
Abstract
Abstract
Background:
The current hemostatic data in relation to laparoscopic cholecystectomy (LC) is limited particularly for patients receiving chronic oral anticoagulant treatment. The aim of this study is to assess hemostatic alterations before, during and after LC for the patients placed on long-term oral anticoagulant treatment.
Patients and Methods:
A prospective, nonrandomized, controlled study was designed to compare the characteristics, hemostatic system, and postoperative complications of patients maintained on long-term anticoagulation with those who did not receive such therapy. In the period from January 2009 to December 2009, a total of 31 patients who underwent elective LC for symptomatic cholelithiasis were enrolled in the study. Sixteen of these patients were on long-term anticoagulation therapy with warfarin (OAC group). The other 15 patients did not receive anticoagulant or antiaggregant drugs and served as the control group.
Results:
Five patients (31.5%) of the OAC group had postoperative bleeding, whereas no bleeding occurred in the control group. Significant reductions in postoperative hemoglobin levels were observed in the OAC group when compared with the control group (P<.05). Although within normal ranges, international normalized ratio values and the tissue plasminogen activator activity were significantly higher, whereas factor II, VII, IX, and X levels were significantly lower in the OAC group when compared with the control group (P<.05).
Conclusion:
Patients receiving oral anticoagulant treatment are at risk of postoperative bleeding and the basic parameters of coagulation appear unable to predict which patients undergoing anticoagulant therapy are candidates for bleeding after surgery. More sensitive methods should be developed to measure the degree of hemorrhagic risk.
Introduction
Patients on long-term anticoagulation therapy represent a challenging subset when surgical intervention is required. The continuation of full anticoagulation throughout surgery increases the risk of bleeding, and interrupting the anticoagulant therapy increases the risk of thromboembolism and prosthetic valve thrombosis.9,10 There is little consensus regarding optimal perioperative treatment for patients on such therapy. The general approach is the replacement of oral anticoagulants with unfractionated heparin (UHF) or low-molecular-weight heparin (LMWH) a few days before surgery to lower the international normalized ratio (INR) values below 1.5.11,12 This treatment modality known as “bridge therapy” is also accepted in surgery clinics. However, neither the effects of such protocol on hemostasis nor all the variables of the hemostatic system have been sufficiently studied in large, controlled trials. Further, unlike other reports, our recently published study confirmed markedly more frequent postoperative bleeding (25%) than expected in patients who underwent LC with bridge anticoagulation therapy. 13
The aim of the present study was to assess hemostatic alterations before, during, and after LC in patients undergoing long-term oral anticoagulant treatment to determine whether these changes have an influence on postoperative bleeding. Therefore, a prospective, nonrandomized, controlled study was designed to compare the characteristics, alterations in the hemostatic system, and postoperative complications of patients maintained on long-term anticoagulation with those who did not receive such therapy.
