
Abstract
Abstract
Background:
The quest for scarless surgery continues, but the goal remains elusive. The logical top contender was natural orifice surgery, but unfortunately even today it remains in infancy. Minilaparoscopy also did not generate much interest. In this scenario, transumbilical single-incision laparoscopy surgery holds promise, especially as far as cosmetics is concerned, and may be the ultimate answer.
Methods:
All the 240 patients were operated by the same surgeon through a transversely placed umbilical incision in the upper half of the umbilicus. Three conventional ports, 10, 5, and 5 mm, were introduced through the same skin incision but separate transfacial punctures. The instruments included 10- and 5-mm 30° rigid telescopes and rigid instruments as in standard laparoscopic cholecystectomy (SLC). Patients with acute cholecystitis and calculous pancreatitis were included, but those with choledocholithiasis were excluded. Results were compared with those with SLC.
Results:
Patients were predominately female, with an average age of 37.6 years. Ten patients had difficult gallbladders, 24 had acute cholecystitis, and 10 had calculous pancreatitis. The mean operating time was 25.8 minutes, compared with 18.4 minutes in SLC. Intracorporeal knotting was required in 2 patients. Conversion to SLC was required in 5 patients. Morrisons pouch drain was left in 1 patient. Injectable analgesic was required in 138 (57.5%) patients and infection was seen in 2 (0.8%) patients.
Conclusions:
Transumbilical single-skin-incision laparoscopic cholecystectomy performed solely with conventional instruments is feasible, easy to learn, and probably the future of laparoscopic cholecystectomy.
Introduction
We present our initial experience with transumbilical SILC, also known as laparoendoscopic single-site surgery (LESS). Only conventional laparoscopic instruments were used. The procedures were all performed through a 2.0–2.5-cm transumbilical skin incision, with one 10-mm and two 5-mm conventional laparoscopic ports inserted through the same skin incision but separate transfacial punctures. We used 10- and 5-mm 30° rigid telescopes and conventional rigid laparoscopic instruments.
Materials and Methods
All patients presenting with gallbladder stone disease from October 2009 onward are now being offered SILC as the primary procedure in our unit. This includes patients with acute cholecystitis or mild acute calculous pancreatitis, but patients with choledocholithiasis are excluded. The present group of patients were investigated, and in those with CBD dilatation (>6 mm), a CT scan was carried out. An informed consent for the procedure was obtained. A 2.0–2.5-cm slightly curved transversely placed incision across the upper third of the umbilicus is deepened and upper flap is undermined for about 1 cm (Fig. 1). After creating a pneumoperitoneum of 8 mm Hg, a 10-mm trocar is introduced blindly through the umbilical incision in an upwardly oblique direction. The transfacial puncture of this port is cranial to the umbilical stalk. The skin incision accommodates all the three ports because it can be made to stretch transversely by about an extra 1.0–1.5 cm. The patient is then positioned in reverse Trendlenberg and left side 10° downward tilt as in three- or four-port standard laparoscopic cholecystectomy (SLC). A 30° 10-mm telescope is introduced through the 10-mm port, and after the initial visualization, two nonvalve, 5-mm tube trocars are inserted about 0.5–1 cm lateral to the 10-mm port on either side (Fig. 2). These ports are also introduced obliquely through separate transfacial punctures positioned cranial to the umbilical stalk. The right 5-mm port (on patient's right) is for the grasper and left 5-mm port is for the Maryland dissector. The dissection is started from the lateral peritoneal leaf of the gallbladder in the region of the Hartmann's pouch and cystic duct and then proceeded toward the fundus of the gallbladder. The dissection proceeds medially, gradually lifting the gallbladder from its bed. The medial peritoneal leaf is then dissected and the Calot's triangle is opened up. The cystic duct and the artery are skeletonized. The dissection continues until whole of the gallbladder, except for a minimal fundal attachment, is detached from the gallbladder bed (Fig. 3). The energy source used for the entire dissection is either the electrocautery or the harmonic scalpel. The 10-mm telescope is now withdrawn and a 30° 5-mm rigid telescope is introduced through the left 5-mm port. A 10-mm clip applicator is used to apply three clips on the cystic duct and one on cystic artery. The clip applicator is held by the surgeon in his left hand and the grip is kept laterally to the left. The cystic artery is alternatively dealt directly with the harmonic or the bipolar cautery without applying any clip. Transfixing intracorporeal knotting with 3-0 Vicryl may be required in patients with a very wide cystic duct. The needle is introduced percutaneously in the epigastrium and dragged in with the needle holder along with part of the suture. The tail of the suture remains attached to the abdominal wall and is cut after the first double loop has been formed on the Maryland in the left hand. After completion, the needle is extracted through the 10-mm port. Through the same 10-mm trocar, hook scissors are used to transect the cystic duct and cystic artery. The hook scissor then cuts the last attachment of the gallbladder fundus (Fig. 4). The gallbladder is then extracted with a 10-mm extractor. The transfacial holes at the umbilicus are closed carefully using 2-0 polygalactic acid (Vicryl; Ethicon Endosutures) or glycocholic acid (Dexon) suture on a 40-mm, 1/2 circle reverse-cutting needle and then the umbilical skin incision is closed (Fig. 5). Among all the suture needles, we found the 40-mm needle to be ideal, because thinner needles bend while applying the transfacial sutures. We do not perform intraoperative cholangiogram routinely, and in the present study, it was not required in any patient.

