
Abstract
Abstract
Background:
The aim of this study was to evaluate and compare the use of choledochoscopy, cholangiography, and laparoscopic ultrasound in ensuring bile duct clearance and the prevention of missed stones after laparoscopic exploration.
Methods:
Operative details of 439 consecutive patients who underwent laparoscopic bile duct exploration between April 1994 and February 2005 were collected prospectively. Thirty-six conversions, 8 failures, and 8 patients who had a biliary enteric drainage procedure were excluded. Follow-up was by postal questionnaire or via their GP if there was no response.
Results:
One-year follow-up was complete in 95%. Patients underwent 253 transductal, 94 transcystic, and 29 radiological explorations. Laparoscopic ultrasound prompted immediate re-exploration of the bile ducts in six patients for stones missed by choledochoscopy. About 3.4% of patients presented with a missed stone within 1 year of surgery. The negative predictive values of choledochoscopy alone, choledochoscopy followed by postexploratory cholangiography and choledochoscopy followed by postexploratory laparoscopic ultrasound have been found to be 94.6%, 97.9%, and 97.4%, respectively.
Conclusion:
Double checking duct clearance with laparoscopic ultrasound after choledochoscopy is worthwhile, whereas cholangiography is not.
Introduction
Intraoperative observation of the bile ducts has been possible since Mirizzi's first description of intraoperative cholangiography in the 1950s. 4 This was shortly followed by choledochoscopy, the use of which was found to be favorable over cholangiography alone in the detection of ductal stones at open operation. 5 The additional tool of laparoscopic ultrasound has been available more recently. Several studies have compared the use of laparoscopic ultrasound and intraoperative cholangiography in the detection of bile duct stones at laparoscopic cholecystectomy before exploration of the bile duct. Laparoscopic ultrasound has been found to be superior with a sensitivity of between 80% and 100% and a specificity of 98% and 100% compared with 64% and 80% and 97% and 100%, respectively, for intraoperative cholangiography6–12 with little additive benefit in performing both procedures. In the only blinded study 11 with both experienced operators and immediate surgical confirmation of duct stones, the sensitivity and specificities for laparoscopic ultrasound and cholangiography were 96% versus 86% and 100% versus 99%, respectively. The superior performance of laparoscopic ultrasound together with its speed and lack of radiation exposure to patients and staff has led some to abandon the use of operative cholangiography in the observation of the bile ducts at laparoscopic cholecystectomy.
Despite the reliability of operative cholangiography and laparoscopic ultrasound in the detection of bile duct stones, these tools are not able to accurately measure the number of stones present. 11 Therefore, attempting to measure the number of stones in the duct before exploration to make a comparison with the number retrieved is inadequate in the assessment of duct clearance. Hence, re-imaging of the ducts after exploration is essential to ensure that the duct is clear.
The published studies of cholangiography describe the detection of stones at laparoscopic cholecystectomy but do not report sufficient clinical follow-up to explore the frequency with which stones are missed. This prevents a true calculation of the negative predictive values of laparoscopic ultrasound and operative cholangiography in the clinical setting. Moreover, there are no published studies evaluating the use of these techniques in re-imaging of the ducts immediately after laparoscopic exploration to assure duct clearance. Hence the reason for this study.
Materials and Methods
Operative details of 439 laparoscopic bile duct explorations between April 1994 and February 2005 were collected prospectively. The operative techniques of laparoscopic bile duct exploration within this institution have been described elsewhere.13,14 Thirty-six cases of conversion to an open operation, 8 failures of surgical clearance, and 8 patients who required biliary enteric drainage procedures were excluded (not mutually exclusive). Therefore, 397 patients who underwent apparently successful laparoscopic clearance of the bile duct were included in the study. After exploration of the bile duct the following modalities were used alone or in combination to assure duct clearance: choledochoscopy (Sc), on table cholangiography (OTC), laparoscopic ultrasound (7.5 MHz Aloka linear ultrasound probe; Key Med, Southend, United Kingdom) with a collapsed duct immediately after exploration (LUSc) or with a full duct after duct closure (LUSf). The techniques were standardized. As a matter of protocol choledochoscopy involved two passes along the bile duct both proximally and distally, after presumed duct clearance, although proximal observation of the bile duct was not always possible after a transcystic exploration. Adequate operative cholangiograms were defined as those that opacified the whole biliary tree, and where laparoscopic ultrasound was performed, the bile ducts were observed from the hepatic confluence to the ampulla.
The differing methods used in ensuring duct clearance over the 11-year period reflect historical changes in practice over the course of the series rather than different clinical indications for the use of each modality (Fig. 1). It was standard practice in the majority of patients to employ two modes of imaging to ensure clearance: either choledochoscopy followed by cholangiography or choledochoscopy followed by laparoscopic ultrasound. From the beginning of the series choledochoscopy was ordinarily followed by cholangiography. In 1999/2000 a number of patients underwent choledochoscopy alone as a second cholangiogram to ensure that clearance was time consuming and, at the time, not shown to be of benefit. In September 2000, and the 128th patient, laparoscopic ultrasound was introduced and came to supercede cholangiography after its initial evaluation in the comparative study of imaging the bile duct before exploration referred to earlier. 11 Laparoscopic ultrasound assessment of the bile duct after transductal exploration was initially performed with a collapsed duct before closure of the choledochotomy, but this technique was further refined from April 2004 and the 370th patient when it was performed with a full duct after closure as this provided easier observation.
