
Abstract
Abstract
Background:
Sleeve gastrectomy represents a valid option for morbidly obese patients, either as a primary or as a staged bariatric procedure. Several variations of the technique have been reported. Herein, we report our initial experience with robot-assisted sleeve gastrectomy (RASG).
Materials and Methods:
A prospectively held database for patients who underwent RASG was reviewed. Data included patient demographics, operative parameters, morbidity, and follow-up outcomes. The outcomes after RASG were compared to the laparoscopic approach.
Results:
From September 2007 to February 2010, 69 morbidly obese patients underwent sleeve gastrectomy. Of these, 30 (43.5%) were robot-assisted and 39 (56.5%) were laparoscopic. There was no statistically significant difference in demographics between the two groups. The RASG group underwent an oversewing of the staple line, and mean operative time was 135 minutes. In the laparoscopic group, where the staple line was not oversewn, mean operative time was 114 minutes (P = .003). Morbidity after RASG was 3.3%, and there were no gastrointestinal leaks or staple line bleeding. Mean postoperative hospital stay after RASG was 2.6 days (range: 1.6–8.3 days). Mean body mass index decrease at 1 year was 16 kg/m2. There were no differences between the two groups in terms of morbidity, mortality, length of stay, and weight loss.
Conclusions:
RASG can be performed safely, with good outcomes. However, the exact role and the advantages of RASG require further study in larger series.
Introduction
Still, there are relatively few series that have reported middle and long-term follow-up for SG as a single-stage procedure.12,13 Likewise, although the da Vinci robotic system (Intuitive, Sunnyvale, CA) has been used successfully since the early 2000s in the bariatric population, essentially for LRYGB,14–16 its role in performing SG is still unclear and the literature remains scarce.17,18
The aim of this small series was to evaluate the outcomes of robot-assisted SG (RASG), all performed at a single institution by a single surgeon.
Materials and Methods
From September 2007 to February 2010, all patients undergoing an SG were prospectively followed up at a single institution. Patients met the National Institute of Health Consensus Criteria 19 as well as the institutional policies for undergoing a bariatric procedure. An informed consent was obtained from all patients.
A total of 69 patients had an SG performed by a single surgeon during the study period. Group 1 patients underwent a robot-assisted approach and group 2, a laparoscopic approach. The choice of the technique was made by the surgeon.
Data on patient demographics, operative variables, and postoperative complications and outcomes were collected prospectively in a dedicated bariatric database and reviewed retrospectively. The operative time was defined as the time from skin incision to skin closure, including any associated procedures. All patients were followed up at an outpatient clinic.
Surgical technique: laparoscopic SG
The patient was positioned in partial lithotomy position. A Veress needle was inserted through the left upper quadrant to achieve pneumoperitoneum. A 10/12 mm trocar was placed just above the umbilicus under direct observation (optical trocar). Two other 10/12 mm trocars were placed on either side of the camera port. An additional 10/12 mm trocar was then placed in the left upper quadrant, and a 5 mm incision was made to place a Nathanson Liver Retractor (Mediflex®, Islandia, NY) (Fig. 1).
