
Abstract
Abstract
Background:
Laparoscopic hysterectomy (LH) is poorly adopted by general gynecologists. The aim of this study was to assess the differences between residents, general gynecologists, and laparoscopic-orientated gynecologists in the choice of surgical route in patients planned for hysterectomy.
Methods:
An observational study was carried out at a teaching hospital in south of The Netherlands. All patients who were planned for a hysterectomy for benign or premalignant indications between January 2005 and April 2009 were included. All performed hysterectomies were evaluated for the planned surgical route: vaginal, abdominal, or LH. Surgeons were divided into three categories: residents, general gynecologists, and laparoscopic-orientated gynecologists.
Results:
One hundred thirty-nine (35.8%) patients were planned for a vaginal approach, 151 (38.9%) for an abdominal approach, and 98 (25.2%) for a laparoscopic approach. The percentage of planned vaginal hysterectomies was comparable for all surgeons. There was a significant difference between the percentage of planned LHs by residents (30%) and that by general gynecologists (6%). As expected, laparoscopic-orientated gynecologists planned a laparoscopic approach in 53% of their cases.
Conclusions:
LH as alternative to abdominal hysterectomy is rarely planned by general gynecologists. Residents could play a role in the implementation of LH.
Introduction
Materials and Methods
Study design and participants
An observational study was performed in a teaching hospital in the south of the Netherlands, where LH has been introduced in 2005. All patients planned for a hysterectomy for benign or premalignant indication between January 2005 and April 2009 were included. All gynecologists and residents participated in the study. General gynecologist was defined as a gynecologist who participate weekly in general gynecological surgical procedures, including level I–II laparoscopic procedures (i.e., minor surgical procedures), but do not perform LHs. Laparoscopic-orientated gynecologists perform level I–III/IV procedures including LHs. One of the two residents was in the first year of training and the other in the last year of training. The resident training in The Netherlands is 6 years. During the first year, residents focus on obstetrics, but they also participate in the outpatient clinic. Patients are planned for surgery only after supervision of one of the gynecologists. Residents in their fifth and sixth year focus on the surgical aspects of our specialty, are trained in the operating room, and equally participate in the outpatient clinic. Residents were supervised concerning a fixed schedule in which all gynecologists equally participated. In our hospital, the primary surgical route for a hysterectomy for benign or premalignant indication is vaginal. Both the size of the uterus and vaginal access are the most important criteria. During the study period, the surgical route was planned based on the estimation of the primary surgeon. The study was exempt from institutional review board approval.
Outcome measurements
Patient age, indication for hysterectomy, previous surgery, planned operation, performed operation, operating time, and complications were registered. Surgeons who planned the operation were divided into three categories: residents (n=2), general gynecologists (n=6), and laparoscopic-orientated gynecologists (n=2).
Statistical analysis
The planned surgical routes, that is, vaginal, abdominal, or LH, were compared between the three categories of surgeons. Differences between these groups were analyzed by chi-square tests. P values below .05 were considered statistically significant. The SPSS software program (16.0) was used for statistical analysis.
Results
Participants
A total of 388 hysterectomies were performed during the study period. The indications for hysterectomy are demonstrated in Table 1. The majority of patients (73%) underwent a hysterectomy for bleeding disorders and symptomatic fibroids. One hundred thirty-nine (35.8%) patients were planned for a vaginal approach, 151 (38.9%) for an abdominal approach, and 98 (25.2%) for a laparoscopic approach. Of the 98 planned LHs, 4 patients underwent a vaginal hysterectomy when sufficient vaginal access was established under general anesthesia and 2 patients underwent an AH because of the fact that no laparoscopic-orientated gynecologist was available. In 11 (11%) patients, conversion to AH was necessary because of impaired mobility, adhesions, impaired access, or uncontrolled bleeding. Of those patients planned for a vaginal hysterectomy, conversion to AH was necessary in 5 (3.5%) patients because of insufficient vaginal access. All performed hysterectomies are presented in Figure 1 with the actual numbers of planned and performed procedures. Complications related to the performed surgical technique were present in 2% (3/137) of patients with a vaginal hysterectomy, 7% (12/170) of patients with an AH, and 11% (9/81) of patients who underwent an LH. The types of complications of the different surgical techniques are listed in Table 2.