Transverse umbilical incision.

Position of the ports at the umbilicus. Also note the vertically directed light cord and CO2 insufflation tube.
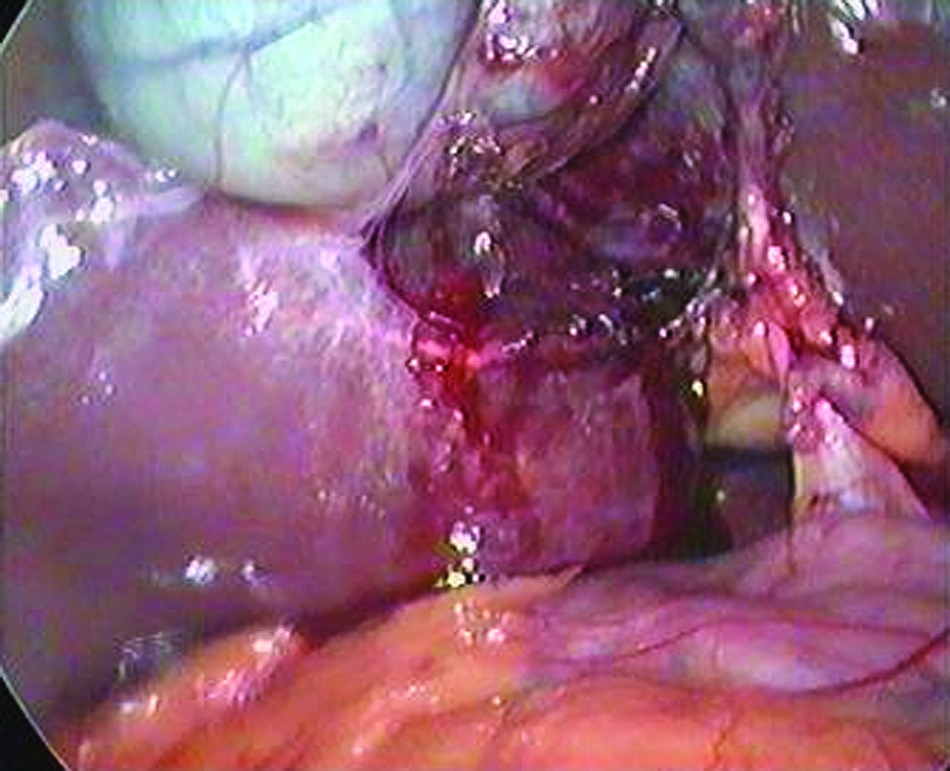
Gallbladder dissected from the liver bed, proceeding lateral to medial.
