
Abstract
Abstract
Background:
Single-port laparoscopic-assisted vaginal hysterectomy (S-LAVH) uses only one transumbilical incision site and has better cosmetic result than conventional multiport LAVH. This study aimed to evaluate our initial experience with S-LAVH compared with the more conventional three-port LAVH in women with benign uterine diseases.
Methods:
Between April 2009 and April 2010, S-LAVH was attempted on 183 patients with benign uterine diseases through a transumbilical incision for a 12-mm trocar, and conventional LAVH was performed on 275 patients by the same surgeon. The medical records of patients were reviewed. The age, body mass index, operative time, blood loss, and uterine weight on pathologic report were compared.
Results:
Two of 183 patients in the S-LAVH group were converted to two- or three-port surgery, compared with none in the conventional group. Data analysis was done for 181 patients in the S-LAVH group and 275 patients in the conventional LAVH group. No major complications, including ureteral or bladder injuries, occurred in any of the patients. No statistically significant differences were found in mean age, mean body mass index, mean operative time, mean anesthesia time, mean estimated blood loss, or mean postoperative days to passage of flatus, but the mean uterine weights on the pathologic reports were significantly reduced in the S-LAVH group.
Conclusion:
S-LAVH could be a feasible alternative method for removal of the uterus with a better cosmetic outcome resulting from single wound in selected patients. For patients with large-sized uterus, more surgical experience and improvement in instruments suitable for S-LAVH are needed.
Introduction
After the first report of a single-port laparoscopic hysterectomy,3,4 many attempts have been made in various laparoscopic procedures (gastroenterology, gynecology, and urology).5–9 These procedures have used Uni-X Single Port Access (Pnavel Systems), TriPort (Advanced Surgical Concepts), AirSeal (SurgiQuest), and SILS ports (Covidien) as multichannel working ports, critical tools for single-port surgery. No commercial multichannel port system was available in Korea till the end of this study. Therefore, we had used a multiple working channel port with the use of a surgical glove and a wound retractor (Alexis; Applied Medical, Rancho Santa Margarita, CA) and performed LAVH via a single port.
Herein, we report on our preliminary surgical outcomes of 181 patients who underwent transumbilical single-port access laparoscopic-assisted vaginal hysterectomy (S-LAVH) by a single surgeon.
Materials and Methods
Retrospective data were reviewed after the institutional review board approved of this study between April 2009 and April 2010. S-LAVH was attempted in 183 patients and successfully completed in 181 patients. Conventional LAVH, which uses three ports, was attempted and successfully completed in 275 patients. All S-LAVH and conventional LAVH were performed by a single surgeon (M.H.J.) for patients with benign uterine diseases.
The patient was placed in the dorsal lithotomy position. A vertical incision was made within the umbilicus for a 12-mm trocar insertion. The 12-mm trocar was inserted directly using a closed technique, instead of using a Veress needle for creating a pneumoperitoneum. After checking the intra-abdominal status via the first transumbilical trocar, a 3-cm wound retractor (Alexis) was transumbilically inserted into the wound opening. After making a multiple working channel port with the use of a surgical glove and three conventional trocars (Applied Medical), it was connected with Alexis. This is a similar method to that described by Lee et al. 10
A surgical glove with cut ends of the distal finger tips and tied with an elastic bandage to prevent leakage of carbon dioxide was draped around the rim of the wound retractor. The elastic nature of the glove enabled it to obtain a good purchase on the ring and achieve an airtight seal, which maintained the pneumoperitoneum. The multiple fingers of the glove functioned as a multiport for laparoscopic instruments and a camera (Fig. 1). A uterine manipulator was inserted to effectively make a surgical field.
