
Abstract
Abstract
Introduction:
The repair of large congenital diaphragmatic hernia frequently results in patch disruption and recurrence as patients grow in size. Absorbable meshes allow for ingrowth of endogenous tissue as they are degraded, providing a more natural and durable repair. The aim of this study was to compare the characteristics of the new diaphragmatic tissue between an absorbable biologic mesh and a nonabsorbable mesh for repairing diaphragmatic hernia in a growing animal model.
Methods:
The left hemi-diaphragm of twenty 2-month-old Yucatan pigs was nearly completely resected. Small intestinal submucosa (SIS; Cook Biotech, Lafayette, IN) and expanded polytetrafluoroethylene (ePTFE; W.L. Gore & Associates, Flagstaff, AZ) were randomly assigned to cover the defect in 10 animals each, and were survived for 6 months. During necropsy, newly formed diaphragmatic tissue was evaluated and compared between the two groups.
Results:
At necropsy, the animals had tripled their weight. Patch disruption and herniation occurred in 3 animals in the ePTFE group and none in the SIS group. The SIS mesh had better integration to the chest wall (2.8 ± 0.2 versus 1.3 ± 0.3), more muscle growth within the newly formed diaphragmatic tissue (1.9 ± 0.2 versus 0.4 ± 0.2), and less fibrotic tissue (2.1 ± 0.5 versus 3.4 ± 0.4) than ePTFE. There was no difference between SIS and ePTFE in terms of adhesion scores to the lung (2 ± 0.4 versus 2.4 ± 0.4) and liver (1.8 ± 0.3 versus 2.2 ± 0.5).
Conclusion:
SIS allows for tissue ingrowth from surrounding tissue as it degrades, providing a more durable repair with 30% less incidence of herniation in a porcine model. As the diaphragm grows, SIS resulted in a more natural repair of the defect with more tissue growth, better tissue integration, and a comparable adhesion formation to ePTFE.
Introduction
The most common prosthetic material used for CDH repair is polytetrafluoroethylene (PTFE; Gore-tex®; W.L. Gore & Associates, Flagstaff, AZ). 4 Concerns have been raised about the use of this material because, as an infant grows, the implanted prosthetic covers a progressively smaller cross-sectional area of the surface of the diaphragm. This has been associated with hernia recurrence, 5 chest wall restriction, and deformity. 6 Depending on the patient population, the material used for repair, and the requirement of extra-corporeal membrane oxygenation (ECMO), authors cite recurrence rates of CDH between 13% and 80%.5,7–9
The search for an ideal material for the repair of CDH continues. Efforts have been directed toward the use of different materials, mainly biodegradeable prostheses that function as a lattice, allowing for ingrowth of endogenous tissues. In the study comparing small intestinal submucosa (SIS) versus acellular dermis (Alloderm) as alternatives for CDH repair, Dalla Vecchia et al. 10 reported adequate integration of the prostheses in rats; however, no evidence of skeletal muscle ingrowth was found. When comparing PTFE versus fluorinated polyester, Kimber et al. reported a strong foreign-body reaction to the PTFE, no cellular ingrowth, and marked fibroblast response in peripheral tissues. 11 The rapid and sustained incorporation of fluorinated polyester made hernia recurrence less likely than with PTFE. Lantis et al. compared PTFE with a collagen prosthetic patch. 12 They found that the PTFE resulted in a higher adhesion grade, greater inflammatory response, and no tissue ingrowth. Hajer et al. suggested this lack of biological union between the sutured PTFE patch and the diaphragm tissue remnant as the likely cause of recurrence. 5
Almost consistently, investigators have used a small animal model to study the effects of growth on diaphragmatic repairs.10–13 One large animal model that has been established is a lamb model for CDH, as written about by Dario Fauza et al. His group has published numerous articles revolving around diaphragmatic repair through fetal tissue engineering.14,15 Still, studies on patch repairs in a growing animal model are less common. 16
The purpose of this study was to compare the properties of the new diaphragmatic tissue formed after CDH repair between a biodegradable prosthetic material and a nonabsorbable mesh in a growing animal model. For this purpose, a large animal model of a diaphragmatic defect repaired in a young animal was developed and animals were allowed to grow to reproductive age. Attention was paid to the following end points: recurrent hernia formation, quality of newly formed diaphragmatic tissue (NFDT), adhesion formation, and tissue integration of the prosthesis to the remaining diaphragmatic muscle.