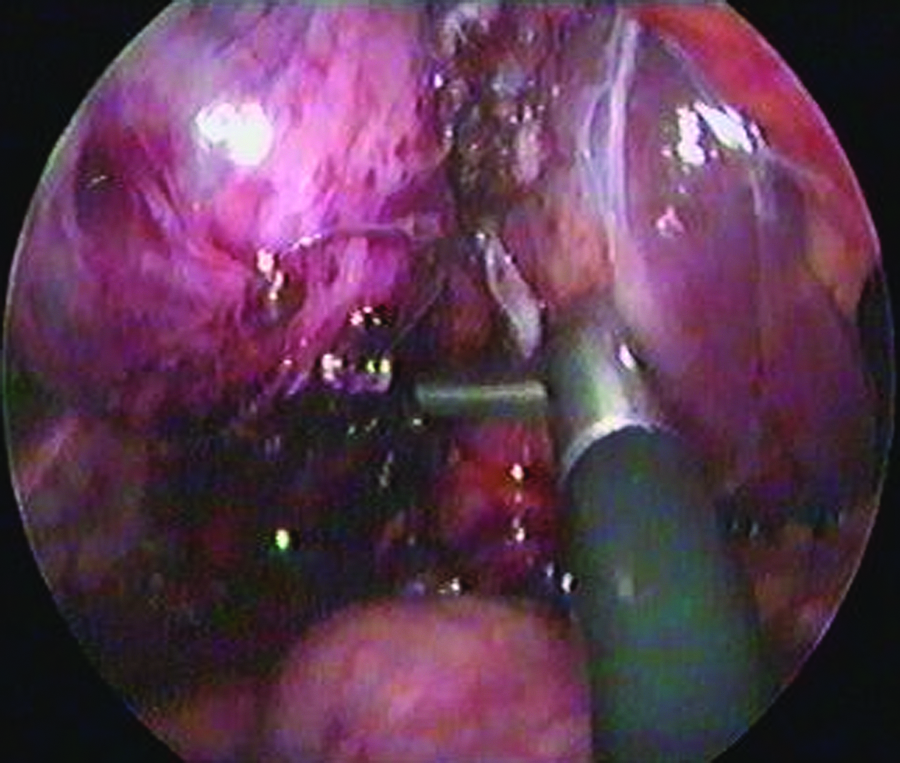
Partially transected cystic duct.

Stitched umbilicus.
The technical modifications required for SILC as opposed to the original SLC include the need to cross the instruments inside the abdomen while dissection is being performed and the need for the surgeon to use both his hands actively. The camera assistant holds the camera with his left hand and stands on the surgeon's right, instead of standing behind the surgeon as in SLC. This gives the surgeon more elbow space. It is also important to emphasize that the rigid laparoscopic instruments used should have the cautery knob at the distal end in line with the instrument and not on the top (Fig. 6). The second assistant is required to keep the light cable and carbon dioxide tube absolutely vertically positioned to minimize their clashing with the hand instruments (Fig. 1). The 5-mm ports are specially selected as simple tubes without valves so as to minimize the clashing of the ends of the ports outside the abdomen (Fig. 7).

The instrument on the top is not to be preferred. Note the obliquely situated cautery attachment point as opposed to in-line attachment in the lower instrument.

Tubular 5-mm ports (reusable).
Postoperative analgesics include injectable Tramadol 100 mg intramuscularly followed by oral diclofenac 50 mg on demand. Pain was assessed by the visual analog scale.
We compared the results with those of our series of SLC, which included 3492 patients. Statistical significance was calculated, but the wide disparity in number of patients among the two groups has to be kept in mind.
Results
Transumbilical SILC was attempted in 240 consecutive patients of calculus gallbladder disease. There were no exclusions except those with choledocholithiasis and those with gallbladder phlegmon presenting anytime after the end of the 2nd week after the attack. The patients were predominantly female and with an average age of 37.6 years (Table 1). The presentation included 24 patients with acute cholecystitis, of whom 14 had a phlegmon, 10 patients had mild acute calculus pancreatitis, and 10 patients were labeled as having difficult gallbladders (Table 2).
n=240 patients.
CC, chronic cholecystitis; AP, acute calculous pancreatitis.
The operating time was taken as the time from the skin incision to closure of the umbilical incision. The operating time varied from 28 to 66 minutes (average, 36.6 minutes) in the first 20 patients and from 16 to 55 minutes (average, 25.8 minutes) in the next 220 patients. The initial patients were those during our learning curve, when we were learning to cope with clashing trocars, instruments, tubes, and cords. Our comparable average operating time in three-port SLC was 18.4 minutes and the difference was significant (Table 3). Conversion was required in 5 patients. In 3 patients, it was converted to two-incision laparoscopic cholecystectomy. In these patients, the reason for conversion was inability to grasp a very thick, fibrotic gallbladder. In the other 2, because the xiphi-umblical length was greater than the instrument length, a three-port SLC was required (Table 3). A very short and wide cystic duct required closure with intracorporeal suturing with 3–0 Vicryl in 2 patients. The suturing was done without conversion. An FG 18 tube drain in the Morrison's pouch is optional.