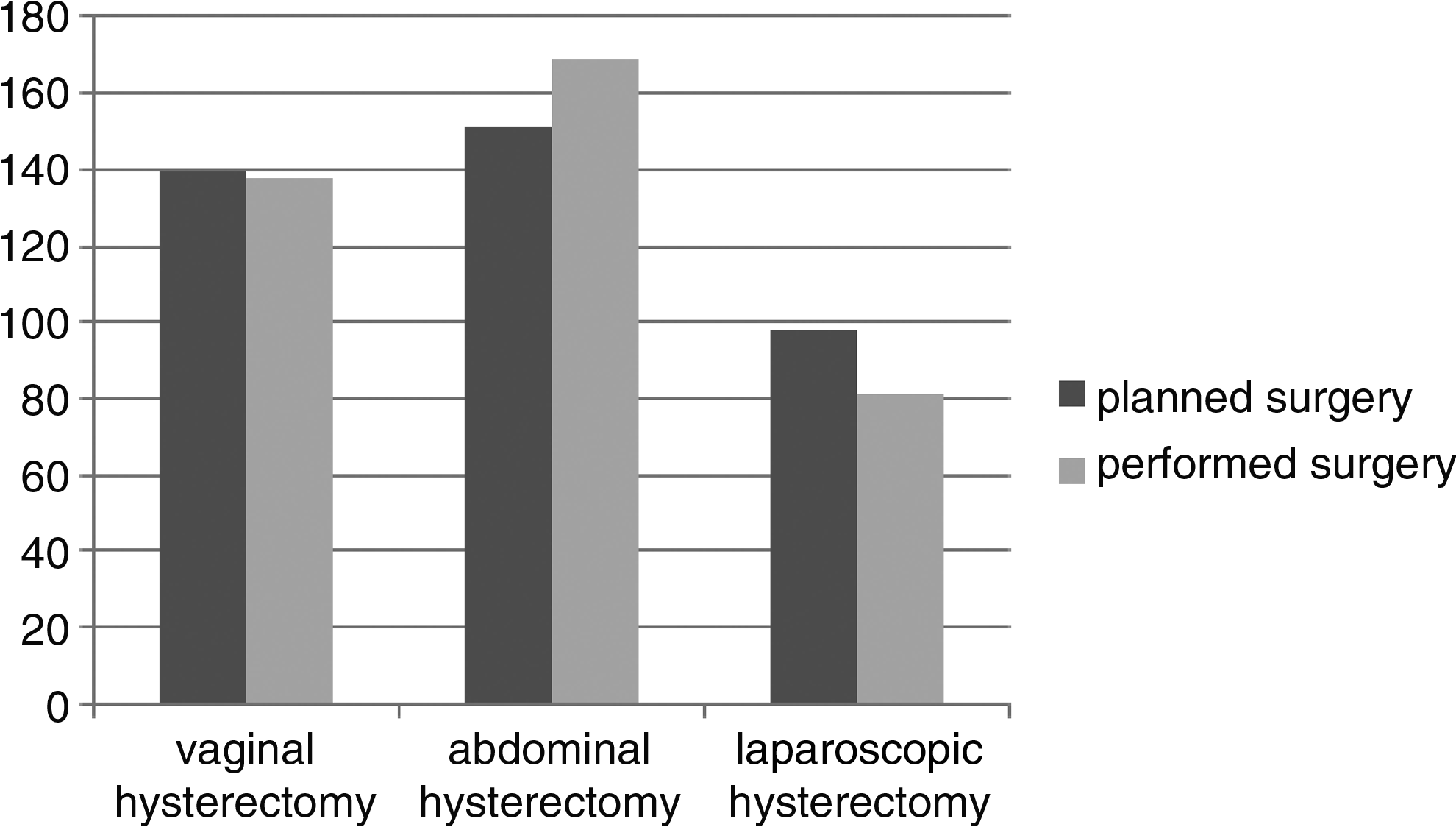
Actual numbers of planned and performed hysterectomies for the three different surgical routes.
Two patients with a ureter lesion underwent a second laparotomie for repair; these counted in the total number as one complication.
Primary outcome
The percentage of planned vaginal hysterectomies was not significantly different between residents, general gynecologists, and laparoscopic-orientated gynecologists (26%, 39%, and 33%, respectively). However, there was a significant difference between the percentage of planned LH by residents (30%) compared with general gynecologists (6%) (P<.05). Laparoscopic-orientated gynecologists planned a laparoscopic approach in 53% of their cases. In Figure 2, the percentages of planned surgical techniques are visualized for the different surgeons, that is, general gynecologists, laparoscopic-orientated gynecologists, and residents.