Patients and Methods
A prospective cohort design was selected and the study was approved by the local institutional review board and ethics committee. Written informed consent was obtained from all patients. In the period from January 2009 to December 2009, a total of 31 patients who underwent elective LC for symptomatic cholelithiasis were enrolled in the study. Sixteen of these patients were on chronic anticoagulation with warfarin (OAC group). The other 15 patients did not receive anticoagulant or antiaggregant drugs and constituted the comparison group (control group). Age, gender, body mass index, preoperative liver function tests, presence of comorbid conditions, American Society of Anesthesiologists (ASA) score, operation time (minutes), hospitalization period (days) of the patients, reasons for anticoagulation, and the duration of such drug use were recorded in a prospective manner. Upon admission, each patient's INR was measured and patients with INR <1.5 were regarded as candidates for surgery. LC was performed with the standard four-port technique. Pneumoperitoneum was maintained at 10–12 mmHg. Intraoperatively, the gallbladder's anatomy and adhesions were noted. The gallbladder was defined according to whether its anatomical appearance was normal, hydropic, scleroatrophic, thick walled, or buried. Our laparoscopic surgery group developed an adhesion scoring over the course of time, based on the degree of inflammatory changes of the gallbladder as a guide for predicting the course of the operation. After the laparoscope was placed, the extent and thickness of the adhesions in the gallbladder region were graded by the surgeon as follows: Grade I, no adhesions; Grade II, flimsy adhesions that permit easy dissection; Grade III, chronic pericholecystitis and pericholecystic fibrosis that makes dissection difficult, but permits visualization of the anatomy; and Grade IV, thickened gallbladder wall and anatomical distortion due to dense adhesions around the gallbladder, which do not permit safe dissection. A hydropic gallbladder was defined as a tensely distended gallbladder. A scleroatrophic gallbladder was defined as a gallbladder profoundly altered by long-standing chronic cholecystitis as indicated by a scarred and contracted appearance, with scarring in the porta hepatis. A thick-walled gallbladder was defined as a gallbladder that is difficult to grasp for retraction. A buried gallbladder was defined as a gallbladder that is more than half encircled by the liver from the posterior side, which makes dissection planes difficult and is more prone to bleeding. 14
As soon as the gallbladder was removed, the liver bed and areas of bleeding were carefully cauterized with electrocautery. The three operative port sites on the peritoneal surface were carefully inspected with the laparoscopic camera after removing the ports while maintaining the pneumoperitoneum. After the pneumoperitoneum was reversed, cutaneous sites of all entry incisions were carefully inspected and closed with meticulous attention to homeostasis. An external drain was placed through the right lateral port incision in all patients of the OAC group, who had a high risk of postoperative bleeding according to our experience from previous operations. 13 In the control group, drains were placed only in selected patients who were regarded to be at high risk of bleeding.
Preparation of the patients receiving chronic anticoagulant therapy for surgery
For LC, antiaggregant drugs were discontinued at 7 days before the planned day of surgery, whereas oral anticoagulant drugs were stopped at 5 days before. The patients were admitted to the hospital at 3 days before. When the patient's INR values were below the therapeutic range (<2.5–3.5), enoxiparin, an LMWH, was started subcutaneously at a dosage of 60 mg twice daily. After the INR decreased to subtherapeutic levels, if the INR further decreased within 3 days to <1.5, the patient underwent LC. If the INR was greater after 3 days, a 2–10 mg dose of vitamin K was given. The final preoperative dose of LMWH was injected at 12–24 hours before surgery. For the patients with a prosthetic cardiac valve, antibiotic prophylaxis was provided with a single dose of sulbactam+ampicillin (1 g) and gentamycin sulfate (120 mg) at the induction of anesthesia.
In the patients on long-term anticoagulation with warfarin, when no bleeding complications were observed postoperatively, a liquid diet was started, and their normal OAC dose (5 mg) was resumed on the first postoperative day. A loading dose was not utilized. On the evening of the day of surgery, the first postoperative dose of LMWH was injected (60 mg). The next day, LMWH was continued at the full dosage (60 mg twice daily). During this time, INR and fibrinogen were measured each day. When patient's INR values reached to their preoperative therapeutic level, LMWH treatment was stopped and OAC treatment was continued. Patients who developed postoperative bleeding were taken under close observation, and in these patients, postoperative LMWH and OAC treatment was not started immediately or was omitted until bleeding stopped.
For the purposes of the study, postoperative bleeding was defined as a hemorrhage that requires blood transfusion and/or reoperation. An intra-abdominal bleeding was defined as bleeding from the drains accompanied by a decline in hemoglobin levels. A port-site bleeding was defined as a hematoma that requires drainage and/or blood transfusion. In patients without drains, postoperative bleeding was defined as a decline in hemoglobin levels accompanied by worsening of vital signs (tachycardia and hypotension) and presence of radiological (ultrasonography [USG] and computed tomography [CT]) findings such as intra-abdominal hemorrhage or hematoma.
