
Abstract
Abstract
Background:
Though rare, bile duct injuries (BDI) during laparoscopic cholecystectomy (LC) represent a major potential complication with significant associated morbidity. The objectives of this study were to (1) assess the national use of LC and incidence of BDI over time in the pediatric surgical population, (2) measure the added resource utilization burden associated with BDI, and (3) identify patient and hospital factors associated with BDI.
Methods:
All patients 0 to 20 years of age undergoing cholecystectomy were identified in the Kids' Inpatients Database from 1997 to 2006. National rates of LC use and BDI as well as overall costs were assessed using weighted estimates. Factors associated with BDI were analyzed with a logistic regression model.
Results:
Of 31,653 patients undergoing cholecystectomy, 28,243 (89.2%) underwent LC. Over time, the proportion of LC has risen from 81% in 1997 to 91% in 2006 (P < .001). Of patients undergoing LC, 0.44% had BDI with no significant change of BDI rate over time. Length of stay was 6.1 days for patients with BDI compared to 3.3 days for those without injury (P < .001). BDI patients had median costs of US $9550 as compared to US $6030 for non-BDI patients (P < .001). After taking patient, hospital, and disease-specific factors into consideration, BDI was more common in patients 5 years of age or less, nonwhite patients, and in patients admitted under an elective setting (all P < .01).
Conclusions:
With increasing LC use, BDI remains a rare yet resource intense complication in children. Age, race, and admission related factors are associated with BDI and may provide guidance toward improving outcomes.
Introduction
Alhough rare, the true incidence of BDI during LC in children has not been well established. The objectives of this study were to (1) assess the national use of LC and incidence of BDI over time, (2) measure the added resource utilization burden associated with BDI, and (3) identify patient and hospital factors associated with BDI.
Methods
Data source
Data on patient encounters were analyzed from the Agency for Healthcare Research and Quality–sponsored Healthcare Cost and Utilization Project (HCUP) Kids' Inpatient Database (KID) from 1997, 2000, 2003, and 2006. 6 The KID is an administrative data set of patients, age 20 years or less, and contains data on over 10 million hospitalizations from 38 states. Versions of the KID are released in 3-year cycles and all available years were used in this study. Charges were converted to 2006 US dollars ($) based on U.S. Bureau of Labor Statistics Consumer Price Index adjustment. 7 The KID provides a hospital specific conversion factor for translating total charges into actual all-payer costs. 8 A linear predictive model was used to generate charge to cost ratio estimates for hospitals missing provided conversion factors. Furthermore, national estimates were generated using discharge- and hospital-level weights provided by the KID. 9 In brief, HCUP KID includes a sample of pediatric discharges from all State Inpatient Databases (SID) that have agreed to participate and share data. Pediatric discharges are sampled based on a stratification of uncomplicated in-hospital birth, complicated in-hospital birth, and all other pediatric cases. To further ensure accurate representation, discharges are sorted by state, hospital, and diagnosis-related groups. Systematic random sampling is used to select 10% of uncomplicated in-hospital births and 80% of complicated in-hospital births and other pediatric cases from each hospital. To obtain national estimates, discharge weights are developed using the American Hospital Association (AHA) universe as a standard. For the weights, hospitals are post-stratified on six characteristics contained in the AHA hospital files, including hospital ownership, bed size, teaching status, rural/urban location, and U.S. region, as well as freestanding children's hospitals status.
Patient selection
Patients undergoing cholecystectomy were identified in the KID using the International Classification of Diseases, Ninth Revision, Clinical Modifications (ICD-9-CM) primary procedure codes for open cholecystectomy (51.21 and 51.22) and LC (51.23 and 51.24). 10 To ensure that a standard cholecystectomy patient population was being identified, patients with diagnosis of chronic pancreatitis, pancreatic pseudocysts, liver or pancreatic transplantation, and malignant neoplasm of the pancreas, gallbladder, or extrahepatic bile ducts were excluded (n = 1505). Furthermore, patients were excluded if they had concurrent procedures performed such as liver biopsy or liver transplantation (n = 408). Patients with BDI were identified using a combination of diagnosis codes for BDI (868.02, 868.12, or 998.2) as well as procedure codes representing biliary reconstruction (51.36, 51.37, 51.39, 51.71, 51.72, and 51.79) during the concurrent hospitalization of a cholecystectomy procedure. 11 The study was performed under exempt status after review of study protocols by the Northwestern University Institutional Review Board.
