
Abstract
Abstract
Aim:
The aim of this study was to compare the safety of laparoscopic operation with open surgery for choledochal cyst in children.
Methods:
Early outcomes of open surgery from January 2001 to December 2006 were compared with early outcomes of laparoscopic operations from January 2007 to July 2010. The main outcome variables included intra- and early postoperative complications, operative time, rate of reintervention, and duration of postoperative stay.
Results:
There were 307 patients in the open operation group and 309 patients in the laparoscopic operation group. There was no significant difference in cyst diameter between the 2 groups. The operative time was longer in the laparoscopic operation group. The number of patients requiring blood transfusion was lower in the laparoscopic operation group. Intraoperative complications were low in both groups and not significantly different. The rate of postoperative complications was lower in the laparoscopic operation group but not significantly. The rate of reintervention was significantly lower in the laparoscopic operation group. The postoperative stay was significantly shorter in the laparoscopic operation group.
Conclusion:
Laparoscopic operation is as safe as open operation for choledochal cyst. The postoperative stay was significantly shorter in the laparoscopic operation group.
Introduction
The aim of this study was to compare the safety of laparoscopic operation with the open approach, based on the rate of intraoperative and early postoperative complications.
Materials and Methods
Criteria for inclusion
Open operation group
Patients with choledochal cyst with type I or IV according to the Todani classification underwent operations from January 2001 to December 2006 at the National Hospital of Pediatrics, Hanoi, Vietnam.
Laparoscopic operation group
Patients with choledochal cyst with type I or IV underwent operations from January 2007 to July 2010 at the same hospital.
Criteria for exclusion
Patients with a perforated cyst in the open operation group (15 patients) were excluded. Laparoscopic operation is not indicated for perforated cysts.
The open operations were performed by one of four senior hepatobiliary surgeons. Two surgical techniques were used in the open operation group: cystectomy and Roux-en-Y hepaticojejunostomy, 1 and cystectomy and jejunal interposition hepaticoduodenostomy. 20
The laparoscopic cystectomy was performed by one of four senior laparoscopic surgeons. The hepaticoduodenostomy or Roux-en-Y hepaticojejunostomy was performed by the same senior surgeon. The laparoscopic techniques have been described in two previous reports.21,22
Oral feeding was initiated on the third postoperative day after fluid from a gastric tube was clear. The abdominal drain was removed on the fifth day if there was no biliary leakage.
The main outcome variables were intraoperative and early postoperative complications, including injury to portal vein, hepatic arteries, or hepatic ducts; bilio-digestive anastomotic leakage; abdominal abscess; intestinal obstruction; abdominal wound dehiscence; need for reintervention; and mortality. We also compared operative time and duration of postoperative stay.
Sample size
Using the rate of early complications in open operation (9.3%) 23 and the expected rate of early complications in laparoscopic operation (18.6%) with a significance level of 5%, and 90% power, at least 290 patients were needed in each treatment arm to provide a reasonable likelihood of statistical significance.
Analysis
Data were analyzed using SPSS 15.0. The chi-square test was used for categorical variables and Student's t test was used for continuous variables. A P value of <.05 was considered statistically significant.
Results
Totally, 616 patients were included in the study. Three hundred nine patients underwent laparoscopic operation from January 1, 2007 to July 13, 2010, including 192 patients with cyst excision and hepaticoduodenostomy, 115 with Roux-en-Y hepaticojejunostomy, and 2 patients requiring conversion to open surgery. The open operation group included 307 patients from January 1, 2001 to December 30, 2006. Two hundred sixty-one patients underwent cyst excision and Roux-en-Y hepaticojejunostomy and 46 patients underwent a jejunal interposition hepaticoduodenostomy.
Clinical characteristics of these 616 patients are presented in Table 1.
The mean age of patients was younger in the laparoscopic operation group than in the open operation group (48.7±2.3 months versus 63.5±2.9 months, P=.001).
Mean choledochal cyst diameter was not significantly different between the 2 groups (47.8±1.5 cm versus 47.6±1.5 cm, P=.89).
The rate of associated dilatation of the intrahepatic biliary tract was not significantly different between the 2 groups (40.4% versus 41.7%, P=.7).
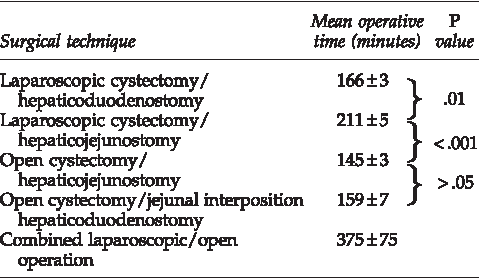
Mean operative time was significantly longer in the Roux-en-Y laparoscopic operation group in comparison with the open Roux-en-Y hepaticojejunostomy group (211 minutes versus 145 minutes, P<.001). Mean operative time according to surgical technique is presented in Table 2.