Tests applied to patients and timing of the tests
The tests applied to patients are listed in Table 1. Blood samples for the tests were taken immediately before surgery, at 30 minutes after the start of the operation, and at 24 hours after the operation.
 , performed;
, performed;  , not performed; CADP, collagen/ADP; CEPI, collagen/epinephrine; INR, international normalized ratio; PAI-1, plasminogen activator inhibitor type-1; tPA, tissue plasminogen activator; Hb, hemoglobin; PLT, platelets; brb, bilirubin; ALT, serum alanine aminotransferase; AST, serum aspartate aminotransferase; GGT, gamma glutamil transferase; LDH, serum lactate dehydrogenase.
, not performed; CADP, collagen/ADP; CEPI, collagen/epinephrine; INR, international normalized ratio; PAI-1, plasminogen activator inhibitor type-1; tPA, tissue plasminogen activator; Hb, hemoglobin; PLT, platelets; brb, bilirubin; ALT, serum alanine aminotransferase; AST, serum aspartate aminotransferase; GGT, gamma glutamil transferase; LDH, serum lactate dehydrogenase.
Methods of hematological and biochemical analyses and measurement of coagulation parameters
Blood samples were collected into vacutainers containing 0.105 M trisodium citrate (9:1 by volume) (4.5 mL; Glass Citrate Tube; BD Vacutainer) and were centrifuged at room temperature at 3000 rpm for 15 minutes. Plasma and serum were separated and stored in sterile plastic tubes at −25°C until use. All these procedures were carried out according to the Clinical Laboratory Standards Institute guide (CLSI guide H21-A4, 2003).
Measurement of hematological parameters was performed using the Advia 2120 hematology analyzer (Siemens). All biochemical tests were measured using the auto analyzer Modular P800 (Roche Diagnostics). Platelet function was measured on a platelet function analyzer (PFA-100®) using both collagen/epinephrine (CEPI) and collagen/ADP (CADP) cartridges. The normal ranges were considered as 82–150 seconds for CEPI and 62–100 seconds for CADP. Plasma INRs were determined by the standard Quick clotting assay and fibrinogen levels by Clauss thrombin clotting rate assay. Clotting factor levels (factors II, V, VII, IX, X, and XII) were determined using the one-stage clotting method and levels >70% were considered as normal activation. Factor XIII activity was measured by photometric assay.
Statistical analyses
Statistical analysis was performed using an SPSS software version 11.5. If the variables conform to normal distribution, the variance analysis of repetitive measurements was used and Bonferroni's correction was applied for binary comparisons. If the variables did not conform to normal distribution, the Friedman test was performed to detect differences. When a significant difference was found, a multiple comparison test was used to determine which means differed. Student's t-test was used to compare the means of the groups. The Mann–Whitney U test was applied in every case where the requirements of the t-test were not met. For nominal data, comparison of the groups was performed using the chi-square (χ2) test. P values lower than .05 were considered significant.
Results
Heart valve replacement (13 patients, 81.3%) was the most common reason for oral anticoagulant treatment (Table 2). The mean duration on anticoagulation was 64.1±54.9 months.
AVR, aortic valve replacement; MVR, mitral valve replacement.
In the OAC group, beyond their existing conditions, 7 patients had hypertension, 2 patients had diabetes mellitus, and 1 patient had chronic obstructive pulmonary disease as comorbid condition, whereas in the control group, 6 patients had hypertension and 2 patients had diabetes mellitus. There was no statistically significant difference with regard to age, gender, body mass index, and preoperative liver function tests between the groups (P>.05). However, ASA score was higher and hospitalization period was longer in the OAC group than in the control group (P<.05) (Table 3).
ASA, American Society of Anesthesiologists.