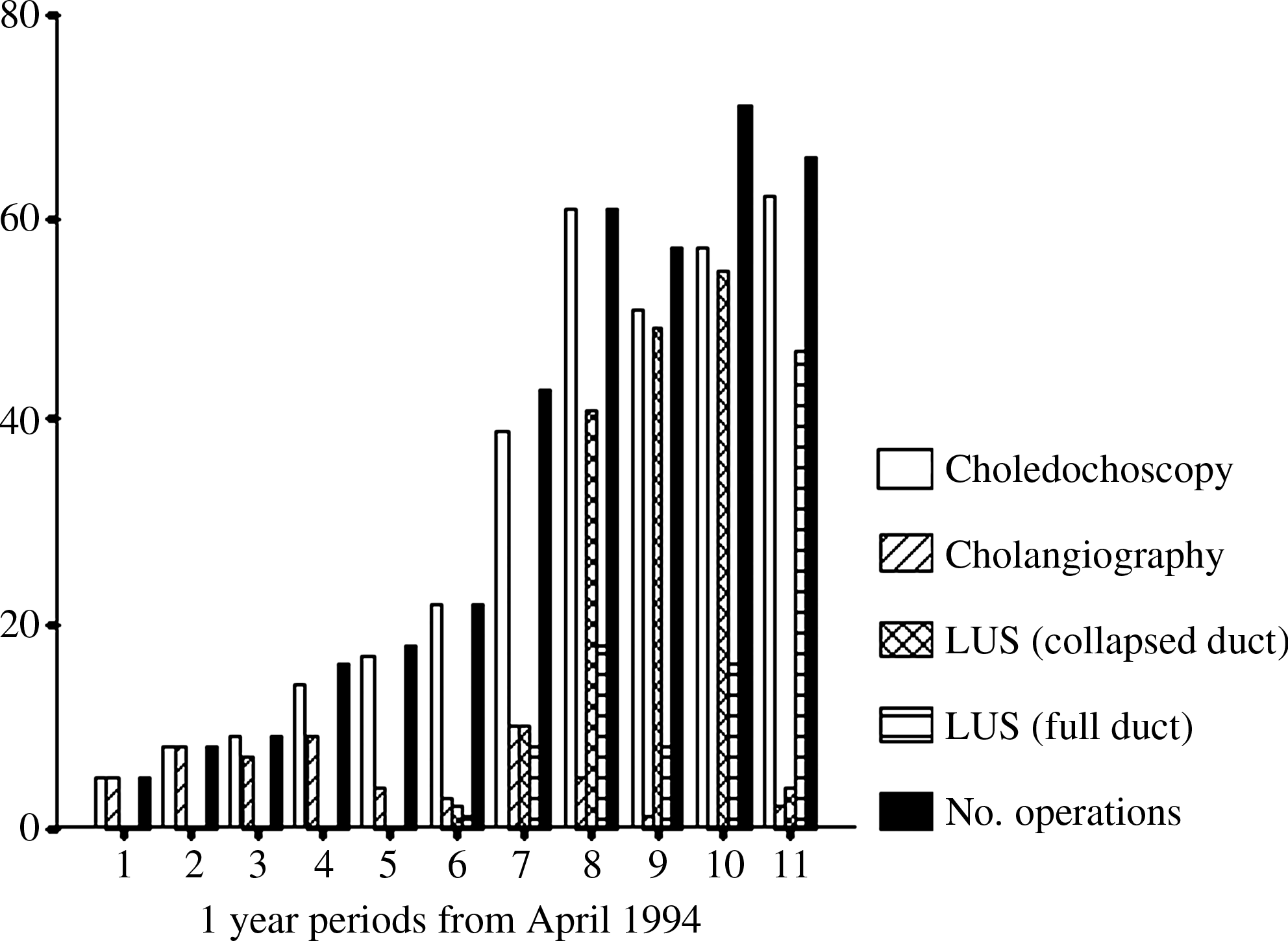
Distribution of methods employed in ensuring complete duct clearance in 397 patients.
The primary outcome measure was missed stones. A missed stone at operation was defined as one presenting within a year of surgery. This period was set, as in our experience this is a realistic time to allow missed stones to present but short of the time taken for primary bile duct stones to form. Patients were followed up by an independent assessor at least 1 year after surgery. Follow-up was by postal questionnaire, via patients' general practitioner if there was no response, or via the case notes if the patient had died. Chi-square test/Fisher's exact test was used for comparison of data
Results
One year follow-up was completed in 376/397 (94.7%) patients. There was 1 postoperative death, 12 patients died during the first year due to unrelated disease, and 8 patients were lost to follow-up. Twelve patients died after a year from surgery and were followed up by a review of their case records. The questionnaire was sent to surviving patients with a response rate of 90.3% (336/372). Twenty-eight nonresponders were subsequently followed up via their general practitioner.
