
Abstract
Abstract
Background:
Obesity is a serious health problem that leads to serious physical and psychological problems. The methods used in treating obesity include diet and behavioral changes, pharmacotherapy, and surgery. Laparoscopic adjustable gastric banding (LAGB) and intragastric balloon (IGB) applications are two of the methods used to treat obesity. The aim of this study was to compare the effects of LAGB with those of two consecutive IGB applications in weight loss management of obese patients.
Methods:
Thirty-two patients (F/M:24/8) admitted in the study were divided into two groups. In the first group of 16 patients, LAGB was performed, and in the other group two consecutive IGBs were applied. Total weight loss, body mass index (BMI), excess weight loss percent (EWL %), and excess body mass index loss percent (EBMIL %) were recorded at months 6, 12, and 18 for both groups.
Results:
At the end of the 6th month, BMI values of LAGB and IGB groups were 36.0 and 30.6 kg/m2, EWL % were 32.3% and 39.3%, and EBMIL % were 36.3% and 47.1%, respectively. The results were similar. At the end of 12 months, median BMI was 36.6 kg/m2 for LAGB and 27.5 kg/m2 for IGB (P<.05). The EWL % and EBMIL % at the end of the 12th month were 57% and 70%, which is significant in favor of IGB. The last evaluation was made at the 18th month of applications, and the three parameters for two applications were found to be similar.
Conclusions:
The achieved weight losses at the 6th month were similar for both groups. However, at the 12th month, two consecutive IGB applications were more effective. At the end of the 18th month, the results were again similar. Two consecutive IGB applications may be offered to obese patients who do not feel ready for surgery.
Introduction
In this study, we aimed to compare the effects of LAGB with those of consecutive IGB applications in weight loss management of obese patients.
Materials and Methods
LAGB (LAP-BAND, Allergan) was applied to 16 patients (group I) and two consecutive IGBs (Bio-Enterics; Allergan) in another 16 (group II), respectively. Demographic characteristics of the patients, comorbidities, complications, and follow-up information in both groups were extracted from prospectively recorded registries (Table 1). Patient eligibility criteria of the American Society for Metabolic and Bariatric Surgery were used in patient selection for LAGB, that is, body mass index (BMI) ≥40 without comorbidities or BMI ≥35 with comorbidities. 6 LAGB was performed using standard pars flaccida technique. After 3 weeks of liquid and soft food intake, band filling began and solid food was introduced. IGB was applied under deep sedation anesthesia in the left lateral decubitus position after a standard upper GI endoscopy, as described by Coskun et al. 7 The exclusion criteria for balloon application were hiatal hernia >5 cm, active peptic ulcer, severe esophagitis, hemorrhagic risk, Crohn's disease, cancer, diverticule or esophageal stenosis, serious cardiopulmonary, renal or hepatic disease, previous gastric surgery, psychological disturbances, sweet eaters, and lack of motivation or reluctance to follow the treatment protocol.8,9 In eligible patients, the balloon was inserted into the stomach and filled with 600 mL saline mixed with 10 mL methylene blue dye under direct endoscopic vision. Patients were discharged after 6 hours under observation. The patients were given an activity-increasing program (150 minutes/week of moderately intense exercise) and a 1200 kcal/day balanced diet and followed up. After 6 months, the balloon was removed under sedation anesthesia and a new one was inserted in the same operation. Follow-up and treatments were repeated as in the first application. Weight losses, BMIs, percentage of excess weight losses (EWL %), and percentage of excess body mass index losses (EBMIL %) were recorded at the 6th month (removal of the first balloon), the 12th month (removal of the second balloon–termination of the IGB treatment), and the 18th month in both groups.
Median.
Range.
BMI, body mass index; LAGB, laparoscopic adjustable gastric banding; IGB, intragastric balloon.
Statistical works
Results are expressed as mean±standard deviation and range for numerical variables and absolute numbers. Statistical analyses were made using Student's t-test for numerical variables and chi-squared test or Fisher's exact test for categorical variables. Data were evaluated using the SPSS program (Statistical Program for Social Science, version 16.0). Values of P<.05 were considered significant.
Results
The number of patients and the female-to-male ratio in each group were identical (12/4). Median ages and preoperative weights were 36.5 versus 33.5 years and 112 versus 103 kg, respectively. The preoperative BMI values were 40.7 kg/m2 for LAGBs and 35.9 kg/m2 for IGBs (Table 1).
The comorbidities accompanying obesity and the improvement that are detected at the 18th month are summarized in Table 2.
At the end of the 6th month, for the LAGB and IGB groups, BMI values were 36.0 and 30.6 kg/m2, EWL % were 32.3% and 39.3%, and EBMIL % were 36.3% and 47.1%, respectively. The results were similar. At the end of the 12th month, median BMI was 36.6 kg/m2 for LAGB and 27.5 kg/m2 for IGB (P<.05). The EWL % and EBMIL % at the end of the 12th month were 57% and 70%, which are significantly in favor of IGB (P<.05). The last evaluation was made at the 18th month of the applications, and the three parameters were found similar (Table 3). Also, EWL % and EBMIL % values are represented in Figure 1.