All patients complained of symptomatic cholelithiasis. There was no statistical difference between the groups according to the adhesions around the gallbladder (P>.05). None of the patients had Grade IV adhesion. The adhesion scores of the OAC group were Grade I in 9 (56.3%), Grade II in 5 (31.3%), and Grade III in 2 (12.5%) patients. The adhesion scores of the control group were Grade I in 7 (46.7%), Grade II in 7 (46.7%), and Grade III in 1 (6.7%) patient. According to the anatomical appearance, 15 patients (93.8%) of the OAC group had normal gallbladder anatomy, whereas the gallbladder was thick walled in 1 patient. In the control group, 10 patients (66.7%) had a normal gallbladder anatomy, 3 patients (20%) had a thick-walled gallbladder, and 2 patients (13.3%) had a scleroatrophic gallbladder. An external drain was used in all patients of the OAC group. Bleeding from the liver bed during cholecystectomy occurred in 6 patients (40%) of the control group, and hemostasis was achieved by cauterization. These patients were thought to be carrying a risk of rebleeding and so a drain was placed. However, no postoperative bleeding occurred in the control group. The mean drainage was 134.29 mL in the OAC group versus 21.67 mL in the control group. Although higher in the OAC group, the difference was not statistically significant (P>.05).
All patients of the control group had normal vital signs in the postoperative period. Neither decline in hemoglobin levels nor bleeding was observed through drains in this group.
Despite INR values <1.5, postoperative bleeding occurred in 5 patients (31.5%) of the OAC group. The enoxiparine dose was omitted until bleeding stopped or was kept under control. Warfarin therapy was also delayed in these patients. None of the 5 patients with postoperative bleeding required postoperative abdominal exploration. Two patients had continuous hemorrhagic drainage through the drains (400 and 800 mL), and as marked hematomas in the gallbladder fossa were detected by abdominal USG, it was defined as bleeding from the liver bed. In addition, the video record of the 2 patients with intra-abdominal bleeding was carefully reviewed and no other origin for bleeding was found outside the liver bed. In these patients, anticoagulation was stopped, close monitoring was started, and fresh-frozen plasma with vitamin K was given. Bleeding ceased in 2 days under conservative follow-up. The other 3 patients had umbilical port-site bleeding. Ultrasonographic examination revealed a subcutaneous hematoma localized in the umbilical region without intra-abdominal bleeding. Of these patients with umbilical port-site bleeding, 1 required 2 units of erythrocyte suspension replacement because of a fall in hemoglobin concentration from 11 to 7.6 g/dL. The other 2 patients underwent evacuation of the hematoma under local anesthesia.
The preoperative and postoperative hemoglobin levels, platelet counts, and markers of platelet function (CADP and CEPI) were compared. Significant reductions in postoperative hemoglobin levels were observed in the OAC group compared with the control group (12.5%±9% versus 3.4%±4.4%; P<.05) (Fig. 1). Platelet counts, CADP, and CEPI levels in both groups did not differ according to time periods. INR levels in the postoperative period were significantly higher than that in the preoperative period among all patients in the two groups. The mean values of INR in both the preoperative and postoperative periods were significantly higher in the OAC group than in the control group during the corresponding time periods (P<.05) (Table 4 and Fig. 2). However, increase in INR levels was significantly higher in the control group when compared with the increase in the OAC group.