Ten patients (3.2%) in the laparoscopic group required intraoperative blood transfusion versus 34 patients (11.1%) in the open operation group. The difference is statistically significant (P=.001).
Two patients in the laparoscopic operation group had intraoperative complications (1 patient had injury to the right portal vein and 1 patient had injury to the right hepatic duct). The small perforations of portal vein and hepatic duct were laparoscopically closed successfully. One patient in the open operation group had injury to the right hepatic artery.
Postoperative evolution was more favorable in the laparoscopic operation group (Table 3).
Twelve patients (3.9%) in the complete laparoscopic operation group had postoperative complications, whereas 17 patients (5.5%) in the open operation group had postoperative complications (Table 4). The difference is not statistically significant (P=.3). Seven patients in the complete laparoscopic operation group had bile leakage: 3 patients in 2007, 2 patients in 2008, 1 patient in 2009, and 1 patient in 2010. Six patients in the open operation group had bile leakage. The rate of bile leakage between different operative techniques was not significantly different. Only 1 patient in the laparoscopic group had postoperative bleeding, whereas 5 patients in the open operation group had postoperative bleeding (Table 4).
One patient (0.3%) in the complete laparoscopic operation group required reintervention versus 11 patients (3.6%) in the open operation group. The difference is statistically significant (P<.01).
Mean postoperative stay was 7.0±0.2 days for the laparoscopic group versus 9.1±0.2 days in the open operation group. The difference is statistically significant (P=.001).
The intraoperative and postoperative complication rates were not significantly different between the laparoscopic Roux-en-Y hepaticojejunostomy group and the open Roux-en-Y hepaticojejunostomy group. However, the reintervention rate was significantly lower in the laparoscopic Roux-en-Y hepaticojejunostomy group (Table 5).
There were no deaths in either group.
Discussion
Our study revealed that intraoperative complications were not significantly different between laparoscopic operations and open operations. However, the number of patients requiring blood transfusion during operation was significantly lower in the laparoscopic operation group.
Injury to portal vein and hepatic arteries is the main concern during cystectomy, especially in laparoscopic cystectomy. These complications happened in only 1 patient in our laparoscopic group, because of severe adhesions. Dissection close to the cyst wall is mandatory to avoid this complication.
Total early complications were not significantly different between the 2 groups. Postoperative bleeding was less frequent in the laparoscopic group, although expected frequencies are too small for reliable statistical analysis. Recognition of bleeding and subsequent hemostasis seems to be a better option, using magnification with the laparoscope.
The rate of bilio-digestive anastomotic leakage is a common complication of surgery for choledochal cyst, with rates reported from 5.8% to 7.3% in open operation.23,24 In our study, bile leakage was not significantly different between the 2 groups (0.22% versus 0.20%). Anastomotic leakage in the laparoscopic group decreased with learning curve. The rate of bile leakage in 2009 and 2010 was very low.
Reintervention was significantly less frequent in the laparoscopic operation group. Only 1 patient in the laparoscopic group required reintervention because of bile leakage. The main reasons for reintervention in the open operation group were abdominal abscess and bleeding.
Total early complications and mortality rate in our laparoscopic operation group were significantly lower than in the open operation series reported by Li et al. (Table 6).
The rate of early postoperative complications in laparoscopic operation for choledochal cyst was also low in other series.3–8,11,15 Abdominal wound dehiscence has occurred in open operations but has not been encountered in laparoscopic operations.4,5,10,11,23
Our overall mean operative time was significantly longer in the laparoscopic group. The mean operative time of laparoscopic cyst excision and Roux-en-Y hepaticojejunostomy was 66 minutes longer in the laparoscopic operation. However, it was only 21 minutes longer in laparoscopic cyst excision and hepaticoduodenostomy in comparison with open Roux-en-Y hepaticojejunostomy (Table 2).
Postoperative recovery was more favorable in the laparoscopic group, with significantly shorter duration of postoperative infusion, shorter duration from the operation to occurrence of flatus, and shorter duration of drain placement.
The mean postoperative stay was significantly shorter in the laparoscopic operation group than in the open operation group.
There were no significant differences between the laparoscopic Roux-en-Y hepaticojejunostomy group and the open Roux-en-Y hepaticojejunostomy patients in terms of intraoperative blood transfusion, intraoperative complications, and postoperative complications. However, the reintervention rate was significantly lower in the laparoscopic group (Table 5).
Our study allows us to conclude that the laparoscopic operation is as safe as open operation for choledochal cyst. Moreover, recovery and hospital stay were shorter and the cosmetic result is superior.
Footnotes
Acknowledgment
The authors thank Dr. John Taylor, Clinical Associate Professor, Department of Pediatrics, School of Medicine, University of Washington, for his careful reading and valuable comments on the manuscript.
Disclosure Statement
No competing financial interests exist.