
Abstract
Abstract
Background:
Accidental splenic laceration and hemorrhage during natural orifice translumenal endoscopic surgery (NOTES) can lead to life-threatening consequences. The NOTES approach may need to be aborted in these circumstances for a standard laparoscopy or laparotomy.
Aim:
To determine the feasibility of endoscopically managing intraoperative splenic laceration and hemorrhage during NOTES using standard endoscopic tools.
Methods:
Nine pigs underwent transcolonic endoscopic surgery, and 18 intentional splenic lacerations were made. Animals were treated as follows: (1) control group with no therapy (n = 3), (2) endoscopic tamponade/packing (n = 3), and (3) endoscopic hemostasis with bipolar cautery (n = 12). A blinded second endoscopist performed NOTES exploration and attempted to identify the site and treat the laceration in 3 cases. The colonic incision was closed using endoclips in the survival studies. Necropsy was performed immediately after surgery in acute cases and at the end of 1 week in the survival cases.
Results:
Bleeding persisted beyond 10 minutes in all control cases without therapy. In the tamponade group, bleeding persisted beyond 17 minutes in 2 and a large clot formed at 12 minutes in 1 case that precluded further assessment. Bleeding was controlled endoscopically using standard bipolar cautery in all animals (mean time: 12 minutes). All lacerations were identified and managed by the blinded endoscopist. Survival animals had an uncomplicated postoperative course. No bleeding was seen at necropsy.
Conclusion:
We demonstrate the management of intraoperative splenic hemorrhage during NOTES using standard endoscopic tools. The site of splenic bleeding could be correctly identified and treated in a blinded fashion.
Introduction
For natural orifice translumenal endoscopic surgery (NOTES) to gain general acceptance as a minimally invasive approach, it must be feasible to manage intra-abdominal complications such as iatrogenic injury to abdominal structures and bleeding. This was highlighted in the White Paper as a key element for future NOTES research. 6 To date, little published data exist on the feasibility of managing solid organ hemorrhage with endoscopic techniques during NOTES.7,8 The aim of our study was to determine the feasibility of endoscopically managing intraoperative hemorrhage from accidental splenic laceration arising during NOTES using standard endoscopic tools.
Materials and Methods
Overview
Nine female pigs (sus) underwent transcolonic NOTES procedures. Transcolonic peritoneal access was obtained, and an intentional splenic laceration was created to simulate an iatrogenic intraoperative complication. Control groups included no therapy and endoscopic tamponade/packing. Hemostasis was attempted with a standard commercially available endoscopic bipolar electrohemostasis catheter. The colonic incision site was then closed using endoclips. The study was approved by the Institutional Animal Care and Use Committee (IACUC) at the University of Florida.
Animals
Female pigs (sus) weighing 60–80 lbs were obtained from the University of Florida Swine Unit (Gainesville, FL).
Endoscopes and instruments
Single- and double-channel gastroduodenoscopes (Olympus Medical Systems Corporation, Tokyo, Japan) were used. Endoscopes were high-level chemically disinfected with 3.4% glutaraldehyde (Cidex Plus; Johnson and Johnson, Irvine, CA) and air-dried. Before each surgery re-usable endoscopic accessories were cleaned and high-level chemically disinfected with 3.4% glutaraldehyde.
Preoperative care
Animals were kept without food for 24 hours before surgery. For survival experiments, preoperative enrofloxacin 5 mg/kg intramuscular (IM) injection was administered on the day of surgery.
Anesthesia
All procedures were performed under general endotracheal anesthesia with inhaled isoflurane (1%–3.5%). Pigs were preanesthetized with Telazol 4 mg/kg IM, ketamine 2 mg/kg IM, xylazine 2 mg/kg IM, and atropine (0.04 mg/kg) IM.
Surgical procedure
Transcolonic access
Transcolonic access to the peritoneal cavity was obtained as previously described. 9 After sequential sterile water enemas, antibiotic lavage (cefazolin) followed by internal instillation of povidone iodine solution was performed. The anus and perineum were cleaned with an external povidone iodine scrub. A high-level disinfected double-channel endoscope was inserted and a colotomy performed to access the peritoneal cavity.
