
Abstract
Abstract
Background and Aim:
Single-system ectopic ureter with dysplastic kidney is a rare urologic anomaly. We report our early experience in 4 children who underwent laparoendoscopic single-site (LESS) nephrectomy for single-system ectopic ureters with dysplastic kidney.
Patients and Methods:
We diagnosed 4 consecutive children (aged 18–59 months; mean: 3.2 years) with single-system ectopic ureter with dysplastic kidney. A single, experienced surgeon performed LESS nephrectomy using a homemade single-port device in all patients.
Results:
LESS nephrectomy was completed successfully in all 4 patients without complications, insertion of an additional port, or open conversion. Blood loss was minimal. Mean operation time was 83.3 minutes (range: 55–125 minutes), and patients began oral intake on the first postoperative day. Mean postoperative hospital stay was 1.3 days (range: 1–2 days). Urine dribbling and wetting resolved immediately after surgery, and no patient has developed a urinary tract infection to date.
Conclusions:
LESS nephrectomy for an ectopic ureter with dysplastic kidney is a safe and feasible method with better cosmesis, compared with classic nephrectomy. LESS nephrectomy is a promising method in pediatrics.
Introduction
In recent years, laparoscopic nephrectomy has emerged as another surgical option.3,4 The procedure is performed with multiple small-diameter laparoscopic access ports, which minimize the need for the long incisions of open surgery and their associated morbidity. The popularization of laparoscopy has led to the development of new techniques, multichannel single-access ports, and articulating instruments that allow the procedure to be performed through a single skin incision, often one hidden in the umbilicus. Laparoendoscopic single-site (LESS) surgery has been performed to treat diverse urological diseases, and initial studies have demonstrated both feasibility and safety in adults.5–9 However, there are few reports on pediatric LESS nephrectomy for single-system ectopic ureter with dysplastic kidney.10,11 In this report, we describe our early experience in LESS nephrectomy for single-system ectopic ureter with dysplastic kidney in 4 children.
Patients and Methods
We diagnosed 4 consecutive children (aged 18–59 months; mean: 3.2 years) with single-system ectopic ureter with dysplastic kidney at our institution from February 2010 to June 2010 (Table 1). A single surgeon with experience in ∼60 cases of LESS surgery, Dr. D.H. Han, performed LESS nephrectomies on all 4 patients.
VUR, vesicoureteral reflux.
Two patients (cases 1 and 3) presented with continuous urinary incontinence despite normal toilet training. One patient (case 2) was diagnosed during work-up for recurrent urinary tract infections, and one patient (case 4) was diagnosed during evaluation for prenatal hydronephroureterosis.
All patients underwent ultrasound, voiding cystourethrogram and magnetic resonance urogram (MRU) as diagnostic imaging studies. In all patients, ultrasound showed multicystic or hypoplastic kidneys. In the 1 boy (case 2), voiding cystourethrogram demonstrated an ectopic ureter inserted into the urethra and causing vesicoureteral reflux (Fig. 1A). There was no vesicoureteral reflux in the 3 girls. All patients had a definite dysplastic kidney on MRU located normally in the renal fossa except for case 1, in which the dysplastic kidney was located on the right at the level of aortic bifurcation. All patients had possible ectopic ureter insertion on MRU (Fig. 1B, C). We performed dimercaptosuccinic acid renal scintigraphy to evaluate the functioning of the affected kidney and found it to be poor or nonfunctional in all patients.

Before surgery, all patients underwent cystourethroscopy or vaginoscopy examinations under anesthesia. The ectopic ureteral orifice was identified in the vaginas of the 3 girls and in the prostatic urethra of the boy.