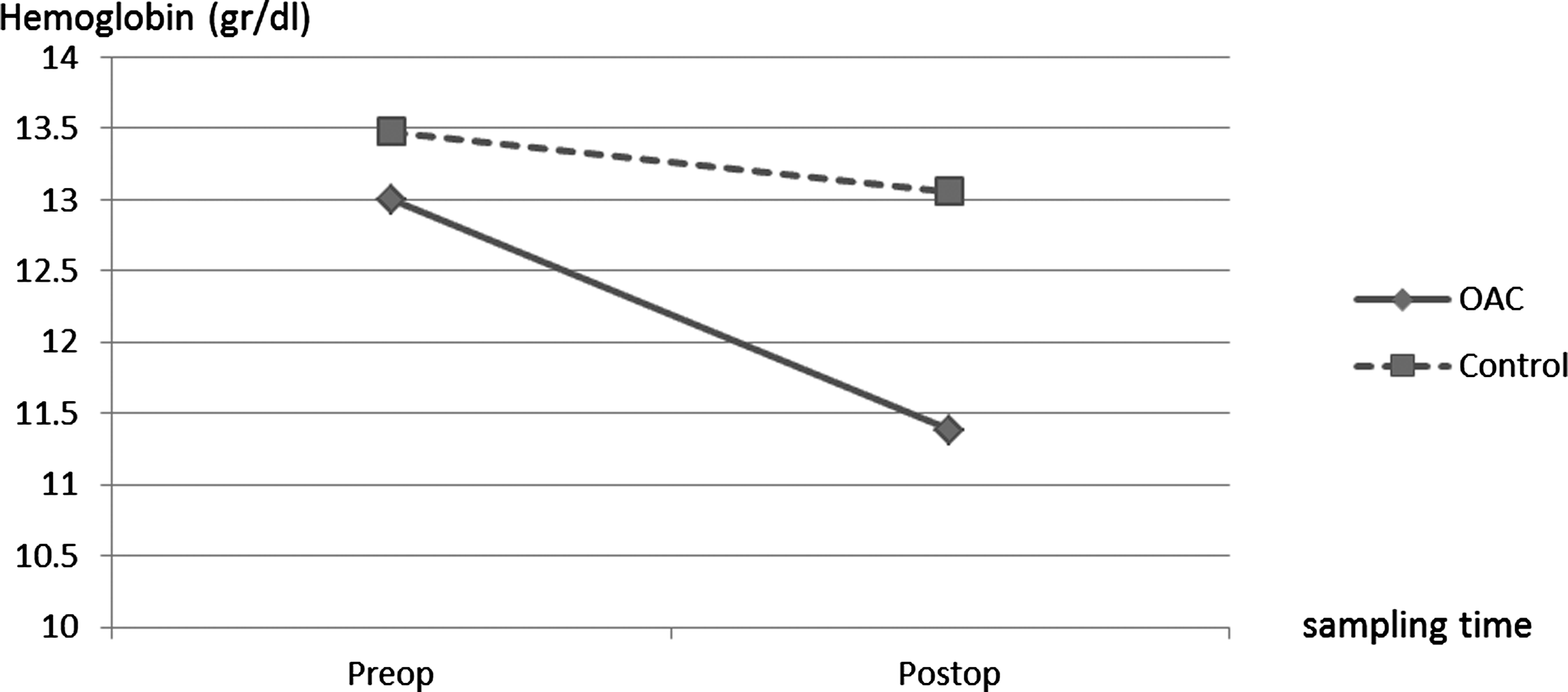
Change in hemoglobin levels. Postoperative mean hemoglobin levels were significantly reduced in the OAC group when compared with the control group (P<.05).