Splenic laceration
Intentional 2 cm splenic lacerations were made using an electrocautery needle-knife (Boston Scientific, Natick, MA) to mimic accidental splenic injury and bleeding during NOTES. The length of the laceration was gauged by comparing it with an open biopsy forceps. A constant depth of the laceration was maintained by embedding the entire length of the needle into the splenic bed. All lacerations produced active and persistent bleeding. Active bleeding was defined as bleeding that persisted beyond 1 minute. This time was chosen as it is standard surgical practice to intervene for hemostasis if bleeding persists beyond 1 minute. The site was lavaged with sterile water and persistent bleeding was confirmed. Control splenic lacerations were performed in 3 cases where no therapy was applied (to assess if bleeding would stop spontaneously).
Hemostasis
Attempt at hemostasis was begun after detecting 1 minute of persistent bleeding. This time period was based on the assumption that if accidental splenic laceration and bleeding occurred during NOTES and was detected, it would be addressed immediately intraoperatively at this time rather than waiting for spontaneous resolution.
In the tamponade group, pressure was applied with a gauze for tamponade/packing after 3 splenic lacerations. Rolled and folded gauze was held with a forceps and Roth net passed through the working channel of the endoscope and pressed onto the bleeding site for physical tamponade.
A standard endoscopic 7F bipolar electrohemostasis catheter (Gold Probe; Boston Scientific) with a power setting of 30–40 W was used to achieve hemostasis in the bipolar cautery group (n = 12). This group included 3 cases where the laceration was performed by one endoscopist and a blinded second endoscopist who was not present at the time of the laceration then performed NOTES exploration and attempted to identify the site of bleeding and treat the laceration. The bipolar hemostasis catheter was pressed firmly along the splenic laceration for coagulation. Clotted blood was suctioned through the endoscope. Intermittent lavage was performed with sterile water to assess adequacy of hemostasis and to rule out persistent oozing of blood. Intraperitoneal pressure was monitored and controlled with a manometer (Fisher Scientific manometer, model 8205). Intraperitoneal pressure was decreased at the end of the procedure before withdrawing the endoscope to confirm cessation of bleeding. Endoscopic therapy was stopped when no further oozing was seen.
Time to achieve endoscopic hemostasis was recorded. The site was revisited 15 minutes after achieving hemostasis for endoscopic confirmation of complete bleeding control and was also confirmed by an independent observer. Hemostasis was considered successful if there was no evidence of bleeding when the site was re-examined 15 minutes after endoscopic therapy was stopped. If bleeding persisted and hemostatic therapy failed, the animal was to be euthanized. Euthanasia would also be performed in case of cardiovascular instability unresponsive to endoscopic hemostatic therapy.
Colotomy closure
The colonic incision was closed using endoclips (Resolution Clip; Boston Scientific).
Postoperative care
For survival surgeries (1 week survival period), analgesia was provided as per the following protocol: buprenorphine 0.01–0.02 mg/kg IM at the start of the procedure and then at 12 hours; flunixin meglumine 1.1 mg/kg IM at the end of the procedure; and then either or both drugs as needed beyond 24 hours. Regular diet was resumed the following morning. Animals were closely monitored daily for signs of distress, behavior changes, loss of appetite, and signs of bleeding and peritonitis (fever, abdominal pain, poor food and water intake, lethargy, and decreased activity).
Euthanasia and necropsy
Nonsurvival cases were euthanized immediately after surgery. Before euthanasia the animals were anesthetized with a ketamine (20–25 mg/kg)-and-xylazine (2–4 mg/kg) cocktail IM. They were then euthanized with ≥150 mg/kg pentobarbital sodium IV. After euthanasia, necropsy was performed, and the peritoneal cavity examined for abscess, bleeding, or perforation. A leak test was performed to confirm adequate colotomy closure in the nonsurvival animals. The gastrointestinal tract incision site and surgery site were assessed for complications.
Results
Eighteen intentional splenic lacerations were performed in 9 live anesthetized animals (7 acute nonsurvival and 2 survival studies) to mimic accidental splenic injury (Fig. 1). Intentional splenic lacerations were successful in all cases resulting in immediate and brisk bleeding (Fig. 2).