“P” value was considered as significant when below 0.05.
SILC, single-incision laparoscopic cholecystectomy; SLC, standard laparoscopic cholecystectomy; NS, not significant.
Injectable analgesic was required in only 138 (57.5%) patients and oral analgesic was never required after 36 hours. Thirty-six patients did not require any analgesic. Significantly more patients (2465 or 70.59%) required injectable analgesics in the SLC group (Table 3). On the visual analog scale, compared with the SILC group, wherein 80.6% patients had a >75% recovery, 70.7% patients had comparable improvement in the LC group. Discharge time was between 24 and 36 hours (1.9 days) when compared with LC (2.3 days). Return to work was identical in both groups. There was port-site discharge in 12 patients, which was serosanguinous. Infection was seen in 2 (0.8%) patients. The infection rate in the corresponding three-port laparoscopic cholecystectomy was 0.40% (Table 3).
The subsequent appearance of the umbilicus was cosmetically very acceptable at 2 weeks, because the scar was totally hidden within the folds of the umbilicus (Fig. 8).

Umbilicus at 2 weeks.
Discussion
SILC or LESS cholecystectomy is an easily learnable and performable procedure that adheres to the principle of laparoscopic surgery albeit with a few modifications and acceptable compromises. The history of single-incision laparoscopic surgery also seems to be a repetition of laparoscopic surgery because once again, as had happened with laparoscopic surgery, gynecological lap surgeons were first off the block and single-incision interventions were being done as early as 1969.1,2 The first general surgical laparoscopic operation through single incision but with an operating laparoscope was an appendectomy.3–5
The first true single-hole surgical procedure was an appendectomy performed in 2005 at the Department of pediatrics in Izmir Turkey. The first SILC was performed by Navarra et al. using two 10-mm trocars 6 and later by others,7–10 who used two 5-mm trocars. In all the studies, the gallbladder was retracted with percutaneous transabdominal sutures or wire. Since then the repertoire of the single-incision laparoscopic surgeon also seems to be increasing by leaps and bounds and during the last 2–3 years the horizon has gradually expanded to include almost all advanced laparoscopic surgeries including urological applications,11–14 gynecological interventions,1,2,15,16 colorectal surgery,17–19 and bariatric surgery,20,21 to name a few.
The majority of literature on LESS procedures reports the use of ports, such as triport, airseal port, and X-cone with three or four holes,22–26 and curved instruments. But these ports are disposable and costly and this is a limiting factor in their adaptation for regular usage. Then there have been some innovations such as using the surgical glove to form a leak proof umbilical port.26,27 But it is heartening to see a few reports wherein SILC (LESS cholecystectomy) has been performed similar to the present study, with conventional ports and instruments.23,28,29
Keeping the 5-mm ports as simple tubes and all ports in the same line and 0.5–1.0 cm apart reduces the clashing of the extra-abdominal parts of the ports. Romanelli et al. also used a similar arrangement of ports but only in their initial 4 patients. 3 Chow et al. 5 and Petrotos 9 also used routine laparoscopic ports, but they have not mentioned the exact position of the port insertion site. In our opinion and practice, a 10-mm and two 5-mm ports in the same transverse line can easily be accommodated in the 2.0–2.5-cm umbilical incision because the skin can be made to stretch in either direction. This is important, because if the punctures are too close, then there is a chance of the holes joining each other and it becomes very difficult to maintain an adequate pneumoperitoneum because of the leaking gas.