Variables of interest
Various patient and hospital level variables were compared. Patient factors studied included age, sex, race (white versus other), admission status (emergent/urgent, elective, or other), primary diagnosis (cholecystitis versus other), number of diagnoses (1–2, 3–5, and ≥6), and insurance type (Medicare/Medicaid, private, and other). Hospital level factors studied included children's hospital designation (children's centers versus non-children's), and teaching status in combination with urban or rural hospital location. The KID assigns each hospital to one of four center types based on National Association of Children's Hospitals and Related Institutions designation: freestanding children's hospital, children's specialty hospital, children's units within general hospitals, or general/non-children's hospitals. 12 All children's hospitals were compared to general/non-children's hospitals. Geographic regions were also studied and assigned based on hospital state location according to U.S. Census Bureau definitions as provided by the KID. 13 Outcomes studied included length of stay, discharge destination, and costs.
Statistical analysis
National estimates were generated using analysis of complex samples. Preliminary inferential statistics were calculated for all variables using chi-squared tests for categorical data, Student's t-test to compare means, and Wilcoxon–Mann Whitney rank-sum test to compare medians. Logistic regression models were used to identify factors associated with BDI. Factors were made available for selection based on significance of P < .20 on univariate analyses. Subsequently, factors were selected in a forward stepwise fashion. Model quality was evaluated through assessment of the c-statistic and the Hosmer–Lemeshow goodness-of-fit statistic. For all analyses, statistical significance was set at a two-tailed P < .05. Statistical analyses were performed using SPSS, version 18 (SPSS Corporation, Chicago, IL).
Results
From the KID, we identified 31,653 patients undergoing cholecystectomy. Of these patients, 28,243 (89.2%) underwent LC. Of patients undergoing LC, and 125 (0.44%) had BDI. Table 1 provides the database rates of LC performance as well as national estimates derived from the KID. In the most recent year of this study, there were 17,322 cholecystectomy procedures performed in the United States, 15,806 LC (91.25%), and 69 BDI (0.44%). Over time, the proportion of LC has risen from 81% in 1997 to 91% in 2006 (P < .001). Over the same period the proportion of BDI has remained stable at ∼0.4% (P = .73, Fig. 1).
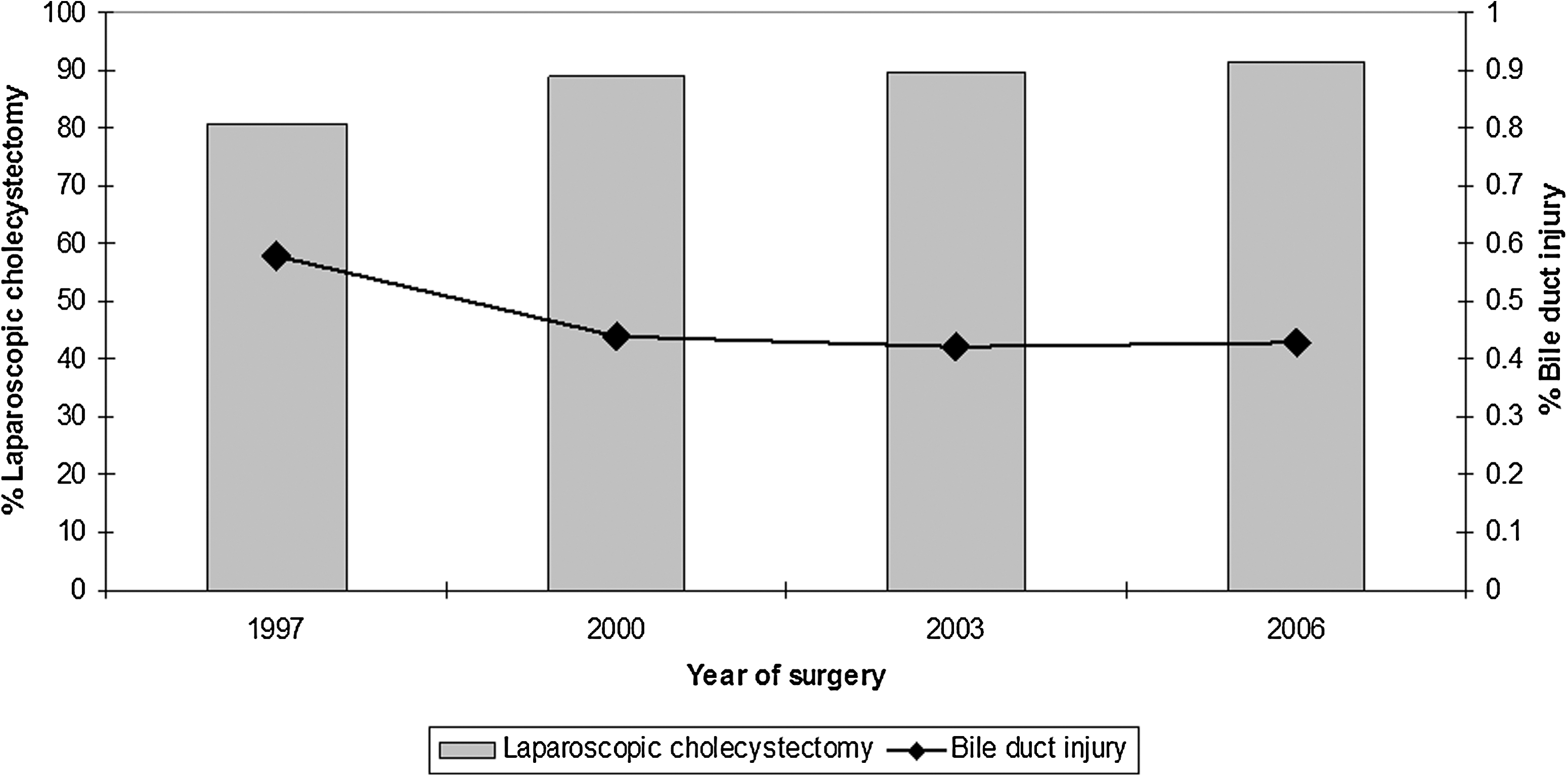
Proportion of laparoscopic cholecystectomy cases performed in the United States and bile duct injury rates by year of study.