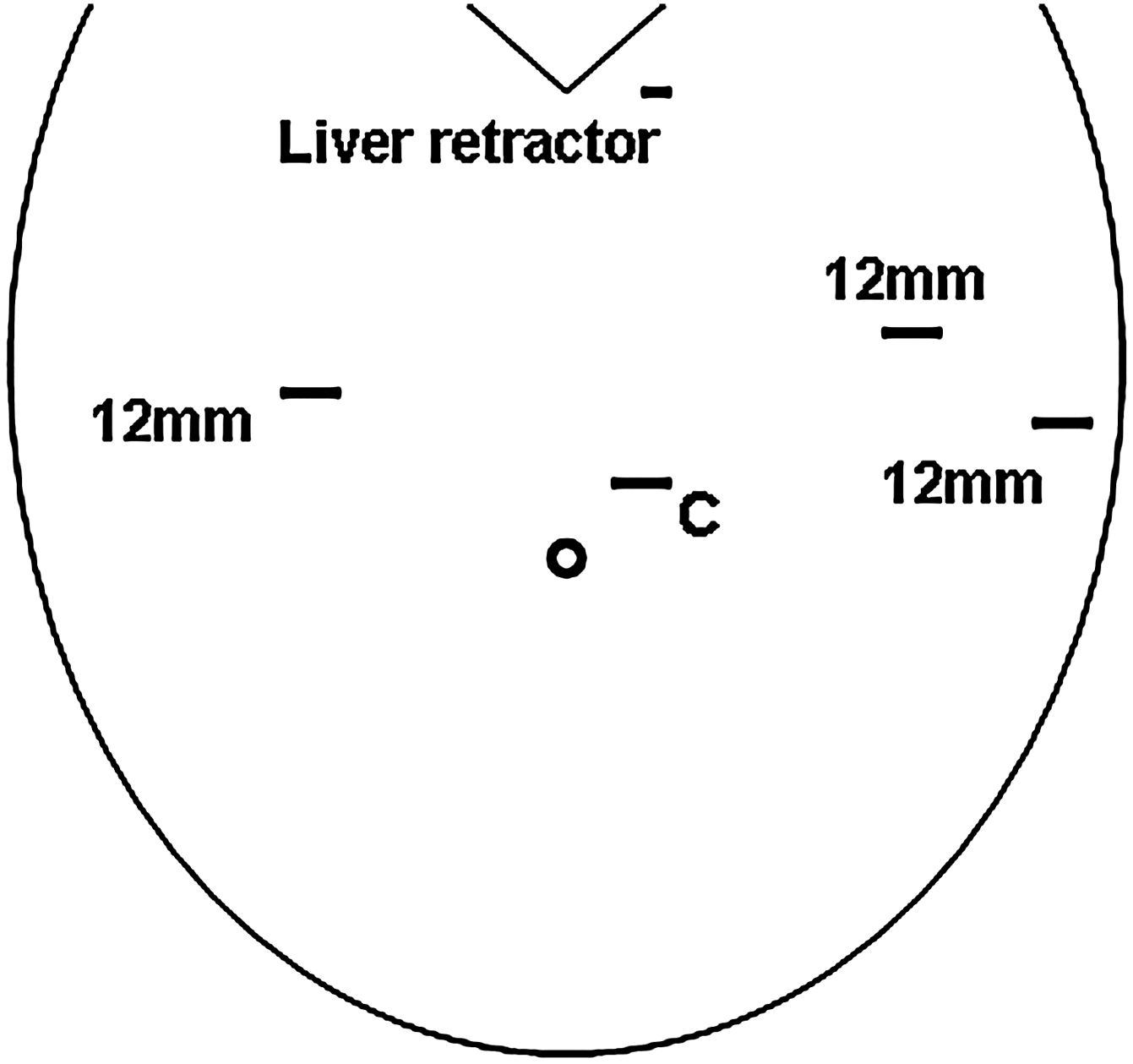
Port placement. C, camera (12 mm).
The vascular supply of the greater curvature of stomach was taken down using a harmonic scalpel starting ∼6–7 cm from the pylorus, all the way to the left crus. The short gastric vessels were taken down from the gastrosplenic ligament. Sequential stapling (green loads; Ethicon, Somerville, NJ) with staple line reinforcers (Gore Seamguard®; WL Gore & Associates, Inc., Flagstaff, AZ) was performed to transect the greater curvature of the stomach, which started ∼7 cm from the pylorus. A 40F Maloney dilator was used as a guide to create the sleeve. Once the greater curvature of the stomach was completely separated, an endoscopic check was performed to control the integrity of the staple line. The specimen was then removed by extending one of the trocar site fascias.
Surgical technique: RASG
The first steps of an RASG are essentially the same as the laparoscopic SG, including the trocar setup. Once this was completed, the vascular supply of the greater curvature of stomach was taken down and the great curvature completely separated. Here again, sequential stapling with staple line reinforcers (Gore Seamguard; WL Gore & Associates, Inc.) was performed to transect the greater curvature of the stomach at ∼7 cm from the pylorus. A 40F Maloney dilator was used as a guide to create the stomach tube from greater curvature to the lesser curvature. Once the greater curvature of the stomach was completely separated, the robot was docked cranially and the arms are attached trocar in trocar double cannulation technique. The entire staple line was inverted by placing sero-serosal sutures of 2-0 PDS (Ethicon) beginning at the angle of His. An esophagogastroduodenoscopy was then performed to exclude any hemorrhage or leak.