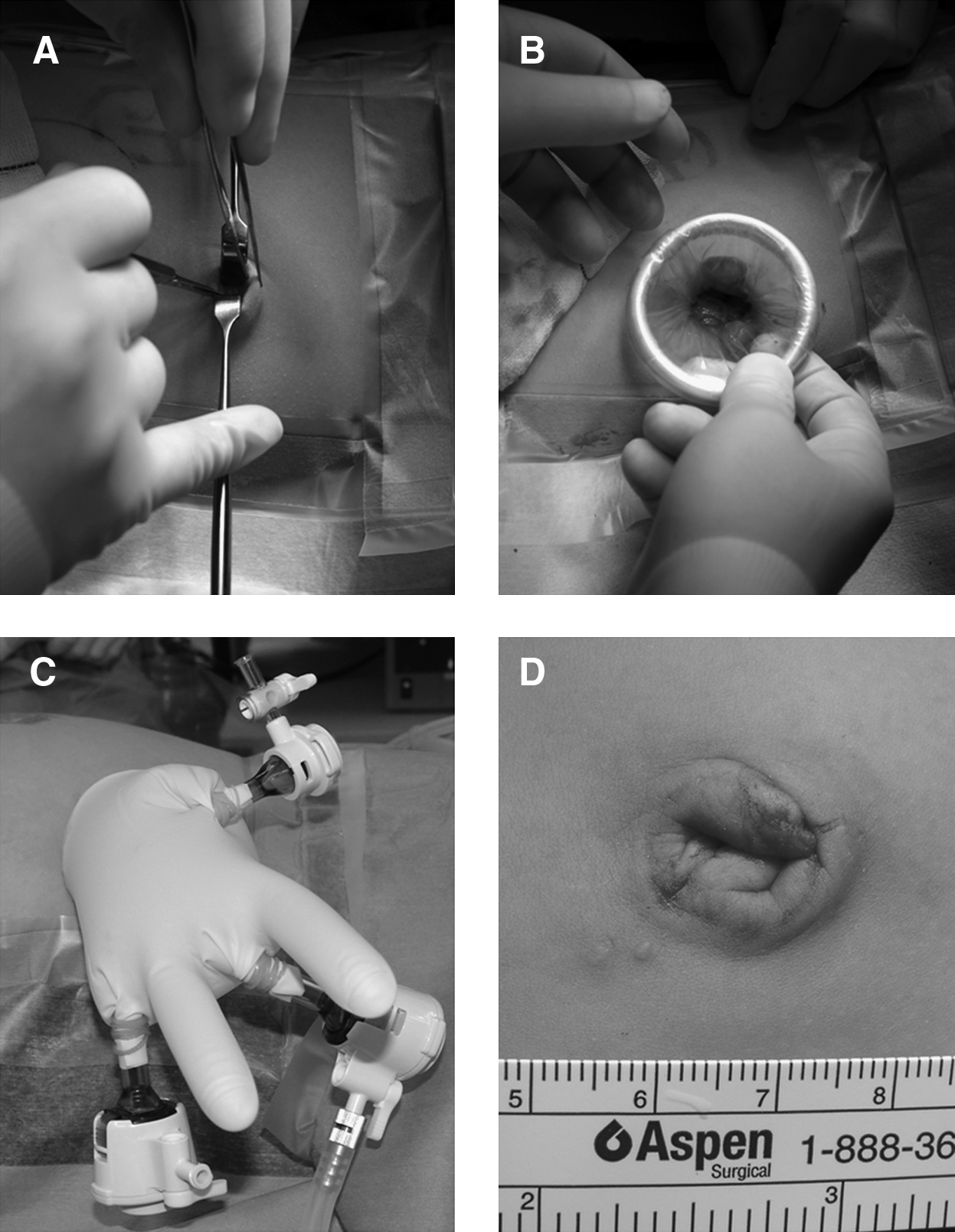
For the surgical procedure, the patient was placed in the semilateral decubitus position, and a 1.5-cm midline longitudinal incision was made at the umbilicus (Fig. 2A). We used a wound retractor (Alexis®; Applied Medical) (Fig. 2B) and a surgical glove as the homemade single port device. 12 To construct a single port similar to a commercial multichannel trocar, the inner ring of the wound retractor was inserted at the umbilicus and the outer ring was attached to a size 6½ surgical glove. We firmly fastened the first, third, and fifth glove fingertips to the ends of the three trocars (all 5-mm trocars) with a tie or rubber band (Fig. 2C). Pneumoperitoneum was achieved by CO2 gas insufflation to 12 mm Hg, and a 5-mm rigid laparoscope angled at 30 degrees was inserted. Using 5-mm articulating instruments (Autonomy™ Laparo-Angle™; Cambridge Endo) to overcome the lack of triangulation that occurs with a single port, nephrectomy was performed via the transperitoneal approach (Fig. 3). Dissection of the distal ureter was performed as caudal as possible, and the specimen was removed without morcellation through the umbilical incision site.
