients were consistently clean between enemas following their antegrade continence enema procedure.
Conclusions:
The umbilical appendicostomy provides a convenient and cosmetic location for enema administration. Cecal plication, which is feasible using a laparoscopic-assisted approach, significantly reduces the leakage rate. Stomal stenoses remains a problem, may be lessened by a V-to-V umbilical to appendix anastomosis, and are easily fixed with a revision.
Introduction
Materials and Methods
Six hundred fifty-four patients participated in our bowel management program for the treatment of fecal incontinence over the last 4 years. A total of 280 patients underwent an ACE procedure after a successful rectal enema regimen was developed. In this regard, success was defined as being clean in the underwear between daily enema administrations. The appendicostomy procedure was performed using an open approach in 235 patients and a laparoscopic or laparoscopic-assisted approach in 45 patients. We reviewed the charts of 44 patients who underwent a laparoscopic-assisted ACE procedure between November 2005 and December 2009 (a patient who had a laparoscopic-assisted neoappendicostomy was excluded from the study).
The patients were admitted on the morning of the procedure in most cases or the day prior to surgery when the ACE was performed together with other procedures requiring a more intensive bowel preparation (e.g., redo posterior sagittal anorectoplasty).
The procedure involved making a V-shaped incision at the umbilicus (Fig. 1) for the camera port (5 mm) and for two other ports (5 mm) for the surgeon's right and left hand. Often, these could be placed in previous abdominal incisions. The cecum is mobilized off the retroperitoneum and the appendix is brought out through the umbilical port. The fascia inferior to the umbilical incision is extended and the cecum is delivered out of the incision. The cecum is then plicated around the appendix using 5-0 silk to create a valve-like mechanism (Fig. 2), without compromising the blood supply of the appendix. In some patients, plication was omitted because it was thought that the appendix was long enough to prevent leakage of cecal contents, and in these patients, the fascia below the umbilical incision was not incised. The appendiceal tip is sutured to the skin in a V-to-V technique using 6-0 vicryl sutures (Fig. 3). An 8F feeding tube is left in place and secured to the skin of the anterior abdominal wall with a suture (Fig. 4). The patient is fed orally usually the next day and enemas are then administered through the tube. Following discharge, the patients are seen in clinic at 2 weeks postoperatively when the tube is removed for the first time. The patient and their parents are then taught the technique of insertion and removal of the catheter. Further follow-up is done using a combination of e-mail correspondence and clinic visitation, which is handled by our specialized colorectal nurses working in a center-based approach to care.

A V-shaped umbilical incision is made for the introduction of the camera.
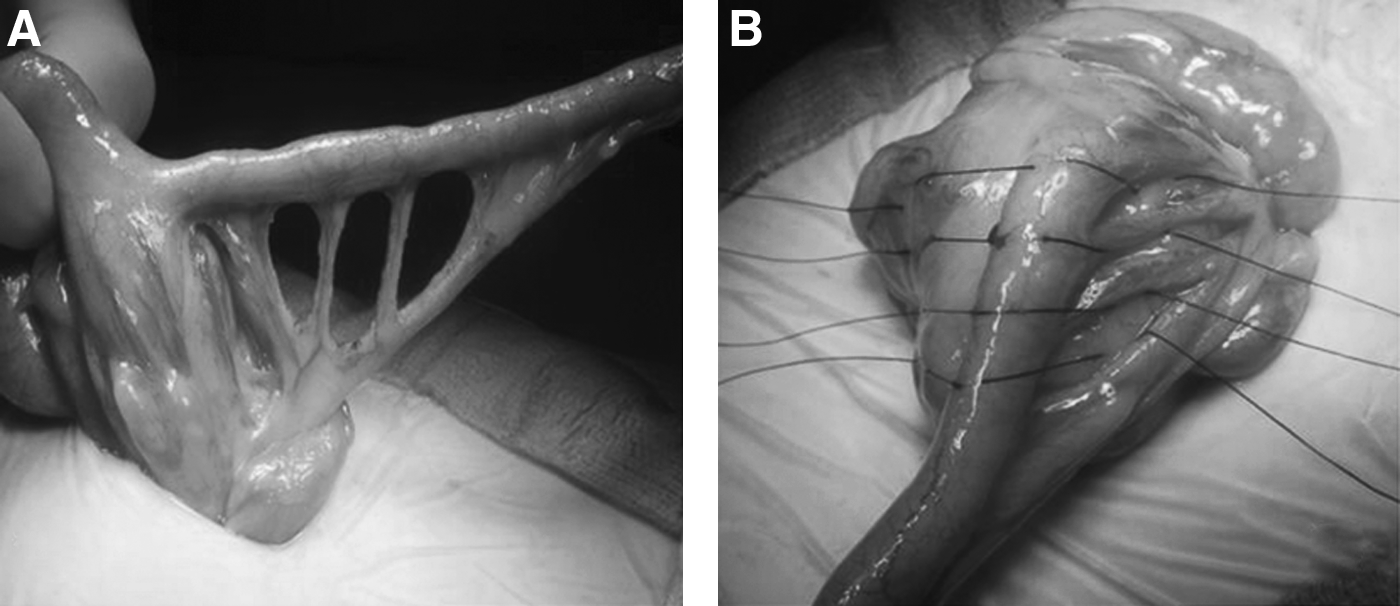
The cecum is plicated around the base of the appendix using silk sutures.