Statistical analysis
The results of parametric and nonparametric data were expressed as mean ± standard deviation and median (range), respectively. GraphPad Software (La Jolla, CA) was used for all statistical analyses. Confidence intervals were set at 95%. A two-sided P value of ≤.05 was considered statistically significant. Comparisons between groups 1 and 2 were carried out using Fisher test for discrete variables and Student's t-test for continuous variables.
Results
During the study period, a total of 69 patients had an SG. Of these, 30 were robot-assisted (group 1: 43.5%) and 39 were performed laparoscopically (group 2: 56.5%). There were 64 women (92.8%) and 5 men (7.2%) included in this study. The overall mean age was 38 ± 9.5 years (range: 24–61).
There was no difference between the two groups in terms of demographics (Table 1). The mean number of comorbidities was not statistically significant between the robotic and the laparoscopic approach (2.4 versus 2, respectively; P = .94) and the initial mean BMI was similar in both groups (57 versus 56; P = .72).
SD, standard deviation; BMI, body mass index; GERD, gastro-esophageal reflux disease.
Perioperative results
The mean operative time for RASG was longer than that for the laparoscopic group (135 minutes versus 114 minutes, P = .003) (Table 2). This can be attributed to all cases in group 1 undergoing an inverted oversewing of the staple line, compared to no cases in group 2 (P = .0001). There was no statistically significant difference between the two groups with regard to associated procedures. Seven patients underwent additional procedures (2 in group 1 and 6 in group 2; P = .45) including 4 lysis of adhesions, 2 liver biopsies, 1 cholecystectomy, and 1 removal of band performed during the study.
Including the time for docking the robot and oversewing the staple line.
Bold numbers represent statistical significance (P < 0.05).
OR time, operative time (in minutes).
Finally, in this series, there were no intraoperative complications or deaths. There was also no difference in amount of blood loss between the two groups (21 mL versus 22 mL; P = .84). One patient in the laparoscopic group was converted to an open procedure due to extensive adhesions. No conversions were noted in the robotic group (P = 1).
Postoperative results
There were no postoperative deaths in this series (Table 3). One patient in the robotic group had to undergo reoperation due to nausea and vomiting in the early postoperative course. Following an upper gastrointestinal series, a gastric obstruction was observed. At reoperation, suture removal on the staple line resolved the problem and the rest of the postoperative course was uneventful. There was no statistically significant difference between the two groups with regard to morbidity or length of stay (2.6 days versus 2.4 days; P = .35).
Bold numbers represent statistical significance (P < 0.05).
Finally, no statistical significant difference was noted in terms of weight loss. The mean BMI decrease was similar in both groups at 1 month and 1 year: 7 and 16 kg/m2, respectively, for group 1, and 6 and 15 kg/m2 for group 2 (P = .19 and .63). However, at 6 months, a significant difference was noted in BMI decrease: 15.7 for group 1 and 12 kg/m2 for group 2 (P = .04).
Discussion
To our knowledge, we present one of the first studies evaluating the robot-assisted approach for SG in morbidly obese patients.
Although it has been well demonstrated that SG can be performed safely with good short-term outcomes,8–11 the long-term follow-up of SG as a single-stage procedure remains underreported. Very recently, Bohdjalian et al. 12 have reported long-term ghrelin level after SG. They showed that the ghrelin level seems to remain low even at 5-year follow-up, thus leading to stable weight loss. Still, the evidence remains scarce for long-term outcomes after SG.
Originally, SG was proposed as a bridging procedure for super-morbidly obese patients to improve comorbidities and to achieve weight loss before undergoing a more radical procedure such as biliopancreatic diversion or LRYGB.4–6 Numerous studies, however, have demonstrated the effectiveness of SG as a single-stage procedure.1–3 In fact, weight loss and improvement in comorbidities have been reported as comparable to LRYGB and even better than LAGB.7,8,11
In this study, we found a median BMI decrease of 6, 14, and 15 kg/m2 at 1, 6, and 12 months, respectively, for the entire study population. There were no differences in terms of demographics or comorbidities between the laparoscopic and the robot-assisted groups. At 6 months of follow-up, the robotic group had lost more weight than the laparoscopic group (BMI decrease of 15.7 versus 12 kg/m2 respectively; P = .04). Interestingly, this difference disappeared at 1 year (16 versus 15 kg/m2; P = .63), and we do not think it was related to application of the robot.