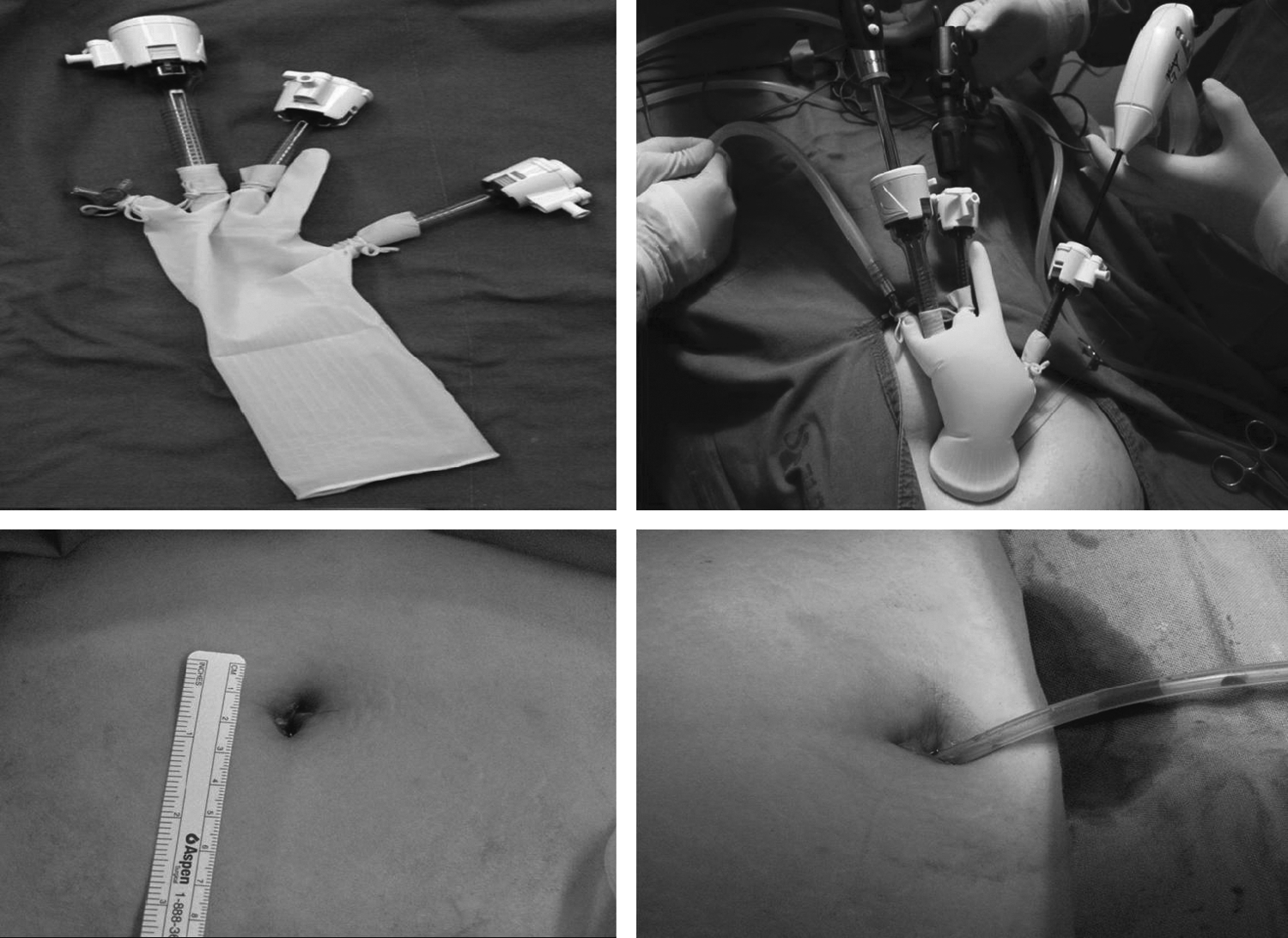
Single-port surgical system: 12-mm laparoscope, 5-mm ligasure, 3-cm wound retractor, articulating flexible surgical instrument, one 12-mm trocar, and two 5-mm trocars. The postoperative transumbilical wound dose not extended over the umbilical margin. The drain, if necessary, is inserted transumbilically.
We used a 12-mm laparoscope and an articulating flexible RealHand surgical instrument (Novare) to avoid clashing of the instruments and to optimize the range of motion as the trocars move within the glove channel. The round and broad ligaments were dissected with monopolar cautery and the ovarian or infundibulopelvic ligament was dissected with a 5-mm ligasure (Valleylab).
After separating the anterior and posterior leaves of the broad ligament, we identified the vesicouterine peritoneal fold and continued the dissection anteriorly, thereby mobilizing the bladder off the lower uterine segment laparoscopically. We then began the vaginal approach. The procedure for three-port LAVH was the same as S-LAVH, with the exception of the number of ports.