Of the 376 patients who completed 1-year follow-up, 253 (67.3%) had undergone a transductal exploration and 94 (25.0%) a transcystic exploration. The remaining 29 patients underwent (7.7%) a radiological exploration. This technique involves flushing of the bile duct under contrast radiological or ultrasound observation. These latter cases are presented separately, as choledochoscopy is not employed with this technique.
At operation, laparoscopic ultrasound prompted immediate re-exploration of the bile duct after identification of stones missed by choledochoscopy on six occasions. Operative cholangiography did not identify any stones missed by choledochoscopy (P=.27).
Overall, 3.2% (11/347) of patients who underwent either a transcystic or transductal exploration re-presented within the first year with a missed stone at a mean of 3.8 months after surgery. The methods used in assuring duct clearance after these transcystic and transductal explorations and the number of missed stones that occurred with each method are shown in Table 1. The methods used in the diagnosis and treatment of these stones are shown in Table 2.
TC, transcystic; TD, transductal.
In patients who had choledochoscopy alone after transcystic or transductal exploration, 5.4% (4/74) presented with a missed stone. For clarity in presentation of the results and analysis, the two patients who had only postexploratory cholangiography are excluded. In the remaining patients, cholangiography and/or laparoscopic ultrasound were then used after clearance had initially been checked with choledochoscopy.
In patients who had postexploratory imaging after choledochoscopy with either cholangiography and/or laparoscopic ultrasound, 2.6% (7/271) presented with missed stones. Although this represents a reduction compared with choledochoscopy alone, the difference was not statistically significant (P=.22). There was no significant difference (P=.86) in the number of missed stones whether further imaging was carried out with either operative contrast cholangiography (1/47 [2.1%]) or laparoscopic ultrasound (6/235 [2.6%]).
Two of the 29 (6.9%) patients who had undergone a radiological exploration, which does not employ choledochoscopy, presented within 1 year with a missed stone. One of five patients who underwent radiological exploration with cholangiographic observation of the ducts and 1/24 performed with laparoscopic ultrasound had an endoscopic sphincterotomy at 6 and 2 weeks postoperatively, respectively, for a missed stone.
Discussion
This study aimed to evaluate the methods used in ensuring duct clearance after laparoscopic bile duct exploration. It has the benefit of relatively large numbers of patients with near-complete follow-up. It is a retrospective study, but throughout this period fixed protocols were used. Data were collected largely by postal questionnaire, which has the inherent limitations of accurate patient recall and responder bias. 15 The questionnaire was, however, very simple to compete and had been piloted in its development before distribution resulting in a very high response rate.
In this series, postexploratory laparoscopic ultrasound prompted immediate re-exploration for residual stones in the bile duct after choledochoscopic exploration in six patients, whereas cholangiography detected none. The rate of missed stones presenting within a year of surgery after transcystic and transductal exploration was halved, from 5.4% to 2.6%, when further imaging with laparoscopic ultrasound or cholangiography was used after choledochoscopy, although this was not statistically significant. There seemed to be no advantage gained between using either laparoscopic ultrasound or operative cholangiography in the rate of missed stones. A slightly higher rate of missed stones was observed after radiological exploration where choledochoscopy was not used. The small number of patients in this study who underwent radiological exploration (29 patients) precludes meaningful analysis, but the higher rate of 6.9% may be an indication that transcystic choledochoscopy might be worthwhile in these patients. It should be noted, however, that despite fastidious technique, it is very likely that other stones were missed by these modalities and were passed spontaneously without significant clinical consequence.
With the benefit of the adequate clinical follow-up presented in this study, the negative predictive values in ensuring duct clearance after retrieval of stones of choledochoscopy alone, choledochoscopy followed by postexploratory cholangiography, and choledochoscopy followed by postexploratory laparoscopic ultrasound have been found to be 94.6%, 97.9%, and 97.4%, respectively.
This study fails to show any statistical advantage for imaging the bile ducts once thorough choledochoscopy has demonstrated the ducts to be clear. However, laparoscopic ultrasound is easy, quick, safe, and inexpensive and resulted in the retrieval of stones that would otherwise have been missed. In the clinical context, this may prevent further complication such as pancreatitis and seems to be worthwhile. Postexploratory contrast cholangiography, on the other hand, appears to have little or no role.
Footnotes
Disclosure Statement
No competing financial interests exist.
Presented in abstract form at the Annual Meetings of The Association of Surgeons of Great Britain and Ireland, Edinburgh, May 3–5, 2006 and The Society of American Gastrointestinal and Endoscopic Surgeons, Dallas, April 26–29, 2006.