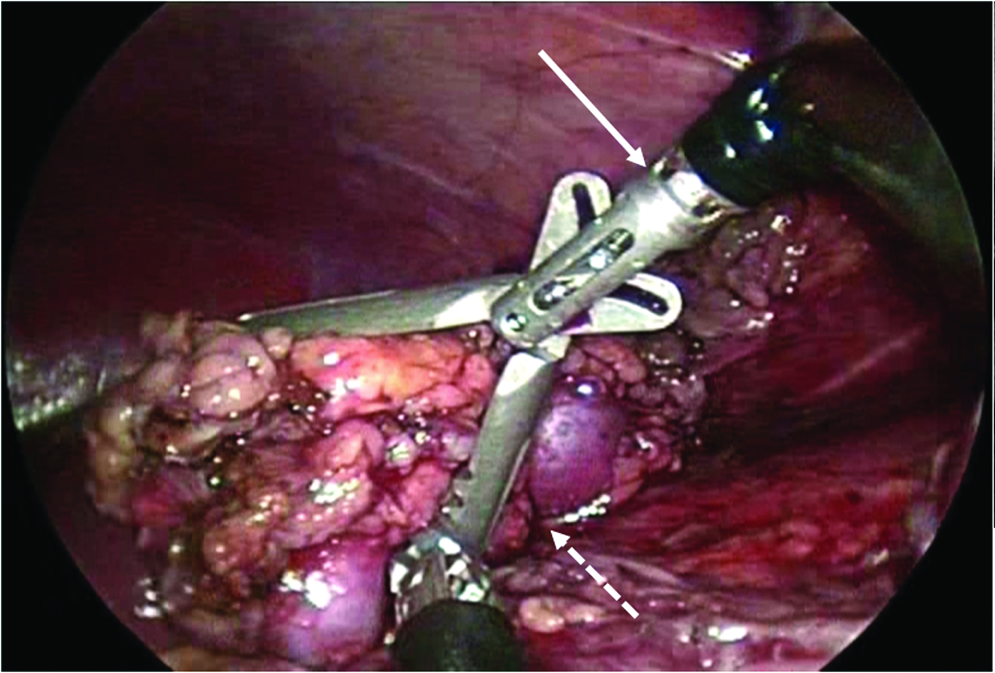
Intraoperative view. Dysplastic kidney (dotted arrow) was dissected using an articulating laparoscopic instrument (solid arrow).
Results
LESS nephrectomy was successfully completed in all 4 patients without conversion to open surgery. All procedures were performed exclusively through a single port. Mean operation time was 83.3 minutes (range: 55–125 minutes); the megaureter dissection in case 4 was difficult and led to a longer operative time of 125 minutes. Blood loss was minimal, and no transfusions or drainage tubes were required. There were no intraoperative or postoperative complications, and the resulting incisional wounds were small (Fig. 2D). Pethidine was administrated as analgesia in 3 patients during the postoperative fasting period; 1 patient (case 2) received 3 injections per day for 2 days, and 1 patient (case 4) did not require any analgesia. Oral intake was begun on the same day of surgery in all patients. Three patients were discharged on the first postoperative day, and 1 patient (case 2) was discharged on the second postoperative day because of wound pain. Urine dribbling and wetting disappeared immediately after surgery, and no patient developed a urinary tract infection during follow-up (median: 4 months; range: 2–6 months).
Discussion
Laparoscopic surgery can reliably confirm exact urologic diagnoses, locate the dysplastic kidney and ectopic ureter, and can safely and effectively accomplish their simultaneous removal. 13 On review of the literature, Jeong et al. reported the outcomes of laparoscopic nephrectomies for single-system ectopic ureters draining dysplastic, poorly functioning kidneys in 16 girls. 3 The mean operative time in their report was 109 minutes (range: 40–155 minutes), with little intraoperative bleeding. The mean postoperative hospital stay was 2.6 days (range: 2–4 days). A single intraoperative complication occurred in which trocar insertion injured the small bowel of 1 patient. Although the report by Jeong et al. is not similar to ours, we consider LESS nephrectomy for single-system ectopic ureters as a comparable treatment with minimal risk of trocar-related complications and better cosmesis compared with those of conventional surgery.
