
Abstract
Abstract
Background:
Conventional open surgery for infected pancreatic necrosis is associated with significant surgical morbidity, that is, wound complications, facial dehiscence, and intestinal fistulae. In recent years, there has been interest in attempting to reduce this surgical morbidity by adopting a number of minimally invasive approaches. 1
Methods:
Fifteen patients with pancreatic necrosis underwent pancreatic necrosectomy by minimally invasive surgery (11 men, 4 women; age group: 25–64 years, mean age: 46 years). Apache II scores ranged from 5 to 14. Pancreatic necrosectomy was performed by laparoscopic transperitoneal approach in 12 patients (transmesocolic, 4 patients; transgastrocolic, 6 patients; and gastrohepatic omentum, 2 patients), by retroperitoneal approach in 2 patients, and by a combination of methods in 1 patient (endoscopic transgastric drainage followed by laparoscopic intracavity necrosectomy). Relook laparoscopy was done in 5 patients to assess for residual necrosis.
Results:
All the patients tolerated the procedure well, and there was no mortality. Two of them had pancreatic fistula, which eventually responded to conservative treatment. Three patients were converted to open necrosectomy because of bleeding or difficulty to access the area of necrosis. The mean operating time was 120 ± 10 minutes. There were no postoperative complications related to the procedure itself, such as major wound infections, intestinal fistulae, or postoperative hemorrhage. Postoperative computed tomographic scans confirmed adequacy of debridement. The average length of hospital stay after surgery was 14 days.
Conclusions:
Minimally invasive necrosectomy is technically feasible and a body of evidence now suggests that acceptable outcomes can be achieved. There are no comparisons of results available, either with open surgery or among different minimally invasive techniques.
Introduction
Materials and Methods
Between 2006 and 2010, 15 patients with infected pancreatic necrosis underwent minimally invasive pancreatic necrosectomy (11 men, 4 women; age group: 25–64 years, mean age: 46 years). Apache II scores ranged from 5 to 14. Pancreatic necrosectomy was performed by laparoscopic transperitoneal approach in 12 patients (transmesocolic, 4 patients; transgastrocolic, 6 patients; and gastrohepatic omentum, 2 patients), by retroperitoneal approach in 2 patients, and by a combination of methods in 1 patient (endoscopic transgastric drainage followed by laparoscopic intracavity necrosectomy). Relook laparoscopy was done in 5 patients to assess for residual necrosis.
Technique
Initial access was always by open technique in all patients, and the rest of port placement was guided by preoperative computed tomography (CT) localization of the site of pancreatic necrosis and by laparoscopic visualization. There were 3 conversions, 2 due to intraoperative bleeding and 1 secondary to inaccessibility of the site of necrosis. The timing of necrosectomy was 25–42 days, with a median of 34 days. Preoperative CT-guided pigtails were put in 3 patients.
Site of necrosis
Two patients had necrosis localized to the head, 11 patients had necrosis involving the body and tail, and 2 patients had necrosis localized to the tail.
Laparoscopic transperitoneal approach
Selection of patients for laparoscopic transperitoneal necrosectomy was based on the site of necrosis on CT abdomen (Fig. 1) and accessibility on laparoscopic visualization. It was done on well-localized infected pancreatic necrosis. Patients with multiloculated collections and inaccessible collections on CT abdomen and very sick patients with coagulopathy were excluded.

Infected pancreatic necrosis.
Two patients had pancreatic necrosis bulging through the gastrohepatic omentum (Fig. 2a). It was drained laparoscopically after opening the gastrohepatic omentum. Thorough pancreatic necrosectomy was done under vision, and drains were placed through port sites and irrigated.

The approach to the necrosis was decided based on intraoperative finding. Infected pancreatic necrosis bulging through (
Six patients had pancreatic necrosis involving the body and tail of the pancreas situated in the retrogastric region but bulging through the gastrocolic omentum (Fig. 2b). It was approached laparoscopically by passing scope through the gastrocolic omentum (Fig. 3). Complete cavity was evacuated, and two drains were placed and daily irrigated till the contents cleared up. One patient developed pancreatic fistula, which required endoscopic PD stenting after MRCP demonstrated disruption of the pancreatic duct. Fistula healed with conservative treatment after 2 months.

Infected pancreatic necrosis bulging through the gastrocolic omentum: (
Four patients had pancreatic necrosis in the peripancreatic region extending to the anterior pararenal space and bulging through the mesocolic omentum (Fig. 2c) as demonstrated by CT scan and on laparoscopic assessment. The fluid collection was approached laparoscopically through the mesocolic omentum, pancreatic necrosectomy was done, and infected fluid collection was drained. Postoperatively, 1 patient developed a pancreatic fistula, which gradually reduced with conservative treatment. One patient had intraoperative bleeding requiring conversion (Fig. 4b).