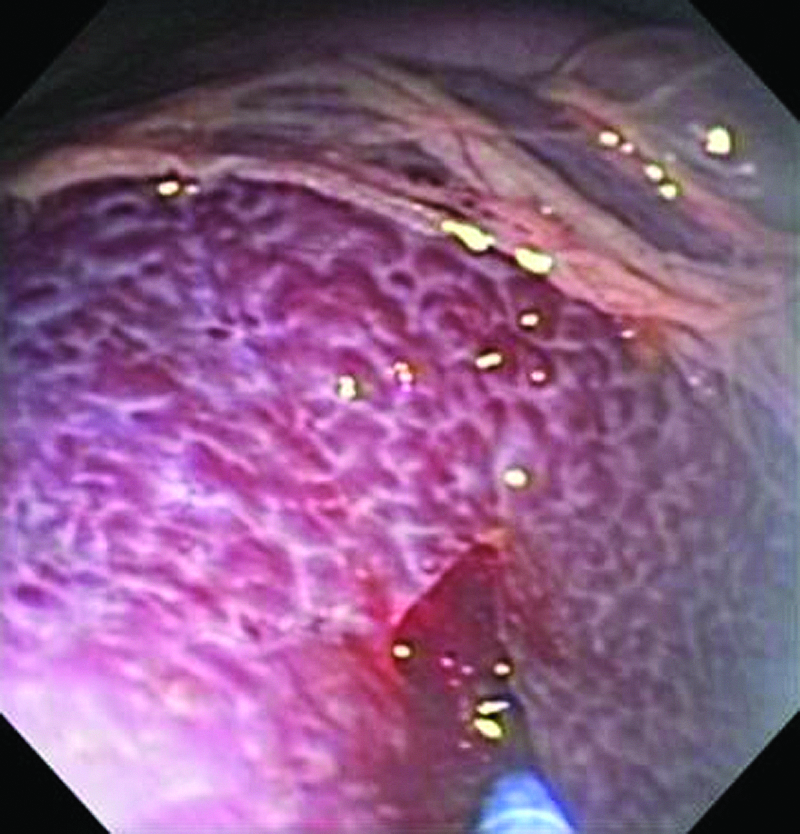
Splenic laceration. A needle-knife is used to perform an intentional splenic laceration.
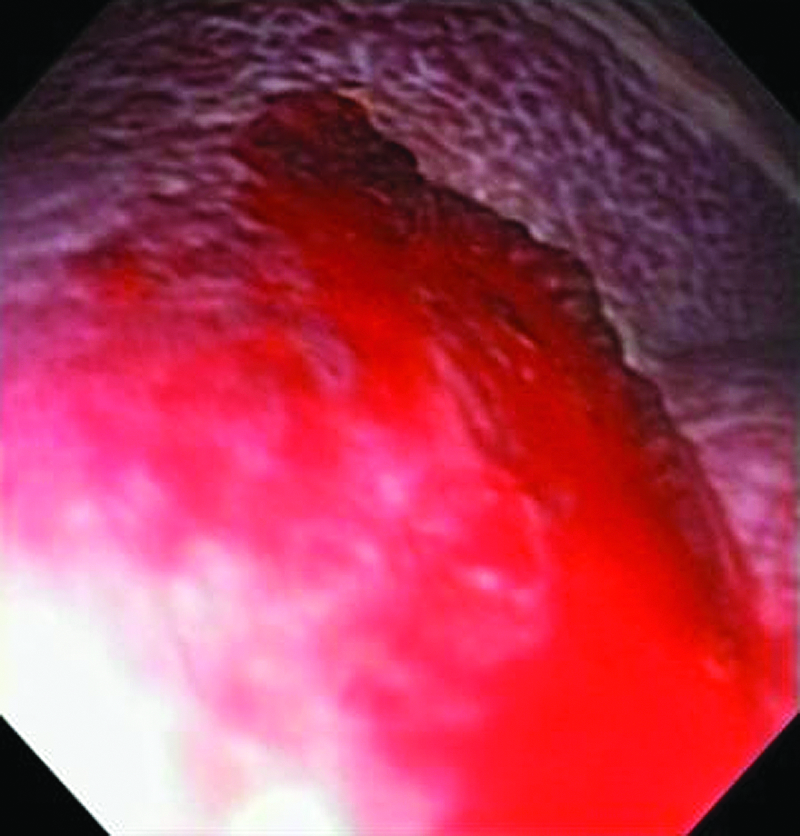
Splenic hemorrhage. Brisk and persistent bleeding is seen after splenic laceration.