Our surgery includes rigid 30° telescopes of both 10 and 5 mm diameters. The view of instruments through these closely positioned ports showed the instruments and telescope in a parallel line. This essential in-line viewing, with this arrangement of port, does have its limitations, but the 30° telescope when rotated sideways can give some degree of lateral view especially required during clip application. Flexible endoscopes and even long bronchoscopes have been mentioned and advocated in many reports.30–32
The majority of reported series on SILC are with Roticulator (Covidien) instruments or flexible or bent instruments and their recommendation is for the advantages of using these instruments.26,29,30,33,34 Routine rigid instruments have been used less frequently,35–37 and even in these studies, there was an early switch to Roticulator or curved instruments. 30 In fact, Rivas et al. 2 have suggested that if more than two rigid instruments are required through the umbilicus, then there would be clashing of instruments, making the procedure more time consuming and difficult, and so they shifted to one rigid and one Roticulator instrument. We do not agree with this, and with our arrangement of ports and dissection using both the hands, using the rigid instruments is easily learned after 15–20 surgeries. It is also important to remember that to reduce the clashing of the external parts of the instruments, the cautery point attachment should be in line with the body of the grasper and not as an oblique attachment.
Another area where we do not agree with the prevailing practice is the use of stay sutures for gallbladder manipulation.23,24,28 These, according to us, are problematic because they result in bile leakage of varying degrees, making the operation a contaminated one rather than a clean contaminated one. But there are studies in which, like us, there is no puppet-like suspension of the gallbladder.26,27,29 Also, the multiple transfacial transgressions by the transfacial sutures in the right hypochondrium are a reason for postoperative pain. In this context, it should be pointed out that those who have been doing and have mastered the art of three-hole LC do not require stay sutures for gallbladder manipulation. Contrary to the belief, the critical view of Calot's triangle was never a problem with this method of SILC because angulations of the gallbladder were easily achievable with the grasper in the surgeon's left hand.
The problem of clashing of instruments and the telescope can thus be minimized in the following manner:
1. Keeping the 5-mm ports as simple tubes with washers prevents clashing of ports.
2. Keeping the transfascial entry points of all the three ports 0.5–1 cm apart, in the same transverse line.
3. Using instruments of different lengths.
4. Cautery point at the distal of the instrument (in line) rather than have it jutting out cranially.
5. Light and CO2 cord to be kept vertically upward (Fig. 1).
6. Keep the intra-abdominal projecting part of the cannula minimally inside the abdomen to prevent crowding and their clashing inside.
There was no selection criteria for our patients, and all patients with gallbladder stone disease were taken up for SILC, including those with empyema and acute cholecystitis. In fact, since the mid-2009, every patient presenting with gallbladder disease in our unit has been offered SILC as the primary procedure. All the studies to date, to the best of our knowledge, have an exclusion criteria, with only patients with gallbladder colics, chronic cholecystitis, or biliary sludge being taken up for SILC. 30 Our results prove that SILC can be taken up as a routine procedure for all patients with gallbladder stones. We could successfully manage acute cholecystis, phlegmon, gallbladder abscess, and difficult gallbladders (Table 2) with SILC. In fact, the conversions that we had were in chronic cholecystitis patients. The operating time logically improved with 36.6 minutes in the first 20 points versus 25.8 minutes in the next 220 patients. This was statistically significant. A similar improvement of operating time was also mentioned by Rivas. 2 Our operating time for SILC was, however, significantly longer than the three-port technique. In addition to the cosmetic appeal, a more obvious advantage of SILC appears to be the significantly lesser incidence of pain when compared with SLC (Table 3).
A concern has been raised about the possible weakening of the facial layer in and around the umbilicus because of the multiple punctures and traction thereof. 4 But till date at 6 months there has been no umbilical hernias in our group of patients. Without the long-term results of SILC, the possible complication of umbilical hernia and its incidence cannot be commented upon. The port-site infection appears to be higher at 0.8% as opposed to 0.4% in the SLC group, but this is of no statistical significance.
The final operative site scar at the umbilicus is cosmetically very acceptable, because after a month of surgery the scar is hardly seen as has also been mentioned by others.27,30 So is this an answer to scarless surgery? However, infraumbilical incision, which been reported in many studies,23,31,33 or the vertical incision,27,30 although being functionally adequate, will not give a cosmetic result as good as the transumbilical transverse incision.
After having performed SILC on a sizeable number of patients, it can be pointed out that highly advanced procedures such as TEP for inguinal hernia and operations on the colon, kidney, spleen, and other solid organs may not be possible without the special ports and Roticulator instruments. But a sizeable number of laparoscopic surgeries can be completed with SIL surgery, using routine instruments. To date we have completed a good number of TAPP for inguinal hernia, appendectomies, ruptured ectopic, tubo-ovarian masses, and myomectomies and intracorporeal suturing with SIL surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.