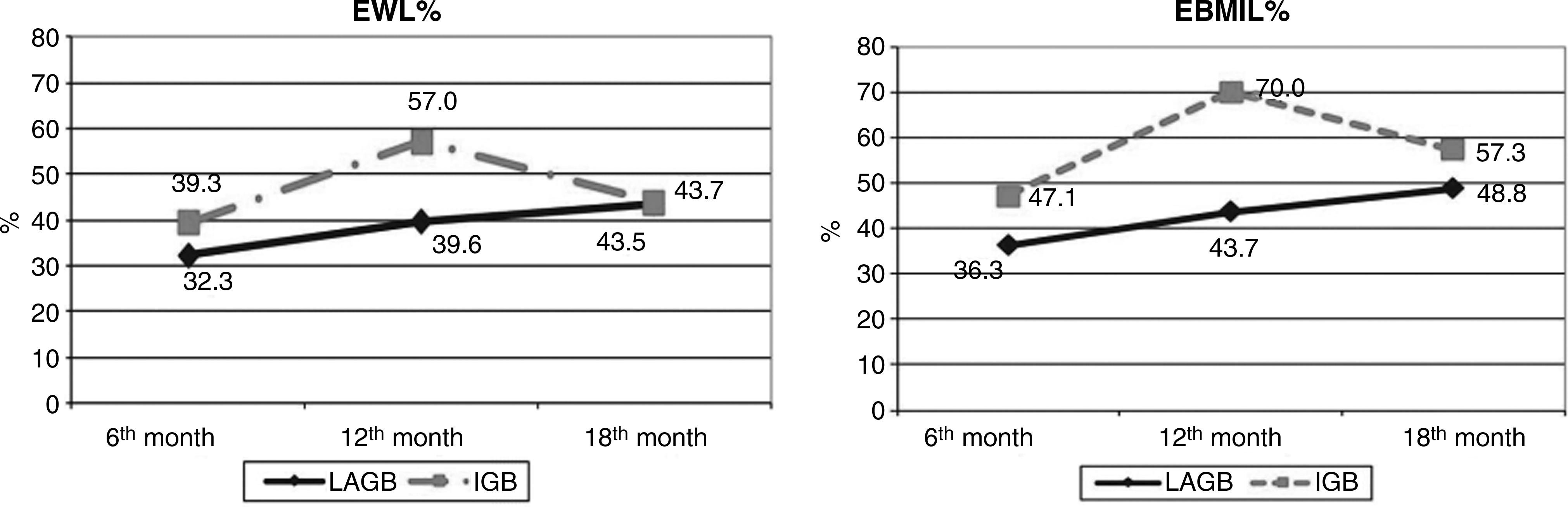
Excess weight loss percent (EWL %) and excess body mass index loss percent (EBMIL %) graphs.
Second IGB was removed.
EWL %, excess weight loss percent; EBMIL %, excess body mass index loss percent.
In 1 of our LAGB patients, port infection at the 2nd month and band migration at the 10th month were determined. The band was surgically removed at the 19th month due to progression in migration. In another patient, a port infection developed after a year. The infection was controlled by medical treatment but it recurred at the 23rd month and the band was surgically removed. The reoperations in these 2 patients were performed after the 18th month of the applications, so the patients were not excluded from the study. In the IGB group, no complications were detected. No mortality was seen in either group.
Discussion
LAGB is the most common bariatric surgical method applied, especially in Europe and Australia. The advantages of the method include reversibility and the fact that stomach resectioning and anastomosis are not required. It is quick and easy to apply, compared with other bariatric surgical methods. However, long-term complications related to the port and the band itself should be considered. 4 IGB is an endoscopic treatment method that is easy to apply and does not require general anesthesia. It also reduces the risks of surgery and anesthesia in planned bariatric operations along with reduction of weight-related comorbidities. The most important disadvantage of the method is the necessity of removal of the balloon at the end of the 6-month period.8,9 This disadvantage is addressed by consecutive applications.
When we evaluated the parameters showing weight losses achieved in LAGB and IGB patients in the study, weight loss at the end of the 6th, 12th, and 18th months, EWL %, and EBMIL % values were similar. BMI reductions at 0–6, 6–12, and 12–18-month intervals were similar in the first two periods, but they significantly increased in LAGB patients in the last period (P=.002). EWL % difference and EBMIL % difference were markedly higher in patients with IGB at the 6–12-month interval (P=.004 and P=.003, respectively). In other words, the values obtained with application of the second balloon were higher than those obtained with LAGB. Individuals began to regain the weight they lost with the removal of the balloon at the end of the 12th month. As weight loss continued in the LAGB patients, the EWL % difference and EBMIL % difference at the 12–18-month period were determined to be markedly higher (P=.001 and P=.001, respectively).