Methods
Animal model
This study was approved by the Institutional Animal Care and Use Committee of Emory University. The animals utilized in this study were 2-month-old Yucatan miniature pigs (mean weight, 10.5 ± 0.5 kg). The principal reason for this selection is the fact that these animals grow rapidly and reach sexual maturation at the age of ∼8 months. With this, one would expect at least a threefold increase in weight after 6 months, the usual breeding age. Twenty pigs were randomized to receive a patch made of either an 8-ply SIS (Cook Biotech, Lafayette, IN) or 2-mm-thick expanded PTFE (ePTFE)-derived soft tissue, the Dual Mesh Plus® (Gore-Tex; W.L. Gore & Associates).
Prosthetic materials
Expanded polytetrafluoroethylene
Two-millimeter-thick ePTFE-derived soft tissue patch, the Dual Mesh Plus (Gore-Tex; W.L. Gore & Associates): This is the most common graft material used for CDH repairs. One side of this mesh has a pore size of <1 μm intended to minimize tissue in-growth or attachment and therefore limiting adhesion formation. With this, it can be placed in direct contact with abdominal viscera. The opposite surface has a microstructure with an average pore size of 22 μm, allowing for host tissue incorporation. Integration with host tissue, particularly in the areas of anchorage to the diaphragmatic wall, is not as thorough. Consequently, strength and resistance to traction are lower than that achieved with macroporous prostheses.
Small intestinal submucosa
The 8-ply SIS (Cook Biotech): This patch is made of the submucosa of pig small intestine that has been rendered free of any cells. Only the structural tissue framework remains. One main characteristic of SIS is that is allows native connective tissue to grow into it as it slowly degrades. Eventually, after 6–8 weeks, the mesh is completely replaced by native tissue, a neodiaphragm. This important feature may allow for the NFDT to remain incorporated with native tissue as it grows in size, preventing repeat herniation while preserving diaphragm function.
Pilot study
Before initiating our study, a pilot study was performed utilizing four 2-month-old animals, 2 with each type of graft. Each was survived for a 2-week period. The purpose of this pilot was to become familiar with the handling properties of each material, refine operative technique, postoperative management, and the treatment of any complications, should they occur. At the end of the 2-week period, the animals were euthanized according to the American Veterinary Association protocol, and a necropsy was carried out taking samples from the diaphragm for histological evaluation.
Operative technique
Under general anesthesia, supine position, and sterile conditions, a 10-cm incision was performed 1 inch below and parallel to the left costal margin. The abdominal contents were retracted to expose the left hemidiaphragm, and using electrocautery, a near complete resection of the diaphragm was performed. An ∼1 cm circumferential margin of muscle remained after resection (Fig. 1). The type of graft material to be used in the repair was randomly assigned after completion of the diaphragmatic resection. The graft was tailored to the size and shape of the defect, and in the use of the ePTFE, positioned with the rough side facing the thorax and the soft, nonadhesive side facing the abdomen (Fig. 2).