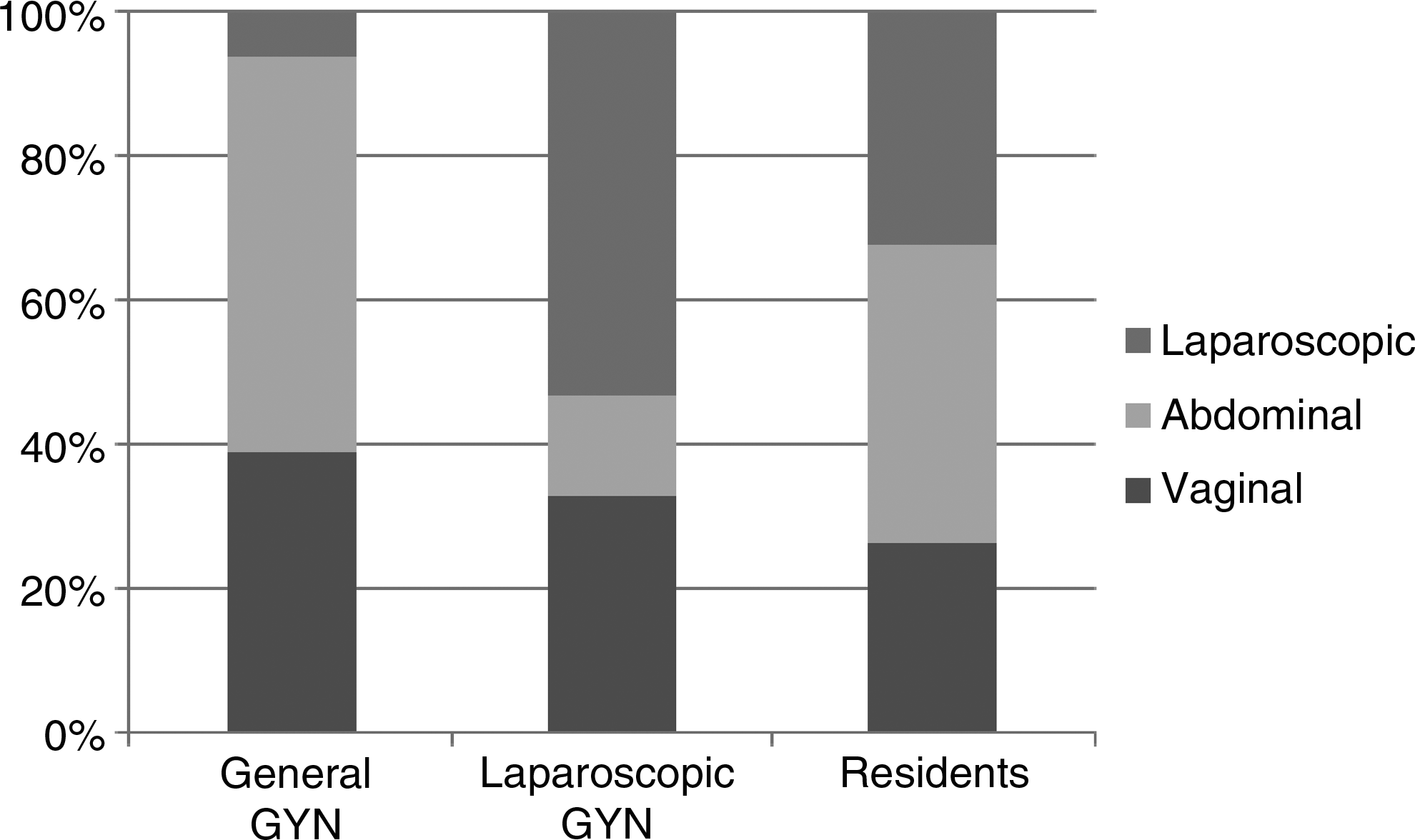
Percentages of planned surgical techniques for hysterectomy for general gynecologists (General GYN), laparoscopic-orientated gynecologists (Laparoscopic GYN), and residents.
Secondary outcome
Most hysterectomies (n=207) were planned by general gynecologists. Absolute numbers of planned hysterectomies per surgeon during the study period were 23 for residents, 35 for general gynecologists, and 68 for laparoscopic-orientated gynecologists. To demonstrate these absolute numbers for the planned surgical route for all types of surgeons, data are illustrated in Figure 3. As demonstrated for laparoscopic-orientated gynecologists, the increased number of patients selected for an LH reduced the number of AHs, compared with general gynecologists.