In the control group, bleeding persisted beyond 10 minutes in all cases without any therapy and was confirmed by an independent observer. These animals were then euthanized. In the tamponade group, bleeding persisted beyond 17 minutes in two and a large clot formed at 12 minutes in 1 case that precluded further assessment of the bleeding site. These procedures were then terminated in light of persistent bleeding.
Hemostasis with a standard endoscopic 7F gold probe was achieved in all cases where it was attempted (Fig. 3A, B). The mean time to achieve hemostasis was 12 minutes. Repeated application of the bipolar probe with careful inspection of the bleeding site was necessary to achieve complete hemostasis (Fig. 4). All splenic laceration sites were correctly identified and treated by the blinded endoscopist who was not present at the time of the initial laceration performed by a different endoscopist.
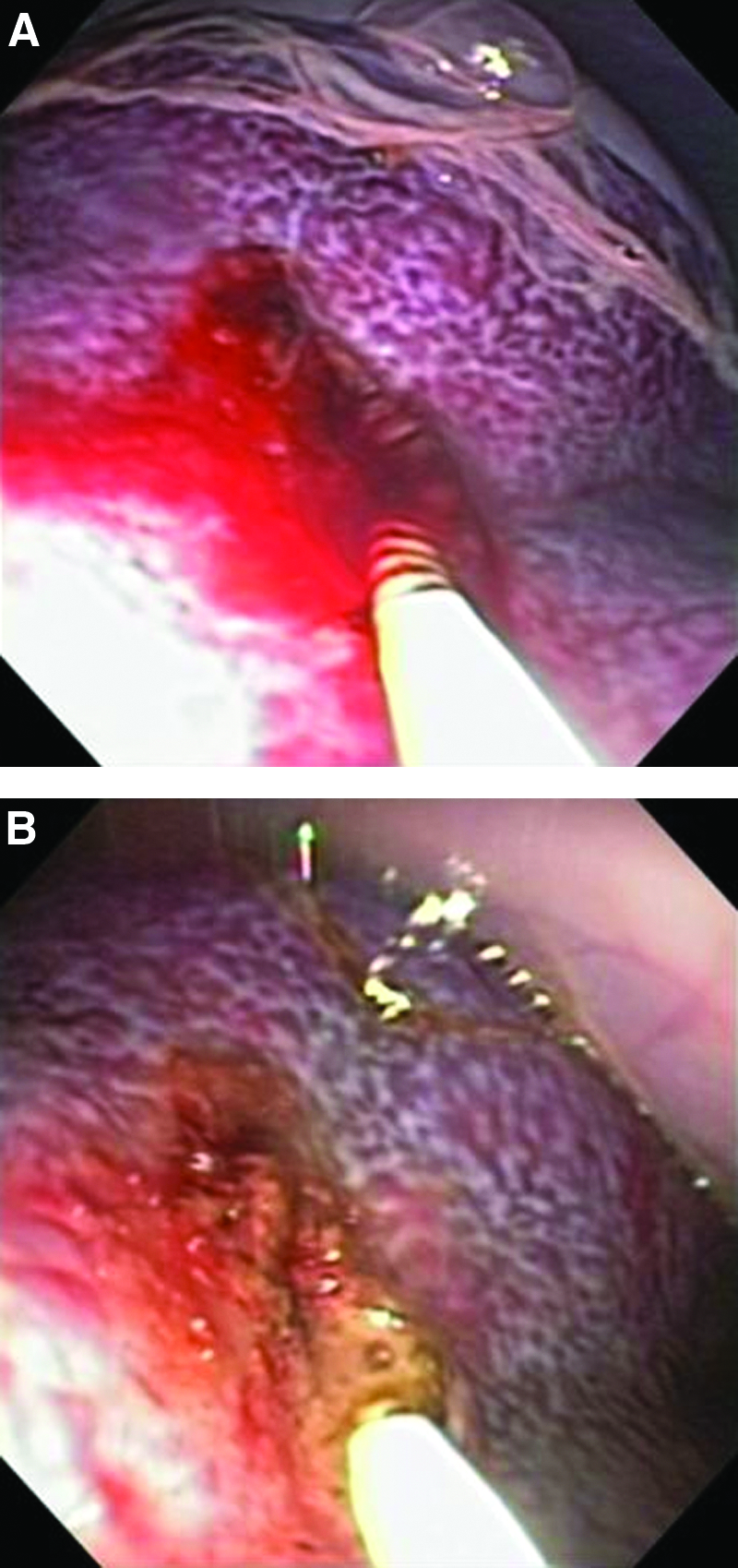
Endoscopic therapy of splenic hemorrhage.