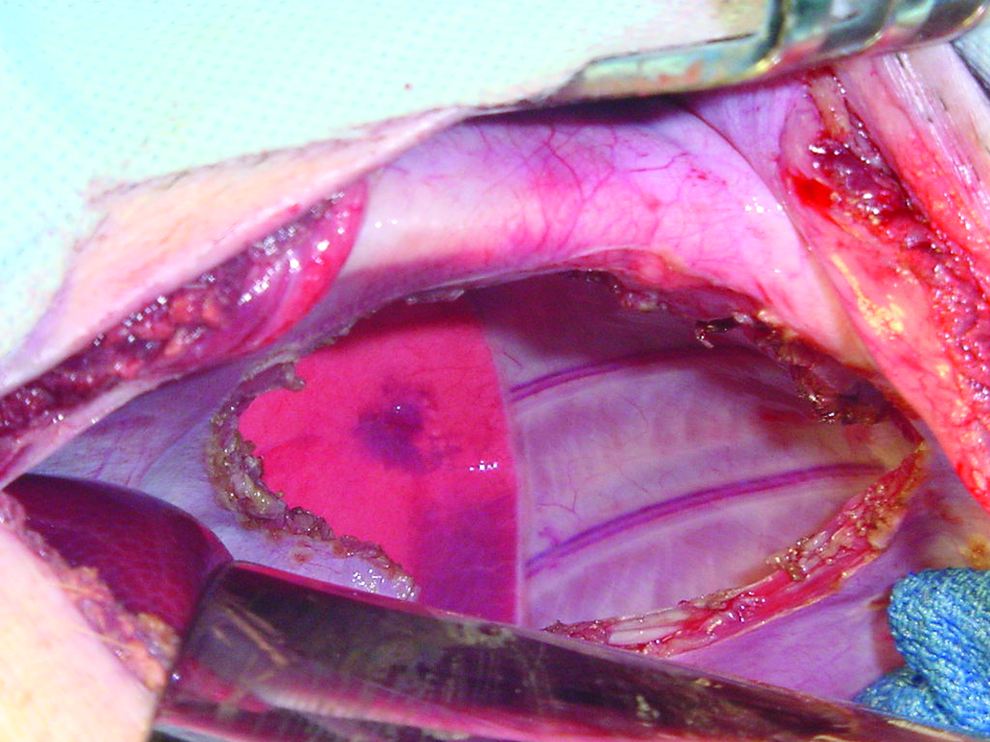
Resection of left diaphragm leaving a 1-cm margin of muscle to allow adequate mesh fixation.

Repair of the diaphragmatic defect with ePTFE graft using running sutures. ePTFE, expanded polytetrafluoroethylene.
In the 4 animals of the pilot study, the grafts were fixed using 3-0 prolene (Surgipro®; USSC, Norwalk, CT) simple interrupted sutures, spaced 1 cm apart. Hyperinsuflation of the lungs was performed before placement of the final suture to verify lung expansion and evacuation of the pneumothorax. During the pilot study, the immediate postoperative period was complicated with inadequate ventilation requiring reintubation of 2 animals. This was due to air leaking between the sutures when chest wall expansion created negative pressure. Based on this experience, the fixation technique was changed to a running suture for study. No thoracostomy tube was necessary.
Postoperative care
The animals were allowed a liquid diet 6 hours after the procedure. If the liquid diet was well tolerated, a bland diet was allowed at 12 hours and normal chow was offered 24 hours after the procedure. The animals were monitored and their progress recorded as per standard postoperative protocols. Daily vital signs and weekly weights were recorded in individual charts. No other procedures or treatments were performed during the postoperative period.
Necropsy evaluation
Six months after the operation the animals were euthanized in accordance with the American Veterinary Medical Association protocol. A necropsy was then carried out and the diaphragm was evaluated. The investigators performing the necropsy were blinded to the material type used in the animal. For exposure and evaluation of the diaphragm, two transverse incisions were performed above and below the diaphragm, connected by a distal sternotomy. Special attention was directed to evaluate the presence of herniations. Additionally, an assessment and classification of any adhesion formation from both the lung and abdominal contents to the diaphragm was carried out according to a frequently used scale.17–20 The amount of surface area of the NFDT covered by muscle tissue was assessed and scored by 2 surgeons independently. The following is the scale for scoring for NFDT covered by muscle tissue: 0 (none), 1 (<25%), 2 (25%–50%), 3 (50%–75%), and 4 (>75%).
Four 0.5 × 0.5 cm2 sections of the NFDT, as well as the lung/diaphragm and liver/diaphragm interfaces were taken and processed for histological evaluation. These tissue samples were subjected to conventional light microscopy techniques (hematoxylin–eosin stain) to evaluate the amount of inflammation, fibrosis, and neovascularization. Integration and native tissue ingrowth was also assessed. The pathologist was blinded to the type of material used in the animal. Amount of fibrosis was scaled with the following criteria: 0 (none), 1 (minimal), 2 (mild), 3 (moderate), and 4 (severe). The integration scale was based on histological findings of connective tissue ingrowth using similar criteria. The scoring criteria are summarized in Table 1.