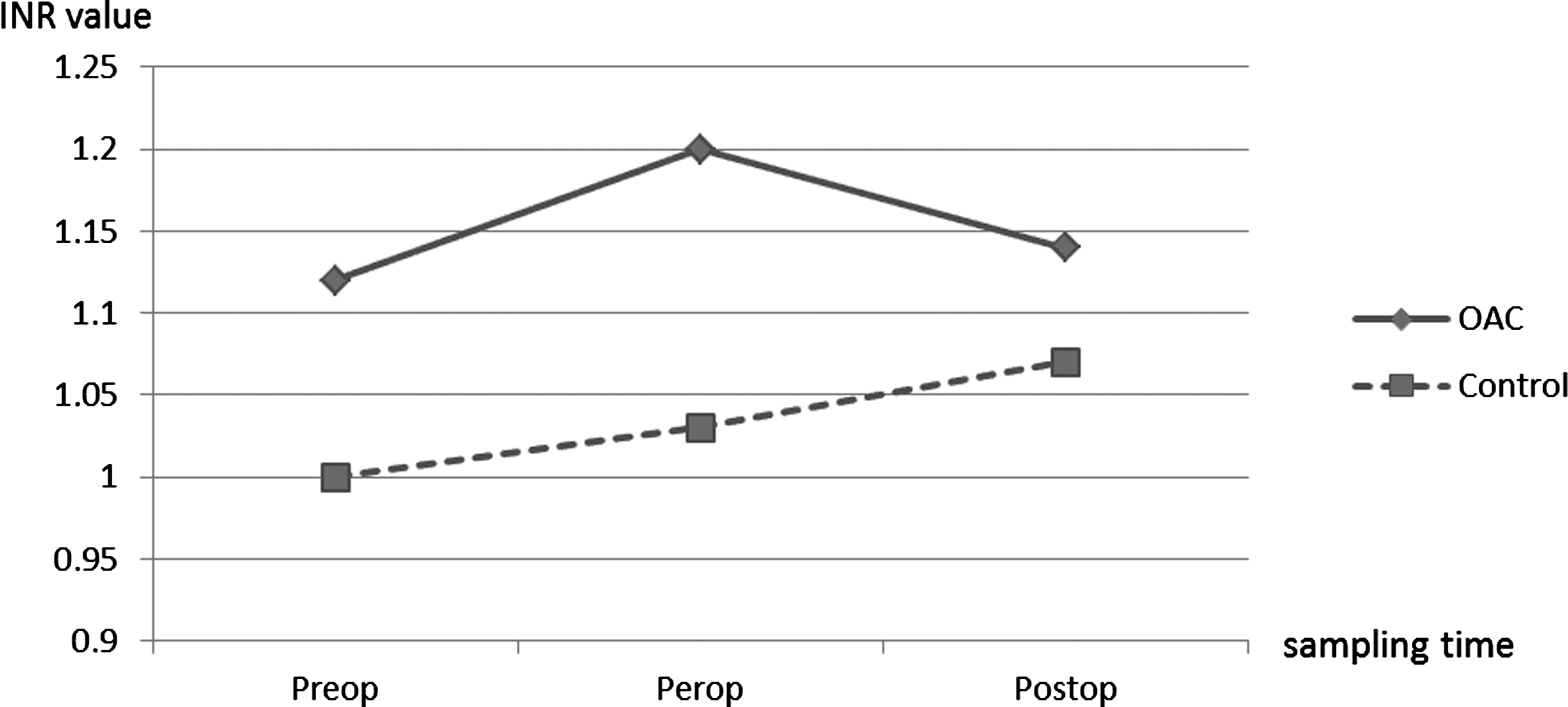
International normalized ratio (INR) values in preoperative, peroperative, and postoperative periods. INR values were within normal ranges but significantly higher in the OAC group when compared with the control group (P<.05).
P values that indicate difference between time periods.
P values that indicate difference between groups.
SD, standard deviation.
Factor X levels of the OAC group were below normal values (<70%) in the preoperative and peroperative time periods. The mean values of other clotting factors and their distribution according to the time periods were within normal ranges in both the OAC and control groups (Table 5). Factor II, VII, IX, and X levels were significantly lower in all time periods of the OAC group when compared with the control group (P<.05).
Levels >70% were considered as normal activation.
P values that indicate difference between the groups.
Indicators of the fibrinolytic system were within normal ranges in both groups (Table 6). PAI-1, fibrinogen, and

Tissue plasminogen activator (tPA) activities of the groups. Although being in normal ranges, tPA activity was significantly higher in the OAC group when compared with the control group (P<.05).
P values that indicate difference between the groups.
In the OAC group, parameters of the patients with (n=5) and without (n=11) postoperative bleeding were assessed, although statistical analyses could not be performed because of small number of patients with bleeding (Table 7). Remarkably, factor X levels were less than normal for all time periods in all patients with postoperative bleeding. The INR levels were similar in both the bleeding and nonbleeding patients. The tPA activity was similar in the preoperative period but decreased in the nonbleeding patients in the postoperative period; however, a slight increase was observed in the patients with postoperative bleeding.