Endoscopic view of the splenic laceration after successful hemostasis.
Survival animals were euthanized 1 week after surgery per protocol. Their postoperative courses were uncomplicated. These animals thrived and had liberal food and water intake and activity without event. There was no clinical evidence of peritonitis or bleeding.
Necropsy was performed in all cases. The omentum was seen adherent to the site of splenic laceration in one survival animal (Fig. 5). There was no evidence of splenic or intraperitoneal bleeding, abscesses, or injury to surrounding structures.

Necropsy. The omentum is seen adherent to site of splenic laceration without evidence of bleeding.
Discussion
The general acceptance of NOTES in humans will depend on the feasibility of managing intraoperative complications such as accidental injury to abdominal structures and bleeding. Splenic laceration and hemorrhage is an example of one such complication with potentially life-threatening consequences. Our data show that hemostasis could be achieved using a standard 7F bipolar probe after splenic laceration during NOTES. Survival animals had an uncomplicated postoperative course with no evidence of complications at necropsy.
Iatrogenic splenic hemorrhage occurs during surgery, but the exact incidence is not known. 1 Surgical literature focuses on the rates of splenectomy due to iatrogenic splenic injury. Injury to the spleen that does not result in splenectomy is rarely reported. Traction, capsular tears, and lacerations are generally the most common mechanism of injury. Procedures such as left hemicolectomy, left nephrectomy, and Nissen fundoplication are common operations in which the spleen can be injured. 1 Splenic injury most commonly occurs during left hemicolectomy with an incidence ranging from 2% to 8%. 10 Compared to its open surgical counterpart, laparoscopy appears to have a lower rate of complication and splenic injury.1,10 This is presumed to be as a result of better observation and less traction placed on the spleen.
Unfortunately, little data exist on the management of iatrogenic splenic lacerations. Most of the data on laparoscopic management of splenic bleeding is from the trauma literature, and in most cases these patients undergo splenectomy. 11 Laparoscopic splenic preservation after trauma using fibrin glue, microfiber hemostatic collagen, argon beam coagulation, and splenic mesh wrapping have been reported.2–5
Early data are beginning to emerge on hemostasis from vascular bleeding during NOTES. Fritscher-Ravens et al. recently reported management of bleeding from the gastroepiploic vessels during NOTES with three different endoscopic methods: suturing, monopolar forceps, and forced argon plasma coagulation. 8 Suturing failed almost immediately as blood obscured the field. Monopolar forceps could not stop bleeding in a total of 7 out of 12 pigs. Forced argon coagulation worked the best and bleeding was controlled in all 12 animals. Time to stop bleeding for the transgastric route was 4–72 seconds and 16–41 seconds for the transvaginal route. Thermal therapy for vascular bleeding during NOTES has also been reported in abstract form only by Park et al. 12 They compared a novel flexible endoscopic forceps to a standard laparoscopic cautery forceps. Both devices performed equally well in controlling bleeding from the uterine artery, ovarian pedicle, main (or branch) inferior mesenteric artery, or pairs of mesenteric bundles.
No published data currently exist for achieving hemostasis (with currently available endoscopic tools) after solid organ injury during NOTES. Giday et al. presented data on the use of nonthermal techniques for achieving hemostasis after liver laceration. 7 These investigators were able to achieve hemostasis using three novel agents (QuickClot, an amino silicate powder, oxidized regenerated cellulose gauze, and SHISH a new bioabsorbable agent).