Infected pancreatic necrosis bulging through the mesocolic omentum: (
Technique of retroperitoneal necrosectomy
CT-guided small caliber percutaneous drains were placed by the radiologist into retroperitoneal collections through as a straight tract. The drain track was dilated using a seldinger technique, nephroscope was placed in the cavity (Fig. 5), and semisolid necrotic tissue was removed piecemeal using continuous saline irrigation. This was achieved using various accessories including biopsy forceps and baskets. A large tube drain was passed for postoperative lavage and continued until the fluid cleared. One patient had optiview trocar introduced over a guidewire for initial entry.

Retroperitoneal pancreatic necrosectomy: (
Combination of methods of pancreatic necrosectomy
A 48-year-old lady presented with walled off pancreatic necrosis at 6 weeks after acute attack of severe pancreatitis. She was breathless at rest, with huge distention of abdomen secondary to large cystic collection (Fig. 6).

Walled off pancreatic necrosis: (
As the site of necrosis was retrogastric, abutting the posterior wall of stomach, endoscopic transgastric drainage was done through the posterior wall of the stomach under endoscopic ultrasonography (EUS) guidance (Fig. 7), 4.5 L fluid was evacuated, and 2 stents were placed. As there were large vessels and extensive amount of necrosis, a laparoscopic necrosectomy at 2nd stage was done.

