
Abstract
Abstract
Background:
Although laparoscopic cholecystectomy (LC) is a common and widely applied technique, the use of antibiotics during the perioperative period in infection prevention remains controversial. In our study, a meta-analysis was performed to assess the impact of antibiotic prophylaxis on the postoperative infection rate in LC.
Methods:
A literature search was conducted on studies published between January 1966 and March 2010 that involved LC and prophylactic administration of antibiotics. Only randomized trials that compared perioperative antibiotic prophylaxis with placebo or no treatment in low-risk patients undergoing LC were selected. Eighteen studies qualified according to the inclusion criteria, but only 12 were of adequate quality according to the Jadad scale to be included for the meta-analysis. Data were analyzed via the Peto odds ratio (OR) method and run using RevMan 4.2 software. The precision of the estimation of OR by individual studies was used to calculate their contribution (or weighting) to the pooled OR.
Results:
The results of the 12 studies did not have significant heterogeneity, and thus, the fixed effect model was used for data analysis. Compared with placebo or no treatment, there was no significant risk reduction in the antibiotic prophylaxis group with regard to overall infections (OR=1.11; 95% confidence interval [CI], 0.68–1.82; P=.67), wound infections (OR=1.07; 95% CI, 0.59–1.94; P=.99), major infections (OR=2.88; 95% CI, 0.3–28.09; P=.36), distant infections (OR=1.01; 95% CI, 0.43–2.36; P=.99), or positive bile cultures (OR=0.76; 95% CI, 0.54–1.08; P=.12). However, prophylactic antibiotics did shorten length of hospital stay (weighted mean difference=−0.16; 95% CI, −0.22 to −0.09; P<.01).
Conclusion:
Prophylactic antibiotics are not necessary for elective LC in low-risk patients.
Introduction
Materials and Methods
A literature search was conducted on MEDLINE, EMBASE, Cochran Central Register of Controlled Trials, Pubmed, and WANFANG DATA between 1966 and March 2010 using the following keywords: “laparoscopic cholecystectomy,” “antibiotic,” and “prophylactic.” Papers and abstracts that evaluated the use of antibiotics in the prevention of infection in LC were gathered irrespective of language, publication status, or results. The references of these articles were also searched for potential papers.
Inclusion criteria
This meta-analysis only incorporated randomized trials that compared use of prophylactic antibiotics in LC versus placebo or “no treatment” in low-risk patients. In these RCTs, “low-risk patients” were defined as not having any evidence of acute cholecystitis or obstructive jaundice, were not on long-term corticosteroid or other immunosuppressive agents, and had no known infections. All patients must have been given antibiotics within 30 minutes prior to the operation and/or up to 3 days postoperation. All studies must have analyzed the impact of prophylactic antibiotics on at least one of the following parameters: overall infection, superficial wound infections, intra-abdominal infections, distant infections, positive bile cultures, and length of hospital stay.
Data collection
Details of the study design, the number of subjects and dropouts, as well as the type, dose, and schedule of antibiotic administration were noted. Infection outcomes according to the inclusion criteria were recorded. All studies were assigned a quality score according to the Jadad scale 2 (Table 1), where a score of ≥3 represented a high-quality study. Data collection was independently performed by three authors and reviewed by a fourth. Differences were discussed by all four and resolved by consensus.
Data analysis
The effects of prophylactic antibiotics on LC were analyzed by calculating the pooled estimates of overall, superficial, intra-abdominal, and distant infections. Separate analyses were performed for each outcome using the Peto odds ratio (POR) method and weighted mean difference (WMD). Both fixed and random effects models were used. A statistically significant result was indicated by a P value of <0.05 or 95% confidence interval (CI). RevMan 4.2 and Stata 10.0 software were utilized for statistical analysis of the data. Publication biases were assessed by funnel plot. Heterogeneity among studies was assessed by calculating I2 measure of inconsistency.
Funding
This meta-analysis was not supported by any pharmaceutical company, government agency, or grant.
Results
The initial search identified 156 articles using the key words “laparoscopic cholecystectomy,” “antibiotic,” and “prophylactic.” One hundred thirty-eight of these studies, some of which were case reports, case series, reviews, or retrospective studies, were excluded for not meeting the inclusion criteria. The remaining 20 RCTs were reviewed by three independent authors.3–21 Of the 20 RCTs, only 12 studies were of adequate quality (i.e., Jadad scores of 3 or more) to be included in the meta-analysis. The detail and Jadad scores of these RCTs are listed in Table 2. The included RCTs were all published between 1999 and 2009. Four of these RCTs were performed in the United States, five trials in Asia, and three trials in Europe. All trials were single-center studies. No significant heterogeneity was present among the studies for any of the nominated outcomes.