In a prospective study of LAGB-applied patients, EWL % at first 5 years were 58.8%±30.0%, 59.0%±34.1%, 56.8%±35.0%, 58.8%±38.8%, and 58.4%±46.6%, respectively. 10 In another study, the EWL % was 42.6% after a year. 11 In our study, the results were 32.5% at the 6th month, 39.6% at the 12th month, and 39.6% at the 18th month.
Lopez-Nava et al. reported that consecutive IGB applications are more effective than single-balloon application with the average EWL % of 31.5±23.2 and average EBMIL % of 59.9±24.4 at the end of the 12th month. 12 In our patients, EWL % was determined to be 40.6%±21.0% after application of the first balloon and 56.8%±20.3% after application of the second balloon.
In the study, although the EWL % and EBMIL % at the 6th month were more encouraging in the IGB patients compared with LAGB patients, it is not statistically significant. But at the 12-month period, when the IGB treatment is completed, the BMI, EWL %, and EBMIL % were significantly high in favor of the IGB group (P=.038, P=.023, and P=0.011, respectively). These results correlate to our hypothesis that consecutive IGB applications are more efficient for weight loss in comparison to the LAGB at the 12-month period. The three parameters at the end of the 18-month period were similar for LAGB and IGB; this can be explained by the continuous effect of LAGB on food intake restriction, which does not apply to patients whose IGBs were removed at the 12th month. The observations showed that weight maintenance beyond a year in IGB was obtained in 40% of the patients, so it is recommended that it be combined with other anti-obesity measures. 13 Because we were unable to find any paper comparing LAGB and consecutive IGB applications in the literature, we cannot compare our results with existing literature.
In the study by Milone et al., who compared laparoscopic sleeve gastrectomy (LSG) and IGB applications, EWL % and EBMIL % at the end of 6 months following applications were determined to be 35% and 24%, respectively. 14 However, this study includes only superobese patients prepared for definitive operation. In the study, LSG is declared to be effective in preparation of superobese patients for definitive surgery and it is also highlighted that IGB is a noninvasive outpatient procedure. When Genco et al. compared the 6th and 12th month EWL % and EBMIL % values of the patients with LSG and IGB (single application), they could not find any statistical difference. It was observed that IGB is a better alternative for preparation of the patients to bariatric surgery, compared with LSG (in a 12-month period). 2
The total rate of complications and reoperations may increase to 10.9%–11.8% and 10.1% after LAGB application.15–17 Band slippage (1.4%–3%), erosion (0.2%–3.1%), acute stoma obstruction (1.4%), and port site complications (0.7%–5.3%) are the mostly seen postoperative problems.15–17 Complications developed in 2 patients. Port-site infection was determined in 2 patients. As the infection could not be controlled with medical treatment, the port and the band were removed. No mortality was seen.
IGB is a noninvasive and endoscopic method in which possible complications of surgery are not experienced. The most common complaints are nausea, vomiting, and abdominal cramps, which disappear in a week with medical measures.9,12 Severe complications such as bowel obstruction and gastric perforation are rarely seen.18,19 Another important feature of IGB is repeatability. A new balloon can be reinserted during the same session when the first balloon is removed. Some authors also recommend a 1-month interval between consecutive balloon applications.8,9 We prefer to replace the new balloon at the same session. In our patients we saw neither complication nor mortality related to IGB. Further, because the selected patients for IGB had mostly refused surgery, no one went to the definitive bariatric surgery.
Obesity is related to multiple comorbidities, including hypertension, diabetes, hypercholesterolemia, and sleep apnea. The weight loss improves or eliminates obesity-related comorbidities, and resolution mostly occurs in a year.19–21 At the end of the 18-month period, we also detected some improvement and resolution in comorbidities in our patients (Table 2).
Both the LAGB and IGB applications cause weight loss by restricting food intake. Although IGB is easy to apply and has very low morbidity and mortality, the requirement that it should not be left in the stomach for longer than 6 months is the most significant disadvantage. We determined in the study that weight loss achieved by two consecutive applications of the balloon is similar to LAGB. However, weight loss ceases after 12 months, and in fact, the patient begins to regain the lost weight. Similar results were described in the study by Herve et al. on a 12-month follow-up of IGB application and the results were characterized as “encouraging,” especially when combined with behavioral therapies. 19
In conclusion, when combined with a calorie-restricted diet and behavioral therapy and applied twice consecutively, IGB is as effective as LAGB for weight loss during a 12-month period. The regain of lost weight after removal of the balloon is the prominent disadvantage of the method; however, LAGB is more successful compared with consecutive two-time IGB application in weight loss and to maintain lost weight for a long period of time. However, we believe that more successful results will be obtained in the future with emerging endoscopic treatment alternatives.
Footnotes
Disclosure Statement
No competing financial interests exist.