Our data appear to be consistent with the current but sparse data regarding the feasibility of hemostasis for bleeding during NOTES. As opposed to other studies, we demonstrate successful hemostasis using standard endoscopic equipment. This may allow further NOTES procedures using currently available endoscopic accessories, thereby broadening its application. A few points from our study appear worth mentioning. (1) A higher energy setting of 30–40 W was needed as compared to standard settings for intraluminal gastrointestinal hemostasis. This is likely related to the high vascularity of the spleen with resultant brisk bleeding. (2) Time to hemostasis appears to be more in our study than in other reported methods. One possible reason for this is that the bipolar probe is not designed for achieving hemostasis from a larger surface area such as a splenic laceration. Also, frequently accumulated charred blood and tissue on the tip of the bipolar probe required this electrohemostasis catheter to removed from the endoscope for more frequent cleaning. Additionally, the surface of the bipolar probe was relatively small and required repeated and persistent application to cover the entire bleeding area. Diligent endoscopic inspection was performed with intermittent lavage to assess for persistent oozing or trickling of blood after electrocautery hemostasis. (3) The double-channel flexible endoscope was able to suction blood and clots from the peritoneal cavity during endoscopic therapy. This is important in managing intraperitoneal bleeding and also allowed adequate endoscopic observation. However, in the tamponade group a large clot formed in 1 case (since bleeding persisted and was not controlled). This large clot could not be suctioned through the endoscope. (4) Three cases were performed in a blinded fashion. One endoscopist performed the splenic laceration and then a second blinded endoscopist not present at the time of the laceration then attempted endoscopic therapy. In all cases the site of bleeding was identified by this blinded endoscopist and successful hemostasis was achieved with the bipolar cautery.
We acknowledge the limitations of this initial feasibility study. (1) Tamponade or packing is probably the first step in managing splenic bleeding as is done during standard surgery. Although packing may be standard practice at the time of surgery for controlling bleeding, it was very cumbersome using flexible endoscopes and accessories and the gauze often interfered with observation due to on-axis observation provided by the endoscope. Since the gauze used for packing did not fit through the channel of the endoscope, it could not be introduced into the peritoneal cavity like standard endoscopic accessories. Hence, an overtube had to be placed through the colotomy into the peritoneal cavity. The gauze was held with a forceps and Roth net and advanced into the peritoneum with the endoscope via this overtube, adding to the complexity of the procedure. This may explain why tamponade/packing may not be as easily employed during NOTES with flexible endoscopes and why it was not very effective in achieving hemostasis in our study. This may also be another reason to use standard endoscopic devices (e.g., bipolar cautery) for hemostasis during NOTES until better tools specifically designed for NOTES are available. (2) Small sample size and (3) lack of data on long-term effects and complications of splenic laceration and hemostasis. (4) This study treated a complication that was intentionally created by the investigators. There may be a bias that only those lacerations were caused that were in locations that could be easily accessed and treated. Successful hemostasis achieved by the blinded endoscopist, however, lends more credence to this method in our study. Also, needle-knife laceration may not be the perfect model to replicate splenic trauma and bleeding. However, the aim of the study was to test the ability to control splenic bleeding with available standard endoscopic devices and it appears that this study does demonstrate the feasibility of successful hemostasis with the 7 Fr bipolar probe. (5) More relevant complications may be those much harder to control via natural orifices such as delayed bleeding occurring during the postoperative period (hours or days after surgery). However, this study focused on intraoperative complications and its management using currently available standard endoscopic tools. Despite these limitations, this study shows that intraoperative bleeding during NOTES can be controlled using a standard endoscopic electrohemostatic catheter that is familiar to all gastrointestinal endoscopists.
In conclusion, our study demonstrates that standard flexible endoscopic bipolar cautery can achieve adequate hemostasis after bleeding from splenic laceration during NOTES. Further studies are needed comparing standard endoscopic bipolar cautery to laparoscopic hemostatic modalities. Newer devices and hemostatic compounds may aid in achieving quicker and more effective hemostasis, thereby allowing more NOTES procedures to be performed backed by the ability to manage bleeding complications.
Footnotes
Disclosure Statement
No competing financial interests exist.