Table 2 compares LC patients with BDI to those with no BDI. Mean and median age was similar between the groups with 98.6% of patients between the ages of 6 and 20 years. Among those 0–5 years old, BDI occurred in 4.51% of patients as compared to 0.41% for those 6 to 20 years old (P < .001). Proportionally, more male patients had BDI than female patients. Although a diagnosis of cholecystitis did not confer a higher rate of BDI, patients with BDI had a greater overall number of associated discharge diagnoses. Of note, biliary dyskinesia was the principle diagnosis for 1.7% of LC in 1997 and increased to 3.8% in 2006 (P < .001). Non-children's centers performed 81.7% of the LC and had a lower proportion of BDI than children's centers (P < .001). Children's centers had a higher proportion of patients ≤5 years of age (4.1% versus 0.3% at non-children's centers, P < .001) and patients with ≥3 diagnoses (41.2% versus 38.4% at non-children's centers, P < .001). Rural hospitals and hospitals located in the south had the lowest proportions of BDI. Length of stay was nearly half as long for patients with no BDI compared to those with BDI (3.3 days versus 6.1. days, P < .001). Overall, 98.7% of patients were discharged to home. Cost data were available for 27,256 patients (96.5%). BDI patients had median costs of US $9550 as compared to US $6030 for non-BDI patients (P < .001). In combination with the estimated frequency of LC in 2006, the national burden of LC was estimated at US $95,945,072.45. Estimated excess national costs of US $242,883.45 are a result of BDI at the time of LC hospitalization.
Missing data: location/teaching status (n = 214).
BDI, bile duct injury; SD, standard deviation; IQR, interquartile range.
Table 3 displays patient and hospital factors associated with BDI. After taking patient, hospital, regional, and disease-specific factors into consideration, BDI was more common in the youngest age group. Patients 16–20 years old were 89% less likely to have BDI compared to patients 0–5 years old (odds ratio [OR]: 0.11; 95% confidence interval [CI]: 0.06–0.21). Nonwhite patients were 49% more likely to have BDI compared to white patients (OR: 1.49; 95% CI: 1.01–2.21). Patients admitted under an elective setting were twice as likely to have BDI to those admitted under emergent/urgent status (OR: 2.00; 95% CI: 1.32–3.03).
Hosmer–Lemeshow test 0.445 and c statistic 0.624.
CI, confidence interval.
Discussion
Laparoscopic surgery has become a key aspect of the pediatric surgeon's technical armament. On the basis of 2008 survey of pediatric surgeons, LC represented the single highest rated minimally invasive surgery with 99% of respondents performing or recommending the procedure. 4 Our data support the trend of increasing LC use over time and closely resembles prior research using the National Inpatient Sample studying both adult and pediatric populations.11,14 Furthermore, indications for LC use are expanding. Our data support trends toward increasing use of LC to treat biliary dyskinesia.15,16 With the rising interest in single port LC in pediatric populations, 17 it is critical to continue to track complications such as BDI using large volume, multi-institutional data over time.