Statistical analyses could not be performed because of small number of patients with bleeding.
Discussion
The major risk encountered during laparoscopic procedures performed on patients undergoing anticoagulant therapy is the possibility of hemorrhage. It has been suggested that the minimally invasive nature of LC, as well as the magnified operative field, facilitates the perioperative management of gallbladder disease in patients on anticoagulant therapy. Two early retrospective case series reported that no bleeding occurred in patients on long-term anticoagulation therapy who underwent LC.2,4 However, in our previous study, a bleeding rate of 25% was reported in patients on long-term OAC therapy and the bleeding rate was only 1.5% in the comparison group. 13 Similarly, a high postoperative bleeding rate of 31.5% is reported in the present study. Our hospital is a high-volume tertiary referral center for cardiovascular surgery and the general surgical patient population is frequently comprised of persons who are on long-term OAC with additional medical comorbidities. In the period from January 2002 to December 2007, a total of 2963 patients underwent LC in our clinic and the documented postoperative bleeding rate was approximately 1.5%, which was comparable to 0.69% of postoperative bleeding in a series of 10,174 LCs reported by Z'graggen et al. 15 Further, our two series determined that patients on long-term OAC did not differ from those who did not receive OAC in terms of INR values, operative time, or intraoperative blood loss. However, postoperative bleeding occurred in a significantly higher proportion of patients on long-term OAC. Similar high postoperative bleeding rates were also found in patients on long-term OAC by Varkarakis et al. 16 and Mourelo et al. 17 after laparoscopic renal/adrenal surgery and laparoscopic bariatric surgery (8% and 14%, respectively). None of the patients in the control group experienced postoperative bleeding in this study. In addition, as stated earlier, our bleeding rate in patients who did not receive OAC was found to be extremely low when compared with that in patients on long-term OAC. Surgical techniques and inspection of the liver bed and peritoneal and cutaneous surfaces of the port sites were performed in the same manner in all patients. Moreover, nearly all patients in the OAC group had normal gallbladder anatomy (except 1, who had a thick-walled gallbladder). Although 33.3% of the patients in the control group had scleroatrophic or thick-walled gallbladder, which made cholecystectomy technically more difficult and prone to bleeding, no bleeding occurred in the control group even in patients with drain placement for suspected bleeding. Therefore, we suggest that the reason for high postoperative bleeding in patients on OAC cannot be related to our surgical inexperience or technical insufficiency.
How does laparoscopy act on hemostasis in patients receiving OAC? Could it be a part of the mechanism causing postoperative bleeding? Various studies have shown that reverse Trendelemburg position and pneumoperitoneum created during the procedure leads to splanchnic vasoconstriction, which decreases venous return and increases the risk of venous thromboembolism. Pneumoperitoneum additionally damages the vessel wall, leading to activation of coagulation with enhanced global fibrinolytic activity.18,19 However, these transient changes were found to be mild and not significant.20–26 It is conceivable that these effects might be more pronounced in patients who are already on long-term OAC. Moreover, the effects of LC on the hemostatic system have not been sufficiently detailed for patients on long-term OAC, and the series published so far consists of small groups.1–3 For these reasons, the present study has been planned in a much more comprehensive way to investigate the homeostatic changes before, during, and after the LC for patients who were under long-term oral anticoagulant treatment.