Adhesion formation scale: macroscopic classification of adhesions to thoracic and abdominal organs.20–23 Tissue integration, fibrosis, and new muscle tissue were scored by pathologists based on histologic findings.
Tissue integration based on amount of connective tissue documented at the diaphragm to chest wall junction.
Fibrosis and new muscle tissue scores were given using representative tissue samples taken from the middle of the newly formed diaphragmatic tissue.
Analysis
Continuous nonparametric data were compared between groups using a Mann–Whitney U-test. Categorical data were analyzed using Fisher's exact test. Ordinal data were analyzed using Wilcoxon matched-pairs signed-ranks test. A P < .05 was considered significant. Data derived from the study are presented as mean ± standard error of the mean.
Results
Pilot study
As previously stated, the animals in this group had inadequate immediate postoperative ventilation and 2 of them had to be re-intubated for a period of 2 hours, after which they were extubated without any pulmonary consequences. One of the animals had a postoperative right side pneumothorax that was managed without placement of a chest tube. The 4 animals were euthanized at 2 weeks for evaluation. The mean weight at the time of necropsy was 12 ± 0.3 kg. There was no difference in adhesion scores from the diaphragm to the liver (1.5 ± 0.5 versus 1 ± 0), lung (1 ± 0.5 versus 1.5 ± 0.5), or chest wall (1.5 ± 0.5 versus 2 ± 0). Histological analysis revealed a similar degree of fibrosis in the lung/diaphragm (1.5 ± 0.5 versus 1 ± 0.5) and liver/diaphragm (1.9 ± 0.2 versus 2.1 ± 0.4) interface between SIS and ePTFE. Histological evaluation of tissue integration also scored similarly between SIS and ePTFE (2 ± 9 versus 1.5 ± 0.5).
Six-month results
The immediate postoperative period and recovery in the animals was uneventful. No pulmonary complications were noted. The animals did not receive any medications that would interfere with the normal healing process. Two of the animals developed a superficial would infection, which was treated with topical antibiotics. One animal in the ePTFE group developed sudden dyspnea and died 3 weeks after the operation. A detachment from the medial side of the mesh was found during necropsy, and a complete herniation of the stomach into the left hemithorax was established as the cause of death. The remaining animals survived until the completion of the study.
The mean weight at the time of the necropsy was 32.4 ± 2 kg, marking a threefold increase in mean weight over the course of the study. At the time of necropsy, 2 animals from the ePTFE group were found to have a DH along the posterior aspect of the thoracic wall. No DH was found in the SIS group, but this difference did not reach statistical significance. There was no difference in adhesion scores between the ePTFE and the SIS group in either liver-to-diaphragm adhesions (1.2 ± 0.3 versus 1.5 ± 0.5, respectively) or lung-to-diaphragm adhesions (2.8 ± 0.5 versus 2.5 ± 0.4, respectively).