Although SG has the advantage of preserving the gastric function without postoperative malabsorption, 20 it also has a long staple line with the potential for hemorrhage and leak at reported rates of 0.4% and 0.8%–1.45%, respectively.21,22 The robot has the advantage of endowristed instruments, which can help oversew the stapled line, theoretically minimizing the risk of hemorrhage or leak by allowing precise placement of suture to oversew the staple line. It is also an interesting training model for fellows and residents to train on the robotic system as it entails sewing in alignment that could be applied to complicated cases (RYGB). This teaching aspect is important and can be developed in academic institutions.
At the end of each procedure, an upper endoscopy was performed to check the integrity of staple line. In our series, we did not notice any gastrointestinal leaks or hemorrhage, even in the laparoscopic group, where no oversewing of the staple line was performed.
Recently, Dapri et al. 23 published a study comparing three methods of gastric closure during SG. They prospectively randomized 75 patients into three groups—group 1: no staple line reinforcement; group 2: buttressing of the staple line with Gore Seamguard®; group 3: staple line suturing. Their study showed that group 2 had less blood loss during stomach sectioning, but there was no difference in the leak rate. Others, 22 however, have reported that routine reinforcement of the staple line after SG is questionable at best because the leak rate is so small. Although a laparoscopic oversewing can be technically challenging, we have shown in the present study no difference between the two groups in terms of leak or bleeding. Of note, the only complication reported in our series was in the robotic group. This was caused by a gastric obstruction caused by a suture narrowing the sleeve at the incisura angularis, which required a reoperation, despite the routine use of upper endoscopy at the end of the procedure. Thus, the real advantage of routine reinforcement of the staple line remains unclear.
Unlike LAGB and LRYGB, SG is irreversible, 24 although it can be converted to biliopancreatic diversion with duodenal switch or to LRYGB.5,6 In fact, some authors have presented their results for robotic duodenal switch as a one-staged procedure.17,18 In these small series, the results are promising and show no mortality and low morbidity (<10%), and no leaks in one series. 17 The robot was reported to add precision when placing sutures for the duodenoileostomy. For LRYGB, different studies have shown a clear advantage of the robotic approach in terms of leak 14 and operative time. 25
So, the exact role of the robot for SG remains poorly defined. For SG, we report one of the first comparative studies of the laparoscopic approach to the robot-assisted approach. Even with a slightly different technique, the complication rates were similar in both groups; in fact, the only parameter that was statistically different was the operative time. This later can be attributed to the suture time and docking time in the robotic group. Moreover, since the introduction of the da Vinci system in the early 2000s, a longer operative time has been reported in the literature and is the result of setup time. 26 A trained team, however, can reduce this time. 27
This study has some limitations that deserve comments. First, this is a relatively small and nonrandomized study. Yet, it is a preliminary series that tried to assess several specific issues like safety and feasibility after RASG. Then, the laparoscopic and robot-assisted approaches differ technically. Indeed, during the first one, the suture line was not oversewn. Although some could argue that it is difficult to compare two different procedures, the main message remains clear. The robot-assisted approach can achieve at least the same results as the laparoscopic approach. The longer operative time in the robotic group can be explained by the difference in the technique (oversewing versus no suture). However, the real benefit of reinforcing the staple line remains hypothetical and further studies are needed to clarify this aspect.
Another issue with the robotic approach is the overall cost. This study does not address cost, but it is well known that the robotic approach is more expensive than the laparoscopic approach, as has been demonstrated for other procedures.28,29 Finally, the decision to use or not the robot for an SG could be based on several factors: the availability of the robot, a concern about the staple line (integrity, bleeding, etc.), the case load of the surgeon for that day, and the type of institution where the robotic procedure is performed (teaching for the fellows and residents). As a result, until a clear benefit can be demonstrated, routine use of the robot for SG may continue to be debated.
Conclusions
Both laparoscopic and RASG can be performed safely with good outcomes. The exact role of RASG should be further defined through larger series. Additionally, long-term follow-up will be required to properly evaluate the sustainability of this procedure as an alternative approach to gastric bypass or duodenal switch.
Footnotes
Acknowledgment
The authors would like to thank Mirza Baig for the maintenance of the database.
Disclosure Statement
No competing financial interests exist.