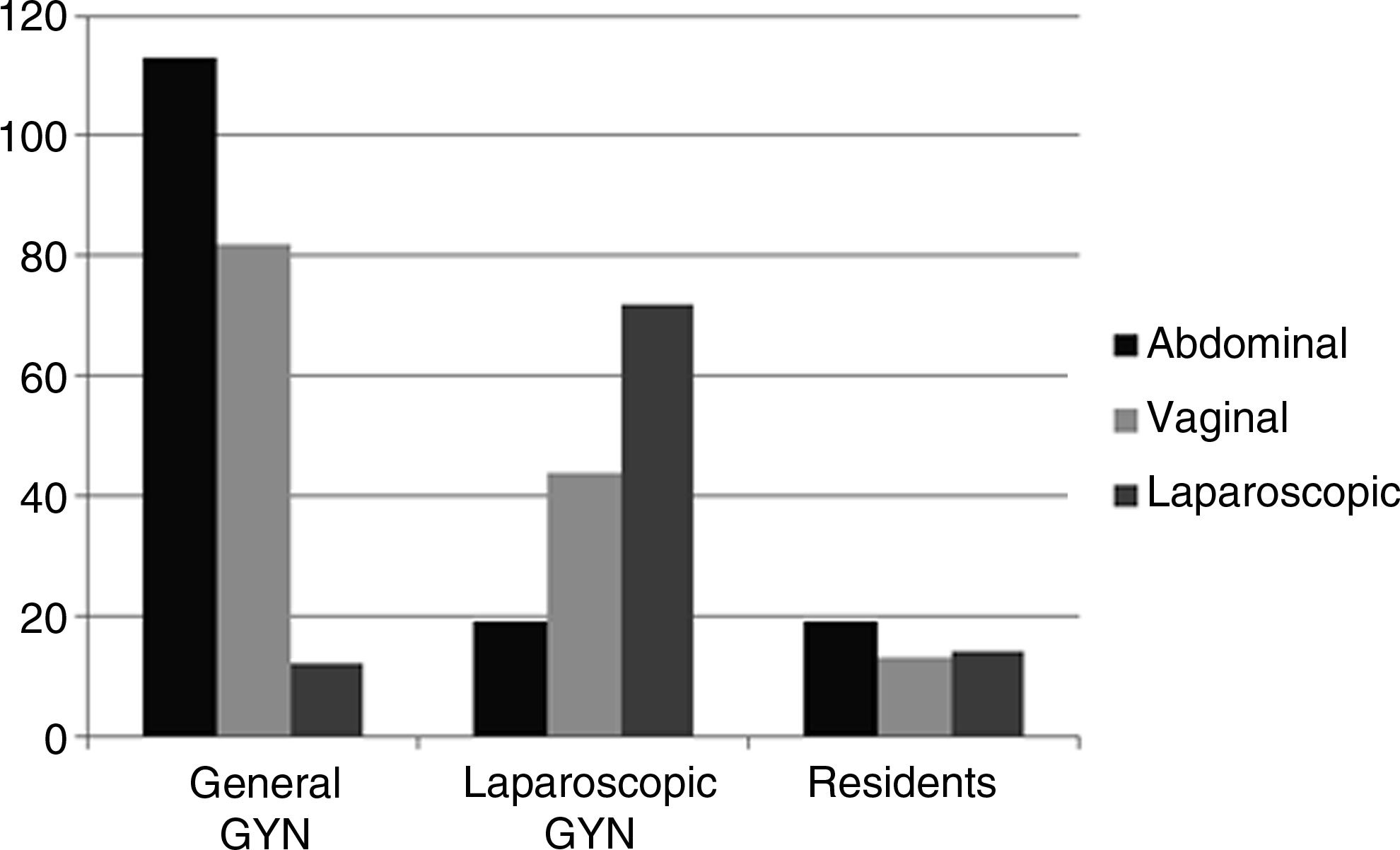
Absolute numbers of planned hysterectomies by surgical route for general gynecologists (General GYN), laparoscopic-orientated gynecologists (Laparoscopic GYN), and residents.
Discussion
This study reports on the differences in planned surgical route for hysterectomy for benign or premalignant indications by residents, general gynecologists, and laparoscopic-orientated gynecologists. The results of our study demonstrate that residents are more likely to plan patients for a laparoscopic approach when compared with general gynecologists. As expected, laparoscopic-orientated gynecologists selected the highest percentage of patients for a laparoscopic approach. Moreover, our data showed that planned LHs reduced the number of planned AHs without changing the percentage of vaginal hysterectomies.