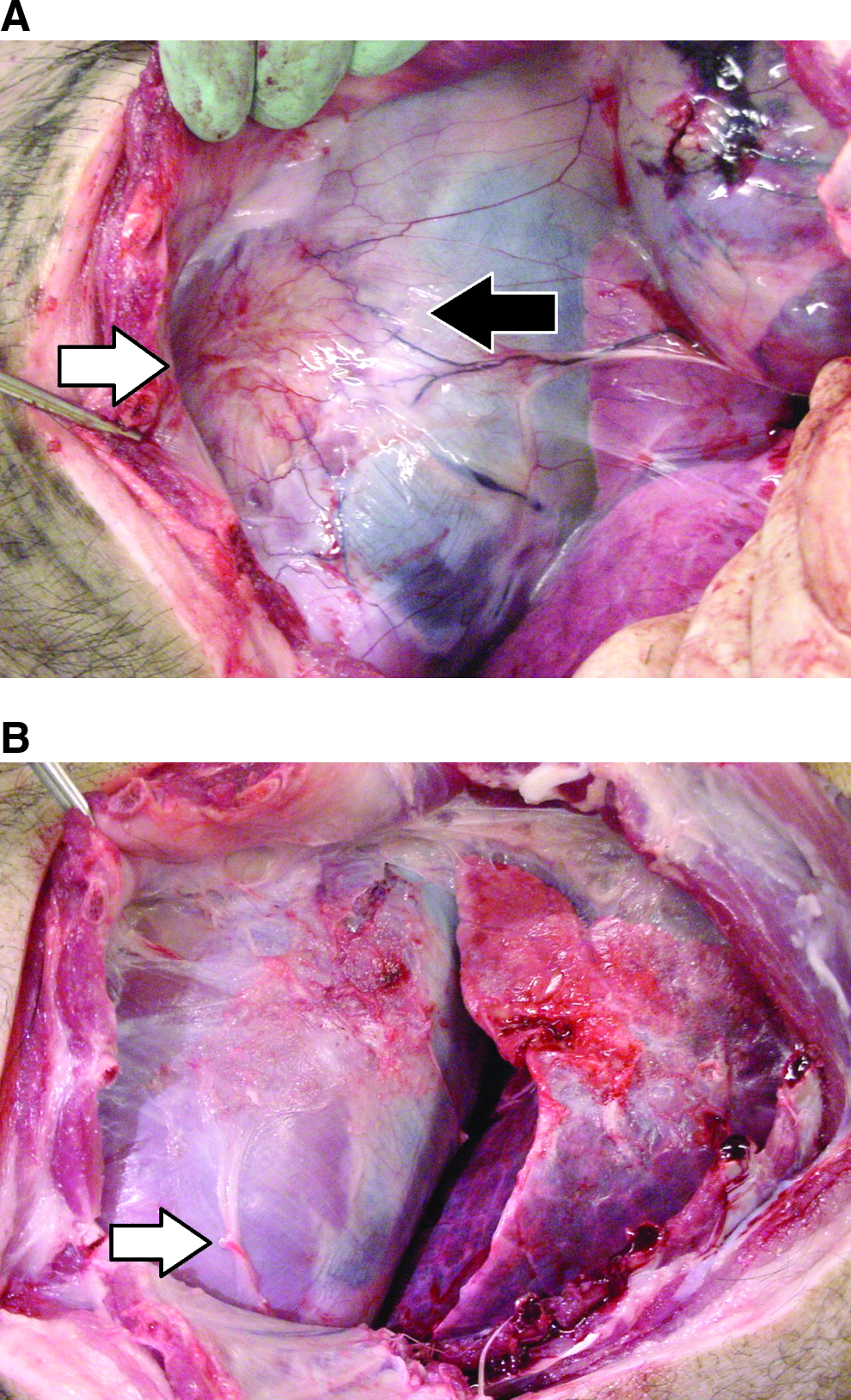
In all animals, the SIS graft was completely replaced by new tissue and no longer identifiable on histology. In animals with ePTFE, the grafts were covered with a thick fibrotic capsule and found to be folded. It was also found in this group that the surface area of diaphragm covered by ePTFE prosthesis was smaller than the original size of the graft. The histological score for degree of tissue integration in the chest wall/diaphragm was higher in the SIS group than in the ePTFE group (2.8 ± 0.2 versus 1.3 ± 0.3) (P < .05). The amount of fibrotic tissue in the NFDT in the ePTFE group was significantly higher than in the SIS group (3.4 ± 0.4 versus 2.1 ± 0.5) (P < .05) (Table 2). The amount of surface in NFDT covered by muscle tissue was significantly higher in the SIS than in the ePTFE groups (1.9 ± 0.2 versus 0.4 ± 0.2) (P < .05) (Fig. 3A, B).
(
Wilcoxon matched-pairs signed-ranks test: P < .05.
ePTFE, expanded polytetrafluoroethylene; SIS, small intestinal submucosa.