BDI rates are hard to assess even from large single-center reports.15,18 Our results are in line with rates published from large adult series and data sets.11,19–21 Dolan et al. assessed the National Inpatient Sample and used a strict BDI definition of LC followed by a procedure code representing biliary reconstruction in the same hospitalization and quoted an overall rate of 0.15% in adult patients. 11 Dolan et al. may have an underestimate of BDI as many patients with BDI are referred to specialized centers for management and may be excluded from their analysis which required the LC and the biliary reconstruction to be performed at the same institution.11,22 Flum et al. reviewed over 1.5 million records of adult Medicare beneficiaries undergoing LC and identified a 0.5% BDI rate. 20 Our study used broad criteria to define BDI including diagnosis codes indicating injury or the presence of a reconstruction code in the same hospitalization and identified a BDI rate of 0.44%. The use of administrative data in this fashion has been shown to possibly inflate the rate of complication detection. 23 Nevertheless, the benefit of using large administrative datasets such as the KID is that rare complications such as BDI can be studied on a national scale.
On the basis of national volumes as well as costs per patient, we estimate that the cost of LC in the United States approaches $1 billion per year. When appraising the hospitalization associated with LC and BDI alone, the national costs of BDI appear smaller than expected at approximately US $250,000 or US $3500 per case. These estimates appear to be a dramatic underestimate of the true costs of BDI. The limitations of the KID must be noted as many patients with BDI will be transferred for management and reconstruction at specialized centers and not captured in our analysis. Although our study provides an estimation of national costs associated with LC in children, there are many additional indirect costs of BDI that must be considered including further patient management, imaging, and follow-up clinic visits not accounted for in our study. Ultimately, the KID does not appear to be the optimal data source to study the costs and resource utilization aspect of BDI in children.
We identified younger, nonwhite patients admitted under an elective setting as having a higher likelihood of BDI during LC. To our knowledge, this study represents one of the first assessments of LC outcomes for patients <5 years old. Although BDI is rare, our results suggest extra attention toward avoiding BDI is warranted when performing LC in the youngest patients. The role of standard intraoperative cholangiogram during LC in children is debated and not uniformly practiced.24,25 Our study may motivate increased intraoperative cholangiogram use in youngest patient population. We were unable to identify if intraoperative cholangiogram was performed within our dataset. Race was also shown to be associated with outcomes. Dolan et al. identified race as an important factor in the adult population studied from the National Inpatient Sample with African Americans having seven times the likelihood of death after BDI compared to white patients. 11 Interestingly, our study demonstrated that patients undergoing elective LC were more likely to have BDI. These findings are supported in adult literature. Gurusamy et al. performed a meta-analysis of randomized controlled trials in adult patients underong LC and found a BDI rate of 0.5% in the early/emergent LC group and 1.4% in the delayed/elective LC group. 26 We hypothesize that this may be partially explained by increased surgeon vigilance and awareness in the more emergent/urgent setting. This observation could also be due to underlying patient pathology such as more chronic cholecystitis or cholelithiasis being scheduled as a elective case but representing a more technically demanding procedure with scar tissue and altered anatomy. This level of risk assessment is difficult to determine using administrative data.
As noted, there are several key limitations to using administrative data. Coding errors can lead to over- or under-estimates of rare events such as BDI. 23 Several data points studied had missing values, and statistical approximations were employed to account for some missing data. Additionally, there are several clinically relevant items such as conversion from LC to open procedures, cholangiogram use, and long-term outcomes that could not be reliably assessed. Key diagnostic subtleties such as the indication for surgical intervention may also be miscoded. For example, a case in which there was evidence of inflammation on final pathologic evaluation of the gall bladder may have been coded as acute cholecystitis where as the clinician's indication for surgical intervention may have been biliary dyskinesia. This type of error may explain our data demonstrating that biliary dyskinesia accounts for roughly 4% of LC, whereas recently published single-center reports note higher rates.15,27 Surgeon experience and specialty training were not available in the data set and may be a factor in BDI. Another key limitation to our data is that BDI that are diagnosed after discharge perhaps with readmission would not be captured allowing for an underestimate of the BDI rate. The most critical limitation relates to the cost and resource utilization data as described above. As noted, the KID does not capture subsequent hospitalizations or follow-up information, and therefore figures provided are a gross underestimate of the impact of BDI. Despite these limits, the KID provides a large sample of children undergoing LC and therefore allows for measurement and evaluation of rare but important events such as BDI.
In conclusion, over the last decade the proportion of LC being performed in children in the United States had increased to over 90% of all cholecystectomies. BDI occurs in 0.44% of LC cases in children and is associated with a doubling in length of stay and at least a 50% increase in costs. Factors associated with BDI included younger age at the time of LC, nonwhite race, and elective cases. On the basis of these findings, there appears to be specific populations and settings where added awareness of BDI risk may assist in improving surgical outcomes.
Footnotes
Acknowledgments
M.V.R. participates in the American College of Surgeons Clinical Scholars in Residence Program. M.V.R. is supported by the John Gray Research Fellowship and Aida and Daniel L. Rice.
Disclosure Statement
No competing financial interests exist.