Specific hemostatic laboratory tests have been chosen to reflect the well-known biology of hemostasis. The hemostatic process can be evaluated within the concept of primary and secondary hemostases. Primary hemostasis comprises blood vessel contraction just after vessel injury, followed by the adhesion and activation of platelets. The secondary hemostatic process involves the activation of the coagulation system, causing generation of thrombin and ultimately leading to the formation of a fibrin matrix stabilizing the platelet plug. The fibrinolytic system is necessary to avoid inappropriate fibrin accumulation, which could lead to thrombosis. To evaluate the primary hemostasis, platelet counts and the PFA-100 were used. In addition to INR, activation levels of the coagulation factors were used to evaluate the secondary hemostatic process, and tPA and PAI-1 levels were examined to evaluate the fibrinolytic activity. The sampling intervals to test those representative hemostatic elements have been chosen to reflect preoperative, peroperative, and postoperative interventional alterations of the primary and secondary hemostases.
In the present study, all hemostatic parameters were within normal ranges in both groups. The usual parameters of coagulation appear unable to predict which patients on anticoagulant therapy will bleed after surgery. However, significant reductions in hemoglobin levels were observed in the OAC group postoperatively. Although being within normal ranges, INR values and the tPA activity were significantly higher, whereas factor II, VII, IX, and X levels were significantly lower in the OAC group when compared with the control group. These significant differences between the two groups may partly contribute to postoperative bleeding.
The low levels of vitamin K–related clotting factors (factors II, VII, IX, and X) and the increase in INR values are expected to be natural results due to anticoagulant treatment. Coumadin derivatives interfere with the carboxylation of the clotting factors II, VII, IX, and X as well as proteins C and S. By inhibiting the synthesis of these proteins, they shift the hemostatic balance to a lower level.
It is not clear whether the relative increase in tPA concentrations of the patients in the OAC group is related to chronic anticoagulation or bridge therapy. If we initially questioned the impact of laparoscopy on the fibrinolytic system, most of the publications indicated that LC does not increase the activity of tPA.23,26–28 On the other hand, contradictory results were reported in a few studies that examined the effects of OAC therapy on tPA activity. One of these studies reported that tPA levels decreased under OAC treatment, 29 whereas another study showed the opposite. 30 Further, the effect of bridge therapy on tPA activation has not yet been handled in detail. Thus, there are no available data to define a close relationship between bridge therapy and tPA activation. One of the limitations of the present study is that protein C and S levels have not been studied, which could be useful to solve these ambiguities or may elucidate the cause of bleeding.
Patients on long-term OAC might be considered at risk of postoperative bleeding even when preoperative INR values are within normal ranges. It should not be forgotten that these patients frequently have extra comorbidities, and therefore, preoperative assessment should be carefully and meticulously planned. Otherwise, postoperative bleeding may lead to hazardous results and may be fatal. For these reasons, patients receiving anticoagulant treatment should be operated in tertiary centers and we recommend patient's admission at 3–5 days before surgery. Because of the thromboembolic risks due to OAC withdrawal, the commencement of UHF or subcutaneous LMWH in a twice-daily dosing scheme known as bridge therapy seems to be practical. Our clinic prefers LMWH because of the advantages of subcutaneous dosing, a predictable anticoagulant response, and less heparin-induced thrombocytopenia compared with UHF. However, in both of our studies, we observed an unexpected high postoperative bleeding rate in patients receiving OAC treatment. Bridge anticoagulation decreases the amount of time patients are not anticoagulated but may increase the risk of postoperative bleeding. Although postoperative bleeding rates are low in the mixed series of patients who underwent various types of surgery with bridge anticoagulation,11,12,31 the available literature does not provide sufficient information to allow clinicians to choose an optimal perioperative strategy.
In conclusion, this prospective, nonrandomized, controlled study has determined that patients receiving OAC are at risk of postoperative bleeding even if their INR values are within normal ranges. The patients receiving OAC therapy had significantly lower factor II, VII, IX, and X levels and increased tPA activities when compared with normal subjects. The main mechanisms that can cause bleeding remain unclear and more sensitive methods should be developed to measure the degree of risk of bleeding. Further, the efficacy of the bridge anticoagulation therapy should be reviewed and further studies are needed to optimize the bridging strategy.
Footnotes
Disclosure Statement
No competing financial interests exist.