In our opinion, laparoscopic renal surgery has technical advantages in pediatric patients compared with those of adults for several reasons. In children, the kidney is small, perirenal fat is minimal, the tissue is soft and fresh, adhesions are absent, and the ureter is more easily identified. Nevertheless, widespread adoption of laparoscopic surgery in pediatric urology may be limited by current equipment, which is not ideally adapted to the small working spaces present in the bodies of children. Especially in infants and toddlers, the distance between the instrumental ports is often insufficient to sustain proper working space and triangulation. Although the 2-, 2.5-, and 3-mm laparoscopic instruments are now made with shorter shaft lengths, specifically for pediatrics, these instruments have less tractive force and durability than do conventional instruments for adults. Fortunately, using our homemade single-port device as described above, instruments for adult can be freely used without additional ports in the pediatric population.
The LESS nephrectomy for single-system ectopic ureters with dysplastic kidneys is technically easier than LESS nephrectomy for other diseases such as renal tumor, refluxing kidney, and nonfunctioning kidney owing to ureteropelvic junction obstruction. The ectopic dysplastic kidney is usually smaller than normal kidney and does not adhere to surrounding tissue. An extension of the umbilical incision to remove the nephrectomy specimen is not necessary. In addition, the feeding vessels of a dysplastic kidney are generally hypoplastic, easing their division.
The first report on urologic LESS in a pediatric population was reported in 2008. 14 LESS varicocelectomy was performed on 3 adolescents with unilateral varicocele using a multichannel commercial port. Operative times were <60 minutes, and all patients were discharged that same day. To our knowledge, there are some reports of pediatric LESS nephrectomy in literature (Table 2).10,11,15–17 Among all of these reports, operative time ranged from 62 to 150 minutes (mean: 108 minutes), blood loss was minimal, and mean postoperative hospital stay was 1.5 days (range: 1–2 days). Of note, Park et al. reported using a homemade single-port device to perform the first LESS nephrectomy in a 3-year-old girl with a single-system ectopic ureter and continuous urinary incontinence. 10 Operative time was 85 minutes and blood loss was negligible. No intraoperative or postoperative complications were reported, and the patient was discharged on the second postoperative day.
Several multichannel commercial trocars have been designed specifically for LESS surgery, including the R-Port (Advanced Surgical Concepts), the Uni-X (Pnavel Systems), and the SILS port (Covidien). However, to date, none of the commercial trocars for LESS have been available in Korea. Thus, we used a homemade single-port device consisting of a wound retractor and a surgical glove. This homemade device has several merits in its application to pediatrics. First, it is able to accommodate different numbers and sizes of instruments. For comparison, the R-Port consists of one 12-mm and two 5-mm ports, and the Uni-X system consists of three 5-mm ports. Second, the range of motion was wide with the homemade device.
A single-system ectopic ureter draining a dysplastic kidney is difficult to diagnose with intravenous pyelography because only the functional kidney is visualized in most cases. If the clinical suspicion is high for a single-system ectopic ureter draining a dysplastic kidney, ultrasound is used initially to rule out a duplex system, to visualize the renal vasculature, and to localize the dysplastic kidney. It can also detect an associated hydroureter if the system is obstructed. However, ultrasound is highly observer dependent. Recently, MRU has been shown to be a better method to diagnose this condition. 18 In our study, MRU suggested ectopic ureter insertion in all cases.
Conclusions
In this report, we review our early experience with LESS nephrectomy in single-system ectopic ureter with dysplastic kidney in 4 children. Compared with open and classical laparoscopic nephrectomy, the benefits of LESS nephrectomy include improved cosmesis in addition to a reduction in iatrogenic visceral and vascular injuries from port placement. LESS nephrectomy is a promising method in children with urogenital anomalies. Further studies, including prospective comparisons between LESS nephrectomy and conventional laparoscopic nephrectomy, are needed to more clearly define its role.
Footnotes
Disclosure Statement
No competing financial interests exist.