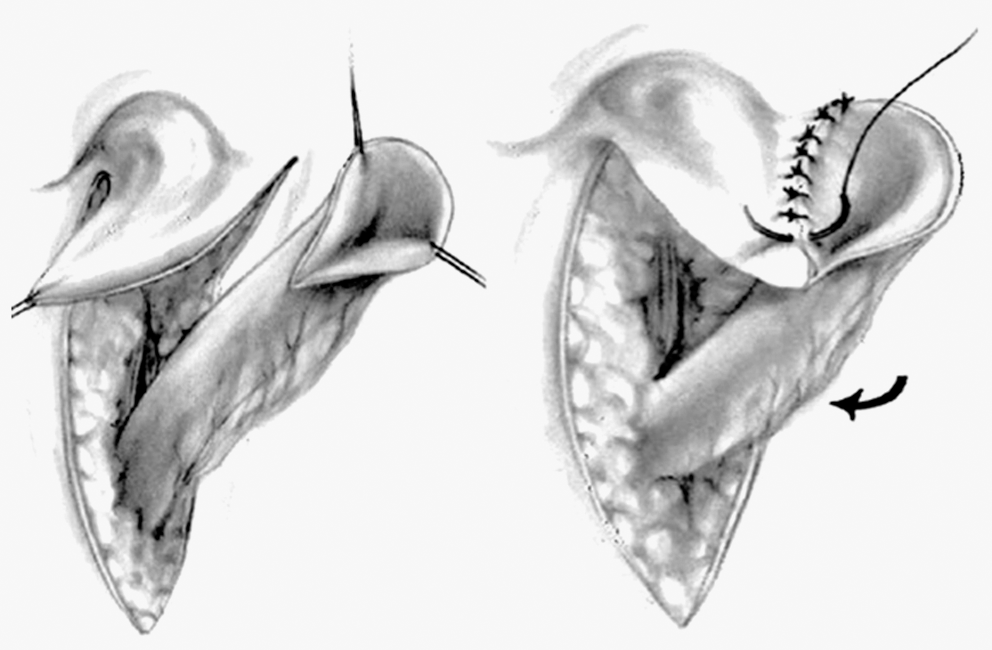
The tip of the appendix is sutured to the umbilical flap in a V-to-V technique.
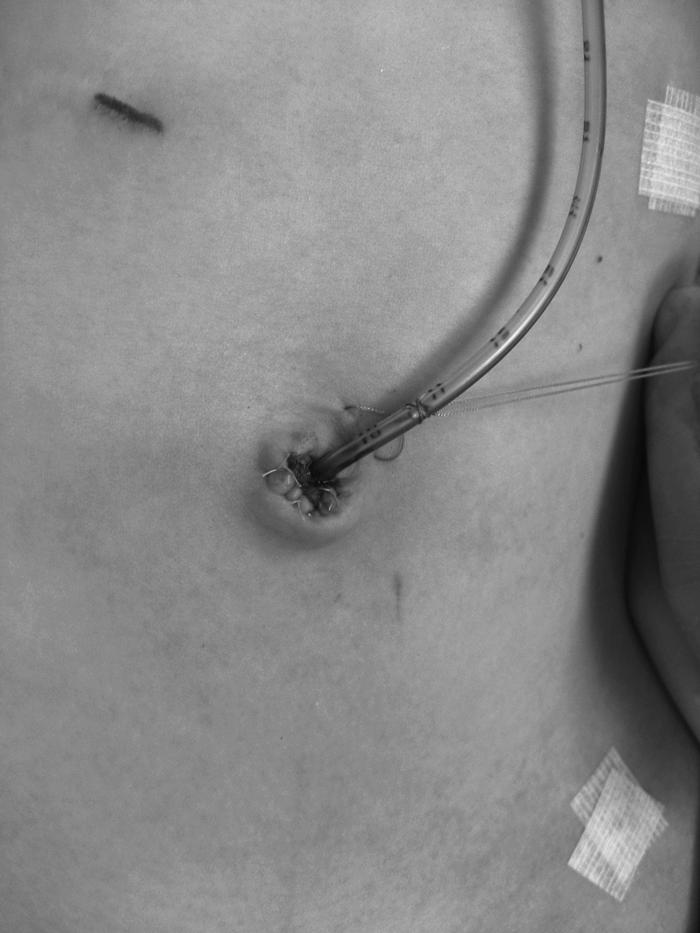
An 8F tube is left in place and secured to the anterior abdominal wall.