The study is limited by its retrospective character and relatively small numbers. Although vaginal hysterectomy is the preferred surgical route in our hospital, the estimation of sufficient vaginal access as well as size is subjective. Information about the considerations that determined the choice of surgical route was limited, and documentation of whether the option of an LH was discussed with the patient planned for AH was unfortunately not available. LHs were performed in our hospital since 2005, the start of the study period, and although the learning curve was partially completed in other hospitals, this could explain the relatively high conversion rate. Yet, it is difficult how to interpret the conversion rate in laparoscopic procedures. If none of the LHs is converted to an open procedure, it is likely that too many women undergo an abdominal procedure. On the other hand, if >50% of the cases are converted to open procedures, one can doubt about the laparoscopic surgical skills or surgeon's estimation. The strength of the present study is the fact that these data perfectly reflect the early processes in adaptation of new surgical techniques in clinical practice. Most data of LHs are from large trials and large hospitals where gynecologists are specialized in laparoscopic procedures. However, still a significant number of our patients are treated in general hospitals with all-round gynecologist that may explain the poor adaptation of the LH.
To our knowledge, this is the first report that demonstrates the role of residents in the adoption of new surgical techniques, and therefore, our data could not be compared with other studies. The percentages of planned vaginal hysterectomies were similar in all three groups of surgeons and data are comparable to data in literature. 7 We speculate that the fact that residents seem to be more open to new techniques could be explained by more flexibility, better insight in the laparoscopic skills of the supervisors, and shared experiences with other residents and other hospitals. It is interesting to note that these residents who are increasingly confronted with declining numbers of major gynecological operations and a wider range of techniques that should be learned seem to be more open to new techniques.8,9
Although many laparoscopic procedures have been introduced by now, it is not clear which factors determine the speed of implementation. Compared with laparoscopic cholecystectomy, which was introduced at about the same time as the LH, there is a large difference in adoption of the technique.10,11 Laparoscopic cholecystectomy was rapidly diffused into clinical practice as this operation seemed to be a fusion of two proved safe technologies: open cholecystectomy and laparoscopy. Unfortunately, the procedure was associated with a substantial increase in biliary tract injury. 12 Because of this increased complication risk, surgery was adopted, and currently, complications are equal, with a preference for the laparoscopic cholecystectomy over the open procedure.13,14 When considering the introduction of an LH, adoption is slow in The Netherlands, 15 but in analog with cholecystectomy there seems to be an unexplained increased risk of complications for this new technology. The percentage of complications in our series is in accordance with reported data (11.1%) for LHs, compared with 6.2% in AH, and is mainly due to an increased number of injuries of the urinary tract. 3 Probably, the increased complication rate is one of the reasons why general gynecologists are skeptical to advise this procedure to their patients and hesitate to refer to their colleagues. It seems that there is a certain learning curve until an equal risk of complications is reached when compared with vaginal and abdominal surgeries. 7 Others have stated that, even during the learning curve, LH can be performed safely at a low complication rate. 16 Recently, Donnez et al. demonstrated in a large series that in experienced hands the LH was not associated with a higher risk of ureter lesions. 17
The hesitation of general gynecologists in implementation of new surgical techniques should be reflected in view of the changing working field in the last decades. The introduction of subspecialists for gynecologic oncology, perinatal medicine, assisted reproduction, and recently, urogynecology may be one of the reasons. By the introduction of LH and pelvic floor reconstructions, the AH is one of the few operations left for a general gynecologist. Although evidence-based medicine should nowadays define clinical practice, a large Swedish study demonstrated that several factors, not related to the evidence-based medicine principle, determined the preferred route of hysterectomy. 6 Yet, our patients should be equally informed about the advantages and disadvantages of LH.