RCT, randomized, controlled trial.
Different antibiotics were evaluated in the selected trials. Five RCTs used cefazolin, two used cefuroxime, three used cefotetan, and three used levofloxacin, ceftriaxone, and cefotaxime, respectively. Antibiotics were administered preoperatively in all studies. Three RCTs continued antibiotics at 24 hours after the operation. No significant publication bias was identified when evaluated by funnel plot (Fig. 1) and Egger's test (t=0.20; P=.844 >0.05; bias 95% CI, −1.38032–1.64805).
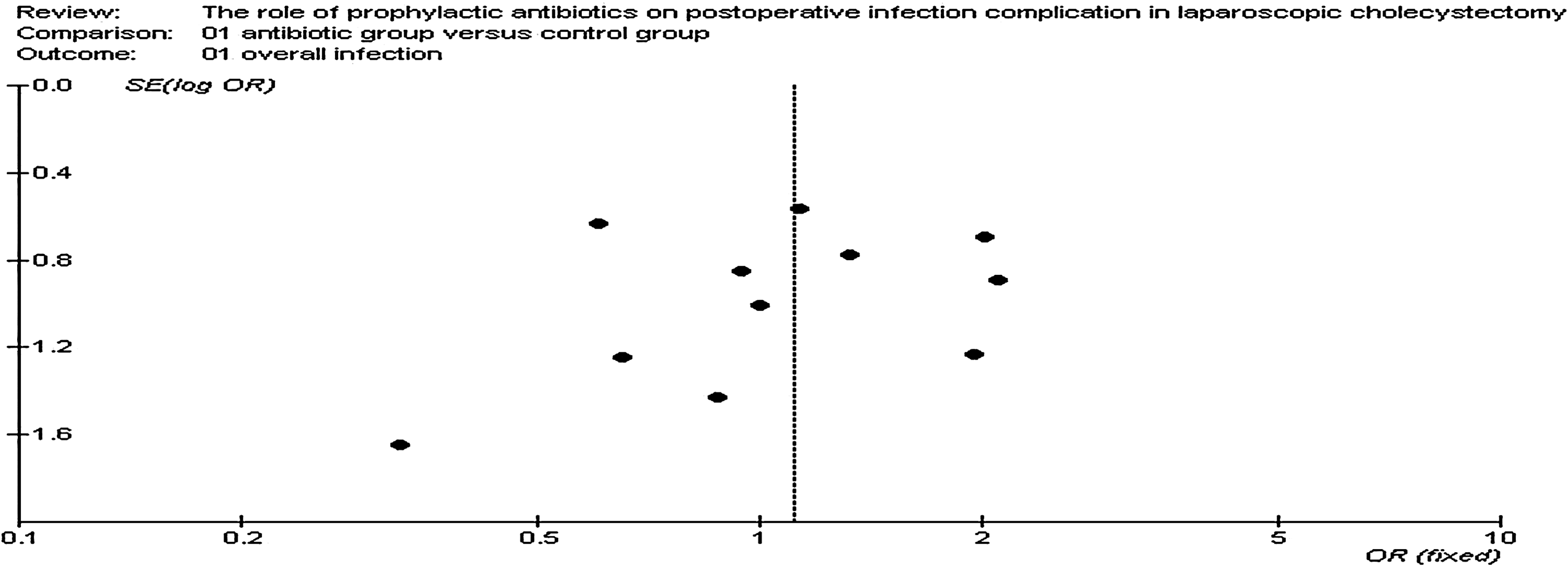
Funnel plot for overall infection from all included studies suggesting no publication bias by showing multiple studies on both sides of the dotted line in an approximately equal distribution.
Overall infection complication
The overall infection complication was evaluated by all 12 trials. One study by Dobay et al. demonstrated no infection. In the remaining 11 trials, 36 of 991 patients (3.6%) treated with prophylactic antibiotics prior to LC developed an infection, as did 32 of 946 patients (3.4%) who did not receive prophylactic antibiotics. Pooled analysis did not reveal a statistically significant odds reduction in overall infection complications using prophylactic antibiotics prior to LC (OR=1.11; 95% CI, 0.68–1.82; P=.67) (Fig. 2). There was no significant heterogeneity among the studies (I2=0%; P=.98). Further analyses were performed for subtypes of infection.

Forest plot demonstrating overall infection from studies with prophylactic antibiotics compared with no antibiotics or placebo for laparoscopic cholecystectomy.