Endoscopic transgastric drainage of pancreatic necrosis.
Three days later, laparoscopic drainage was attempted but attempts at entering the peritoneum at two sites resulted in entry directly into the cyst. So intracavity debridement was done using hydrodissection, drains were placed, and cavity was irrigated daily.
Relook laparoscopy was done after 7 days. CO2 was insufflated through the previously placed drain. A trocar (5/10 mm) was inserted through the drain by cutting the drain and simultaneously it was advanced under local anesthesia (Fig. 8). Remnant necrosis was removed by hydrodissection (Fig. 9). Initially, we did this in all 3 patients because of our limited experience with laparoscopic necrosectomy, but now we do it in selected patients based on clinical condition and have done in 5 patients who had residual collections on CT abdomen and signs of sepsis.
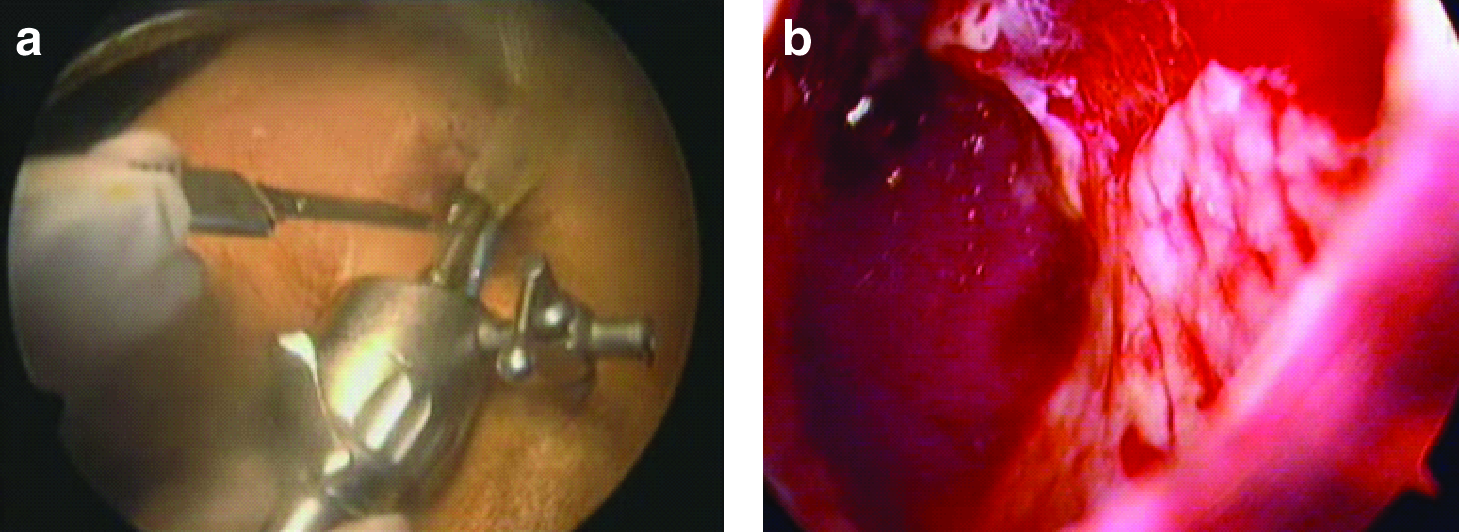
Relook laparoscopy in a previously done pancreatic necrosectomy: (
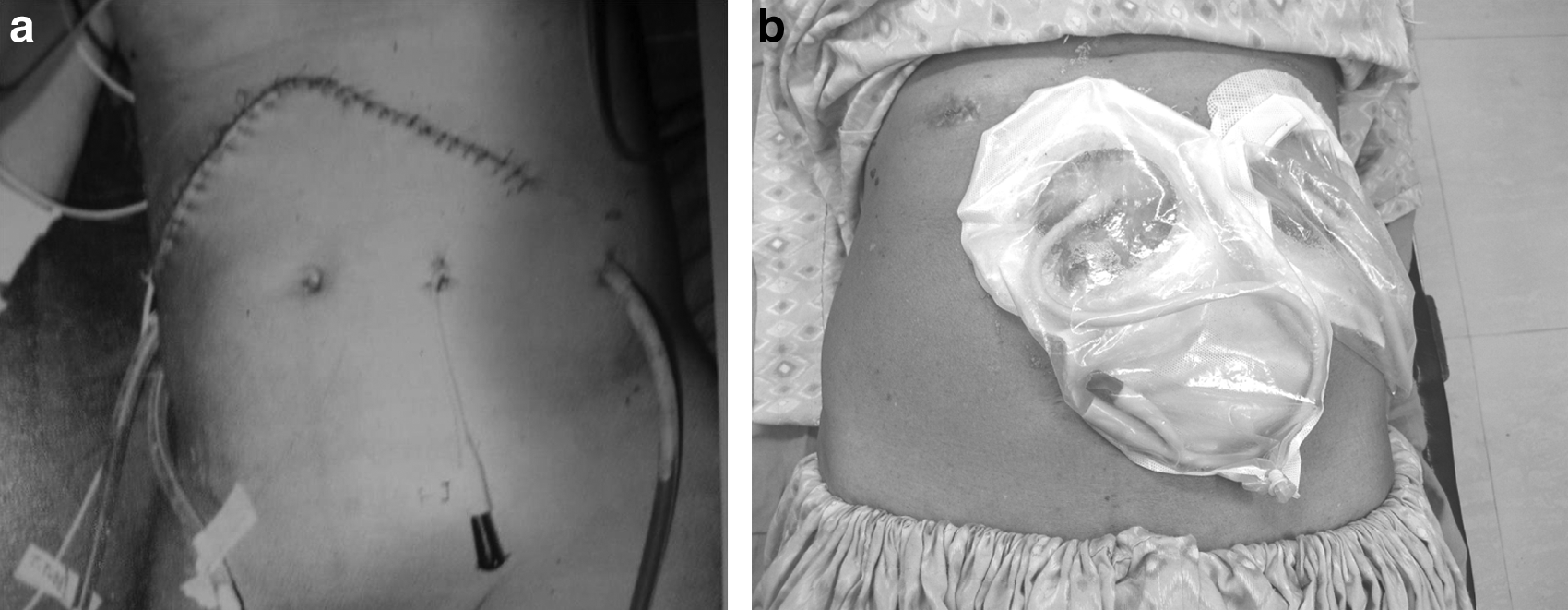
Postoperative picture after (
Discussion
Pancreatic necrosis occurs in 15%–25% of all attacks of acute pancreatitis and becomes infected in 40%–70% of necrosis,2,3 with an associated considerable rise in the risk of death. Mortality is high (20%–70%), especially when the necrosis is infected. 3 It is the most severe end of a spectrum of inflammation associated with pancreatitis. Inflammation causes cell death with resultant devitalized tissue, which is likely to become infected. The amount of necrotic tissue is the strongest predictor of mortality in this condition. The process of maturation or “organization,” with separation and partial liquefaction of the solid components within a collection, takes in excess of 12 weeks to complete.
Minimally invasive approach for management of infected pancreatic necrosis
A secondary infection of the necrosis demonstrated by a fine-needle aspiration under guidance of CT is an indication for surgical debridement and drainage. 4 The treatment of infected pancreatic necrosis and acute peripancreatic fluid collections has evolved significantly over the last few years. More recently, the preceding methods of operative debridement and drainage have been accomplished laparoscopically. An increasing number of reports have described the endoscopic drainage of infected pancreatic fluid collections.
The rationale for minimally invasive approaches is to minimize perioperative and postoperative stress in seriously unwell patients with multiple organ system failure. It may also extend indications for intervention to patients otherwise unfit for surgery. Additionally, these techniques may be used to initially control sepsis and thus usefully delay more major surgery until there is better demarcation of necrotic tissue.
Laparoscopic techniques via a transperitoneal approach is feasible, although occasionally an incomplete procedure because the viscosity of necrosis makes removal of the material difficult. It has the advantages over open necrosectomy in that it achieves the same objectives but with little tissue mortality and morbidity. It causes less tissue aggression and pain, and fewer laparotomy-associated hernias. The main disadvantages are rigidity of instruments and limitation of operating field, difficulty with evacuation and aspiration of necrotic materials due to its viscous consistency, formation of enterocutaneous or pancreatic fistulas, and infection of abdominal cavity. It is possible that some critically ill patients with severe acute pancreatitis may experience intraabdominal hypertension and abdominal compartment syndrome.