Discussion
This animal model proved to be a suitable large animal model to study DH repair in a growing subject. Herniations that were found during necropsy replicated what has been described in humans after CDH repair, occurring in the posterior aspect of the thoracic wall. The rate of herniation that we observed after ePTFE repair was similar to that which has been documented in other clinical trials.21,22
In this study, the herniation that occurred 3 weeks after surgery was possibly secondary to a technical error. However, it occurred in animal no. 17, and histologic findings revealed a severe foreign-body reaction, pointing to inadequate mesh integration. The herniations found at 6 months are likely due to inadequate mesh incorporation to the remaining diaphragmatic tissue. In those cases, the mesh had pulled away from the tissue as the growing chest wall subjected it to tension. Although the difference did not reach statistical significance, there is an important clinical implication of 30% recurrence for this operation, especially given that that recurrence rate for SIS was 0%.
These results confirm findings from previous studies. The adhesion formation from the diaphragm to the lung and liver were as expected. The rough side of the prosthesis is created to stimulate tissue incorporation to the surrounding tissue. Conversely, the soft side resulted in only minimal adhesions in both materials, supporting their use in contact with abdominal contents. The histology results confirm these findings, with no difference in amount of fibrosis in the lung/diaphragm and the liver/diaphragm interfaces between both groups.
As previously reported, ePTFE resulted in a poor integration in the areas of anchorage, which could predispose to herniation when subjected to tension as the diaphragm grows. 23 SIS resulted in better tissue integration than ePTFE evidenced by the higher amount of collagen-forming fibroblasts in the chest wall/diaphragm interface. Furthermore, almost 50% of the surface area of the NFDT was covered by skeletal muscle tissue in the SIS group. This was significantly more than the amount of endogenous tissue growth stimulated by the ePTFE. It is unclear why skeletal muscle tissue replaced the SIS graft compared to the thick fibrotic capsule, which was found on the ePTFE; however, it is likely due to the foreign body response to the ePTFE. The histologic findings corroborated these results, with higher amount of fibrotic tissue found in the NFDT in the ePTFE group than the SIS group. This is a significant finding in this study, since the muscle tissue that grows might not only prevent recurrent hernias, but also perhaps have capability of contracting, aiding in respiration. Additional follow-up studies to consider are evaluation of the NFDT strength, diaphragmatic function, as well as evaluation of newer materials.
As with all animal studies there are limitations to this experiment that should be discussed. This animal model utilized healthy 2-month-old pigs as compared to neonates, which are most frequently encountered in the clinical setting of CDH. Tissue strength and healing may be different in the neonate as compared to a 2-month-old pig. Likewise, the pigs used in this study had normal lung tissue and function versus the hypoplastic lung parenchyma encountered in infants with CDH. It is possible that a hypoplastic lung could impact the overall ingrowth of the patch. A potential drawback in the study is the growth rate of the pig compared to that of an infant. Perhaps the rapid tissue growth seen in the pig model favors the incorporation of a biologic scaffold over a synthetic mesh. Another possible factor which could impact ingrowth is the small rim of muscle which was left during the diaphragm excision. In many cases, what is encountered in infants is an agenesis of the diaphragm or absence of the posterior aspect of the diaphragm. Since all animals had the same amount of tissue left behind at the excision, the two repairs can be compared head to head in terms of ingrowth and hernia recurrence. However, consideration of this point should be taken in translating these data directly to humans. Another concern is that there are likely different forces on the diaphragm of the pig compared to a human, as animals spend the majority of their time walking on “all fours,” thereby possibly influencing the presence of different stress patterns on the grafts, and altered frequency of herniation.
Conclusion
This study has demonstrated in a growing large animal model designed to evaluate repair of a DH using ePTFE and SIS, that in a porcine model, SIS mesh is an effective prosthesis with completely degradable properties. It was associated with no recurrences, minimal abdominal adhesion formation, adequate tissue ingrowth and fixation, and the stimulation of a large amount of new muscle tissue ingrowth.
Footnotes
Disclosure Statement
No competing financial interests exist.