We wondered how to lower the percentage of AH and assist in a proper selection of patients suitable for LH. Kovac et al. demonstrated in a large series that resident physicians following a guideline for the selection of the route of hysterectomy reduced the ratio of abdominal-to-vaginal hysterectomy from 3:1 to 1:11. 18 We have adjusted their flow chart with focus on vaginal hysterectomy as the primary route of surgery for benign and premalignant reasons (Fig. 4). Only if vaginal hysterectomy is not possible, LH could be performed as an alternative to AH. As the experience of laparoscopic-orientated gynecologists may differ, the exact uterine sizes in the guideline may differ in various centers. This flow chart is currently used and prospectively collected results will be reported in the future. Finally, mentor traineeship and virtual reality training could be used to facilitate the implementation of laparoscopic surgery into an established gynecological practice.19,20
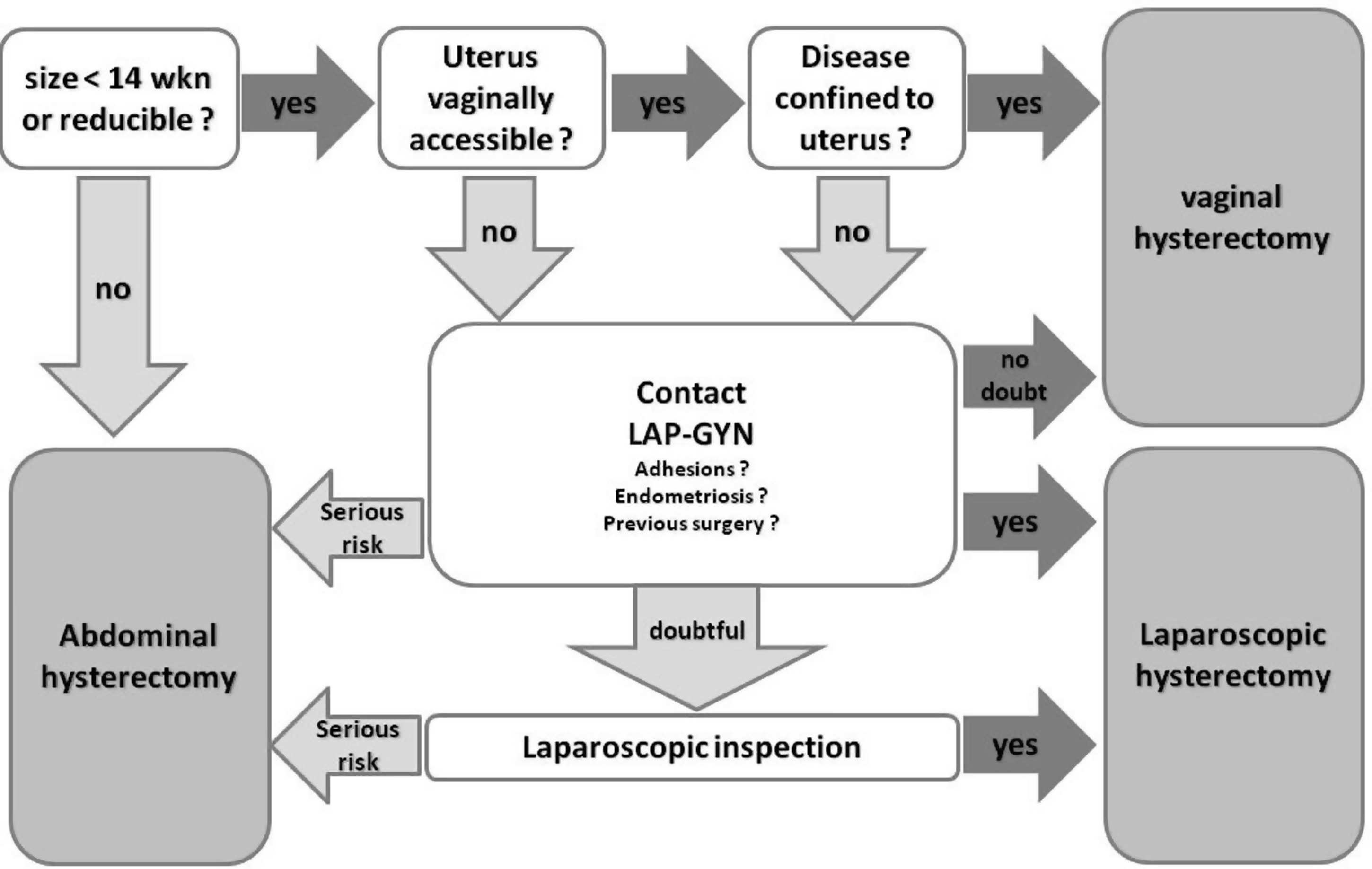
Flow chart for planning the surgical route for patients with benign or premalignant indication for hysterectomy.
In conclusion, since the introduction of LH, its implementation in general gynecologists practice is only slow. Residents seem to play an important role in a changing attitude toward the mode of hysterectomy. A flow chart as a practical guideline may facilitate the selection of patients for vaginal, laparoscopic, and AH but should be prospectively evaluated.
Footnotes
Acknowledgment
The authors kindly thank K.B. Kluivers for critical reading of the manuscript.
Disclosure Statement
No competing financial interests exist.