Transperitoneal laparoscopic pancreatic debridement using traditional laparoscopic surgery or the first-generation hand-access devices through a retrocolic access to the lesser sac have been previously described in anecdotal case reports. The perceived difficulty of the laparoscopic procedure for pancreatic debridement has led to the exploration of alternative minimal access retroperitoneal approaches using videoscopic and endoscopic approaches.4–6 Carter initially reported on 10 patients in whom percutaneous access to the necrosis cavity was obtained; the cavity was dilated to a final size of 30F, allowing the insertion of an operating nephroscope to remove some of the necrotic material in a piecemeal fashion. Multiple procedures were required to adequately drain all the necrotic tissue with this technique.
In 1996, Gagner reported his experience with the laparoscopic treatment of acute necrotizing pancreatitis in 8 patients by utilizing one of three approaches—transgastric, retroperitoneoscopic, and retrogastric/retrocolic. 7 He reported a high morbidity rate and a need for reintervention for persistent sepsis in few patients. Hamad in 2000 described laparoscopic pancreatic necrosectomy. 8 Horvath and colleagues 9 have reported on a promising videoscope-assisted retroperitoneal approach, in which a small subcostal flank incision is used to access the retroperitoneal space through which a videoscope is inserted through a port; debridement is accomplished with hydrodissection and long laparoscopic spoon forceps inserted through a second port. 9 Ammori described the laparoscopic transgastric pancreatic necrosectomy in 2002. 10 The transgastric route is more likely to avoid major vessels that may otherwise be encountered with the transmesocolic route (middle colic vessels) and the direct retroperitoneal approach (splenic vein), with the antecedent risk of visceral ischemia and bleeding.
In 2006, Parekh described hand-assisted laparoscopic approach for draining infected pancreatic necrosis. 11
Variations in the target lesions (location, fluid/mixed/solid, early/late, sterile/infected, single/multiple, wall thickness) and in the patients (comorbidity, habitus, degree of organ dysfunction) require an individually tailored and flexible approach to the treatment of pancreatic necrosis. 12 The development of MIN has led to two contrasting philosophies. The first advocates an orthodox “step-down” approach in which open necrosectomy plays a primary role, with less invasive methods used for residual or subsequent collections. The second, or “step-up,” approach relies initially on less invasive techniques, with open necrosectomy used as a last resort. 12 Promising technologies that require evaluation in this context are laparoscopic ultrasonic aspiration and ultrasonic tissue emulsification, but more efficient mechanical devices may ultimately give way to a biological approach promoting accelerated liquefaction. 12
Role of relook laparoscopy
Relook laparoscopy is visualization of the debrided cavity after a period of time to assess for the completion of pancreatic necrosectomy. Completion necrosectomy can be done by placing ports through the previously placed drains in the debrided cavity under local anesthesia and sedation. It is similar to the multiple explorations, which were performed in the past to achieve complete necrosectomy albeit with little morbidity of repeated surgeries.
Conclusion
In conclusion, it is clear that the era of minimally invasive necrosectomy has arrived, but with a limited body of evidentiary support. Drainage of the infected cavity can be achieved through all the routes described. Different areas of the pancreas may be more amenable to one technique than others. The tail of the pancreas is less accessible to transgastric drainage, the body is less accessible to percutaneous approaches, and the head is less accessible to retroperitoneal or laparoscopic approaches. Some patients may require a combination of approaches to secure control. The selection of treatment must be guided by the need to ensure the availability of true multidisciplinary expertise in a specialist unit.
Footnotes
Disclosure Statement
No competing financial interests exist.