Superficial wound infections
All 12 trials evaluated the complication of superficial wound infections. The study by Dobay et al. demonstrated no infections. Superficial wound infections were documented in 23 of 991 patients (2.3%) treated with prophylactic antibiotics prior to LC and in 21 of 946 patients (2.2%) who did not receive prophylactic antibiotics. Pooled analysis did not reveal a statistically significant odds reduction superficial wound infection complications using prophylactic antibiotics prior to LC (OR=1.07; 95% CI, 0.59–1.94; P=.99). There was no significant heterogeneity among the studies (I2=0%; P=.83).
Major infections
Only six trials evaluated major infection complications. Major infections, in the form of intra-abdominal collections or abscesses, were documented in 2 of 554 patients (0.36%) treated with prophylactic antibiotics prior to LC. Major infections were not documented in any patient who did not receive prophylactic antibiotics. Pooled analysis did not reveal a statistically significant odds reduction in major infection complications using prophylactic antibiotics prior to LC (OR=2.88; 95% CI, 0.3–28.09; P=.36). There was no significant heterogeneity among the studies (I2=0%; P=.98).
Distant infections
Nine trials evaluated distant infection complications. Distant infections were defined as any infection separate from the wound site and include urinary track or respiratory tract infections. Distant infections were documented in 11 of 786 patients (1.4%) treated with prophylactic antibiotics prior to LC and in 11 of 736 patients (1.5%) who did not receive prophylactic antibiotics. Pooled analysis did not reveal a statistically significant odds reduction in distant infection complications using prophylactic antibiotics prior to LC (OR=1.01; 95% CI, 0.43–2.36; P=.99). There was no significant heterogeneity among the studies (I2=0%; P=.68).
Bile bacteria cultures
Seven trials evaluated positive bile bacteria cultures. Positive cultures were documented in 75 of 486 patients (15.4%) treated with prophylactic antibiotics prior to LC and in 94 of 488 patients (19.3%) who did not receive prophylactic antibiotics. Pooled analysis did not reveal a statistically significant odds reduction in positive bile cultures using prophylactic antibiotics prior to LC (OR=0.76; 95% CI, 0.54–1.08; P=.12) (Fig. 3). There was no significant heterogeneity among the studies (I2=0%; P=.84).
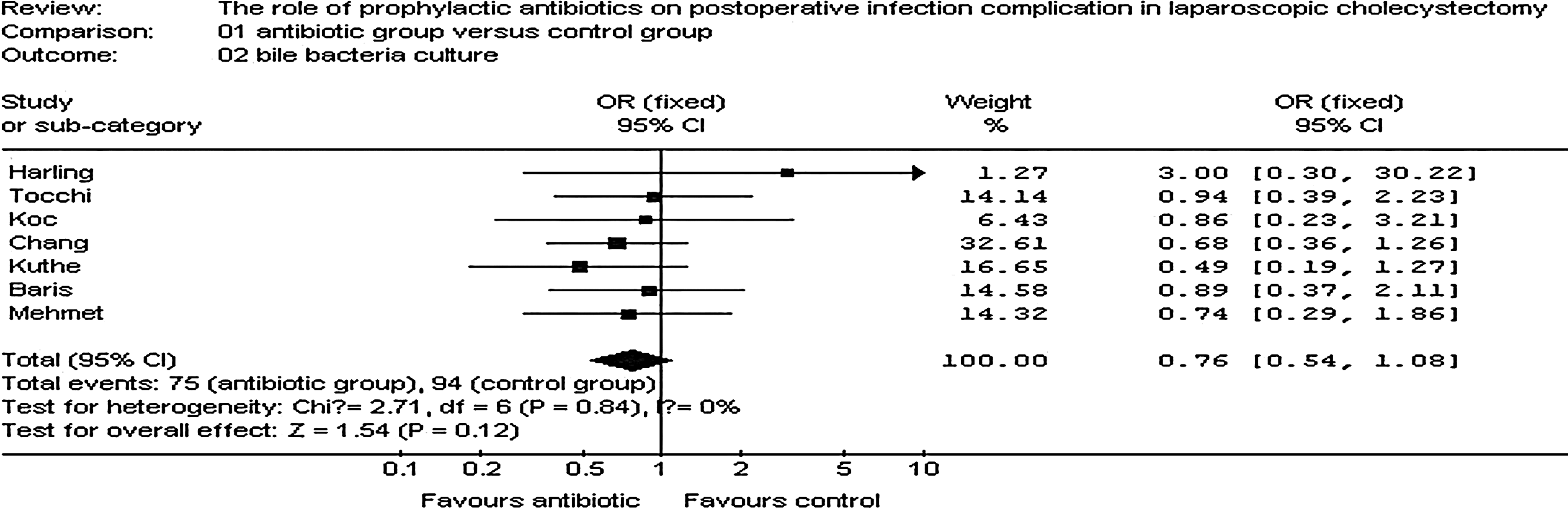
Forest plot demonstrating bile bacteria culture from studies with prophylactic antibiotics compared with no antibiotics or placebo for laparoscopic cholecystectomy.