We reviewed the diagnosis leading to fecal incontinence, operative technique, duration of surgery, length of hospital stay and associated complications for all patients who underwent a laparoscopic ACE procedure. Statistical analysis was done using SAS v. 9.1 (SAS Institute, Cary, NC) and we did a contingency analysis of the differences observed between the plicated and nonplicated groups with Fisher's exact test. The Student's t-test was used to compare the differences between the operation times and length of hospital stay.
Results
Forty-four patients underwent a laparoscopic-assisted ACE procedure over the 4-year study period. There were 27 boys and 17 girls. Their mean age was 8.6 ± 1.0 years. Thirty one (70%) had fecal incontinence related to their ARM. The other indications for the ACE procedure were idiopathic constipation (6 patients), Hirschsprung disease (3), spinal cord injury (2), myelomeningocele (1), and spina bifida (1). Forty of the 44 patients (91%) are active, with normal physical activities. All of the patients participated in our bowel management program prior to their procedure and were successfully clean with a retrograde enema. 1 The cecum was plicated around the base of the appendix in 34 patients (77%), whereas in 10 patients (23%) a plication was not done. All the patients had a V-V appendicoplasty performed at the umbilical anastomosis. The median operative time was 67 minutes (range: 37–94 minutes). The operative time was not significantly different between patients who underwent a cecoplication and those who did not (65.2 ± 3.4 versus 56.4 ± 4.2 minutes, respectively; P = .1669).
In the overall group, the median length of hospital stay was 2 days (range: 1–5 days). The length of hospital stay was significantly shorter in the nonplicated group (1.7 ± 0.2 versus 2.8 ± 0.2 days; P = .0057). There were no perioperative complications of surgery or anesthesia. The median follow-up was 21 months (range: 3–51 months). Twelve complications occurred in 9 patients (20.5%)—1 patient (2.3%) had intermittent leakage from the stoma, 5 (11.4%) had stomal stenosis, and 3 (6.8%) had both stenosis and intermittent leakage. The overall stricture and leakage rates were 18.2% (8 of 44 patients) and 9.1% (4 of 44 patients) respectively. One of the 8 cases of stricture occurred in a patient in whom the catheter was passed into the lateral wall of the appendix, resulting in a false passage and subsequent stricture. The mean interval between surgery and development of a stricture was 4.6 ± 0.5 months. Cecoplication was associated with a reduction in the leakage rate when compared with nonplication [0% (0 of 34 patients) versus 40% (4 of 10 patients); P = .002]. The patients with strictures or leakage underwent revisions, a minor same-day surgical widening of the orifice, or for leakage, plication of the appendiceal base. We have also used interventional radiology guidance to dilate the strictures (in 2 cases) and avoided the need for reoperation in 2 patients.
We found that having had a previous laparotomy does not hinder the ability to perform a laparoscopic-assisted ACE, as 33 patients (75%) have had previous laparotomies. The median number of previous laparotomy/laparoscopy that the patients had undergone was 2 (range: 0–7).
All 44 patients who underwent a laparoscopic ACE procedure have remained free from soiling between enemas.
Discussion
The use of ACEs in the management of fecal incontinence has been associated with a high level of satisfaction, improvement in self-esteem, and overall quality of life of patients.5,6,11 In the original description of the ACE, Malone, using an open technique, amputated and reversed the appendix, reimplanted it into the cecum, and created a stoma in the right iliac fossa. 7 In 1997, we reported our preliminary series of 20 patients, who underwent an ACE procedure with our modifications such as leaving the appendix in situ, anastomosing the appendiceal tip to the umbilicus, and, for patients who have had a previous therapeutic or incidental appendectomy, creating neoappendicostomy flaps. 6 We have found that the use of the umbilicus as the catheterizable orifice has an excellent cosmetic advantage (Fig. 5) and interferes minimally with the daily activities of the child.6,12

The appearance of the umbilical stoma a few weeks after the procedure.
We have also described our experience with a comprehensive bowel management program and have noted the use of an ACE as an adjunct to successful bowel management.1,13 Many reports write about a “cure for fecal incontinence” using the ACE but this is not accurate. It does not obviate the need for a proper bowel management protocol, which was the reason that patients in this series were successfully clean 100% of the time on daily rectal enemas prior to being considered for the ACE procedure. The critical element for successful bowel management is the correct enema, not the route of administration.