The primary study outcomes were different in the following main operative data: operating time (calculated from skin incision to closure), anesthesia time (calculated from induction to awakening), blood loss (estimated by calculating the blood volume of the suction machine during surgery, excluding liquid utilized for intraperitoneal washing, and by weighing swabs), postoperative bowel gas passage time (calculated in days from the end of the procedure to gas passage), and postoperative complications (any unfavorable episode occurring within 30 days after surgery, requiring readmission, blood transfusion, or repeat surgery). Intraoperative complications included damages to the bowels, urinary system, or vasculature.
Student's t-test and chi-square test were used for statistical analysis. A value of P<.05 was considered statistically significant.
Results
The pathologic reports of all patients who underwent laparoscopic hysterectomy showed uterine myomas and/or adenomyosis.
There was no difference in demographic and perioperative data between the two groups except the mean uterine weights. It was significantly lower in the S-LAVH group (Table 1).
Data are mean±standard deviation.
LAVH, laparoscopic-assisted vaginal hysterectomy.
Two patients who underwent the S-LAVH procedure were converted to two- or three-port LAVH. One patient was converted to three-port LAVH for bleeding control of the right uterine vein. The other patient was converted to two-port LAVH because of an incidental finding of an appendiceal mucinous adenoma. The cecal resection was performed with two ports.
There were no cases of operative conversion in patients undergoing conventional three-port LAVH.
We encountered no postoperative complications, including reoperations, adjacent organ damage, and postoperative morbidity.
Discussion
Hysterectomy is the second most common surgical procedure performed worldwide. 11 Traditionally, hysterectomies have been performed via the abdominal or vaginal routes. By necessity, all surgical interventions involve the process of traumatizing normal tissues in order to remove, repair, or examine abnormal tissues, and the focus of minimally invasive surgery is to accomplish a procedure with the least disruption of normal tissues.
Laparoscopic hysterectomy was first reported in 1989, and since then a number of refinements have been described, depending on the extent of surgery carried out via the laparoscope.1,2,12,13
Laparoscopic hysterectomy is currently the very preferred care for uterine removal in Korea, with the open technique being largely reserved for failure of laparoscopic resection.
LAVH is a safe, established procedure for uterine disease, usually performed through three small incisions. Although postoperative pain is minimal, there exists some discomfort from multiple incisions. In theory, surgery with fewer incisions or without incisions may decrease postoperative morbidity more than that which currently exists. Today, we stand on the brink of a technological explosion that may drive surgery from requiring small incisions to none at all.
Reports of microport instrumentation as well as normal orifice transluminal endosurgery cholecystectomies transvaginally, transcolonically, or transgastrically have been recently reported. However, these surgical procedures require a different set of skills and new technology, which is in its developmental infancy.2,14–18
Single-incision surgery has recently entered the minimally invasive arena. The results of this study showed that the S-LAVH is safe, feasible, and reasonably time-efficient, even with our initial experience with this new technique.
In selection of the patients enrolled in this study, we did not exclude any patient who was expected to have severe pelvic adhesions on the basis of previous surgical or medical history.
The benefits of S-LAVH with surgical glove and wound retractor are listed as follows: first, a better cosmetic outcome was possible by limiting the number of port incisions to only one site and concealing the scar within the umbilicus without any wound complication; second, use of a surgical glove and a wound retractor for the single-port system was practical, because we could perform all procedures with only minimal modification of the conventional surgical techniques; and finally, if needed, we could easily convert to a conventional LAVH, and in that situation, cost is saved, because the trocars could be reused.
Prior studies have shown that one of the technical limitations of the commercial multichannel working port was the clashing of instruments.5,6,9 This was also observed in our study. In addition, a limitation in the range of motion of the scope through the single-port access was another disadvantage. However, all of the current problems are likely to be resolved by more advancement in the equipments available with articulating instruments and scopes with flexible tips.
For experienced gynecologic laparoscopists, S-LAVH is safe and feasible although technically more difficult and could be an alternative method for very well-selected patients, with cosmetic advantages in comparison to the conventional method. But larger, prospective, comparative studies on conventional multiport LAVH with cost analysis, surgical outcome analysis, and long-term follow-up will be necessary.
Footnotes
Disclosure Statement
M.H. Jung has received Kyung Hee University Research Fund in 2007 (KHU-20070717).