Hospital stay
Only three trials evaluated length of hospital stay and found that prophylactic antibiotics prior to LC lead to shorter hospital stays (WMD=−0.16; 95% CI, −0.22 to −0.09; P<.01). There was no significant heterogeneity among these studies (I2=78.8%; P<.01).
Discussion
Antibiotics do play an important role in the reduction of postoperative infection complications, especially in large complex operations such as open abdominal surgery. However, it appears that too many surgeons have applied this general rule to even minor operations in the hopes of preventing postoperative infections. 22 Zhu et al. investigated the antibiotic use in 579 patients who had undergone LC 23 and found astonishingly that 85.4% of patients received preoperative antibiotics and 70.5% received postoperative antibiotics.
LC has become the preferred method to treat symptomatic cholelithiasis and gallbladder polyps. It has many advantages over OC, such as small-size incision sites, mild postoperative pain, faster recovery of gastrointestinal function, shorter hospital stay, and lower rate of infections. 24 The rate of postoperative infections has been found to be 0.4%–1.7%, much lower than that of OC.25–27 Lippert's study found that prophylactic antibiotics were necessary during perioperative period. 28 However, many other researchers have found the opposite to be true. 29 Therefore, the use of prophylactic antibiotics in LC remains controversial.
Our meta-analysis demonstrates that there is no statistical significance between the two groups (antibiotics versus no antibiotics) in overall infection, superficial wound infection, major infection, distant infection, and positive bile cultures. The RCTs selected for our study included the latest national and international research papers to obviate language bias. All selected trials scored equal to or more than 3 on the Jadad scale, to increase the reliability of the result. In addition, our study found similar results to that of Choudhary et al. and Zeng et al. 30
Finally, we found that prophylactic antibiotic can shorten the length of hospital stay. The reason behind this result is probably related to the infection of surgical incision. Prophylactic antibiotic is the periprocedural systemic administration of an antimicrobial agent intended to reduce the risk of local and systemic postprocedural infections. The potential benefit of prophylactic antibiotic is determined by patient-related factors (ability of the host to respond to bacterial invasion), procedural factors (likelihood of bacterial invasion at the operative site), and the potential morbidity of infection. Prophylactic antibiotic is recommended only when the potential benefit outweighs the risks and anticipated costs (including expense of agent and administration, risk of allergic reactions or other adverse effects, and induction of bacterial resistance). The prophylactic agent should be effective against organisms characteristic of the operative site. Cost, safety, and convenience of the agent should also be considered. The duration of antimicrobial prophylaxis should extend throughout the period when bacterial invasion is facilitated and/or likely to establish an infection. 31 There have been many reports and comprehensive reviews on the prevention of surgical site infection and the use of prophylactic antibiotic in general surgery. 32 But in LC, of which infection risk is much lower than OC, using prophylactic antibiotics is no more significant.
The strengths of this meta-analysis include using RCTs, different population groups, and similar outcomes in all studies despite different antibiotics being used. Also, no publication bias or significant heterogeneity was noted for any of the major outcomes. It is a limitation of this meta-analysis that only low-risk patients were evaluated for the use of prophylactic antibiotics. There is still uncertainty for prophylactic antibiotic use in high-risk patients undergoing LC. High-risk patients have been defined by some investigators as age >60 or the presence of diabetes mellitus, acute colic within 30 days before LC, jaundice, acute cholecystitis, or cholangitis. Interestingly, Tocchi et al. and Koc et al. found that the presence of high-risk factors were independent of the development of infective complications. However, Kuthe et al. and Chang et al. showed the opposite to be true. Despite the controversy, none of the RCTs provided separate data about the effect of prophylactic antibiotics in LC in this particular subgroup of high-risk patients for comparison. Therefore, another meta-analysis would be needed to be conducted for high-risk patients.
It can be inferred from the results of this study that to reduce the infection complication rate in LC, surgeons must meticulously adhere to the operative aseptic technique, aim for shorter operation times, and improve operative technique. For example, careful use of diathermy to reduce risk of gallbladder wall rupture, and if rupture does occur, thorough abdominal cavity wash out is required. To expedite recovery, surgeons should encourage early mobilization and ensure good nutrition. Easing tissue tension is another method to reduce the incidence of infection. In conclusion, this meta-analysis has found no benefit for using prophylactic antibiotics in low-risk patients undergoing LC. At present, most research trials have only focused on the low-risk patients. Ideally, to complete the evaluation of prophylactic antibiotic use in LC, multicenter RCTs involving large sample sizes of different population subgroups, especially high-risk patients, are needed.
Footnotes
Disclosure Statement
No competing financial interests exist.