There are reports that laparoscopic ACE has been used by numerous authors for patients with fecal incontinence.10,14–18 It offers a minimally invasive approach to localization of the appendix, cecal mobilization, and bringing the appendix to the abdominal wall for the appendicoplasty. The major advantages include shorter hospital stay, improved cosmesis, and fewer complications.10,14 It also offers an avenue to simultaneously perform procedures such as inspection of internal reproductive anatomy in a patient with rectovestibular fistula and absent vagina and in those with cloacal anomalies. 19 A major constraint is the ability to perform cecal plication, but a suitable option is the technique of laparoscopic-assisted ACE, in which the appendix is mobilized to the umbilicus and cecal plication is performed via an infraumbilical fascial incision. 20 We found from this review that the addition of cecoplication does not significantly prolong the operative time. This contrasts with a doubling of the operative time noted in another series when cecal plication was performed and discouraged. 14 Perhaps, with more experience, the time needed to complete the procedure can be shortened. The length of stay in our series was longer in the plication group, by 1 day, perhaps because of edema of the cecum, which may delay return of bowel function.
In literature, the most common complications of the ACE procedure include strictures, leaks, stomal necrosis, flap necrosis, appendiceal false passage, and intestinal obstruction.6,14,18,21,22 The reported stricture rate following laparoscopic ACE with an umbilical stoma has ranged from 0% to 38%.15,18,21,22 Although technical modifications such as Y-appendicoplasty 12 and the V-to-V umbilical anastomosis have contributed to lowering the stricture rate, the wide variation is also due to different classification of what constitutes a stricture 22 as well as the threshold of the individual surgeon to repair the problem. There is a low threshold in this series, with a stricture rate of 18%, to reoperate once there is difficulty catheterizing the stoma. Leaving the catheter for a longer duration or more frequent catheterizations are helpful when the fibrosis is minimal. A less-invasive option that may work is to have patients undergo dilation by interventional radiology.
Leakage of fecal contents through the stoma is the second major complication of the ACE procedure. The rates reported in the literature vary widely as well, ranging from 0% to 40%.11,14,16,23,24 Leakage rates depend on the volume of enema, frequency of enema administration, patient characteristics, and the liquidity of the stool.6,11,16,17,23 The main measure that has been employed to reduce leakage is performing a cecal plication. Leakage rates with cecal plication range from 7% to 22%.14,23 In the present series, we had no leakage with cecal plication.
Some authors suggest that plication is not necessary,14,16,25 but our findings differ. Plication has been omitted by some, in a bid to reduce the operative time and perform the procedure entirely laparoscopically.14,16 Nanigian and Kurzrock retrospectively reviewed 22 patients who underwent a laparoscopic ACE procedure, without cecal plication, and reported no leakage at a mean follow-up period of 24 months. It was thus suggested that plication was unnecessary. 16 Similarly, Koivusalo et al., in a comparison of open ACE (with cecal plication) and laparoscopic ACE with or without cecal plication, in a population consisting mostly of patients with myelomeningocele, reported no leakage in the group who underwent laparoscopic ACE without cecal plication compared with three leaks in 14 patients (21%) who had laparoscopic ACE and cecal plication and three leaks in 11 patients (27%) who had undergone an open procedure. 14 This contrasts with the 40% leakage rate in the absence of plication in our series. A possible reason for this difference is patient selection. In the study by Nanigian and Kurzrock, 20 of the 22 patients have relatively reduced physical mobility (spina bifida, 19; muscular dystrophy, 1) and only 1 had undergone previous abdominal surgery. 16 Conversely, in our study, 40 of 44 patients (91%) are active, with normal physical activities and the majority (33 patients, 75%) have had previous laparotomies. The anterior abdominal wall characteristics are therefore different. Others have suggested that patient factors relating to gastrointestinal motility may be important to the success of the ACE.18,26 Kim et al., in a review of 74 patients who underwent a laparoscopic ACE, found a surgical ACE revision rate of 63% in patients with ARMs compared with a 14% revision rate in patients with other diagnoses such as spina bifida (P = .005). 18
Other complications noted in the literature, including intestinal obstructions, flap necrosis, and stomal necrosis, were not encountered in this series.
This is the largest series, to date, of laparoscopic (assisted) ACE procedures in patients with ARM and fecal incontinence. We found that the umbilical appendicostomy provides a convenient and cosmetic location for enema catheterization. Laparoscopic-assisted ACE produces a satisfactory route for enema administration in children with ARM and fecal incontinence. Cecal plication, which is feasible using a laparoscopic-assisted approach, significantly reduces the rate of leakage of fecal content via the stoma in between enemas. Stomal stricture may be related to patient factors, may be reduced by a V-to-V technique, and, when it occurs, is easily repaired with a local revision.
Footnotes
Disclosure Statement
No competing financial interests exist.