
Abstract
Abstract
Introduction:
Notes is the logical answer to scarless surgery, but despite being around for almost 4–5 years, it has to still garner a major support because of a number of limitations. Single-incision laparoscopic surgery, especially when done through the umbilicus, should be the perfect answer as far as the absence of any visible scar is concerned.
Materials and Methods:
All the 67 patients were operated by the same surgeon through a transversely placed umbilical incision in the lower half of the umbilicus. Three conventional ports, 10, 5, and 5 mm, were introduced through the same skin incision but separate transfacial punctures. The instruments included 10-mm and 5-mm 30° rigid telescopes and rigid instruments as in standard laparoscopic cholecystectomy. Patients with irreducible hernia and obstructed hernia were included, and those with strangulated hernia were excluded.
Results:
All the patients were men, with an average age of 38.6 years. Three patients had bilateral hernia and 2 each had irreducible and obstructed hernia. The mean operating time was 42.8 minutes for unilateral hernias when tackers were used and 51.7 minutes in those in whom intracorporeal suturing was done. The operating time for bilateral hernias was 71.7 minutes. There was minimal flap discharge, without infection, in 3 patients. There were no other complications. There were no conversions and no recurrences upto 9 months of follow-up.
Conclusions:
Transumbilical single-skin-incision laparoscopic transabdominal preperitoneal repair for groin hernias, performed solely with conventional instruments, is feasible, easy to learn, and probably the future of laparoscopic inguinal hernia repair.
Introduction
Materials and Methods
All the patients presenting with operable inguinal hernias in our unit, from October 2010, are now being offered SILTAPP as the first option, and informed consents were obtained. The prerequisite preoperative investigations and preparations were then carried out.
The patient is positioned 10–20° head down with hernial side upward tilt 10° and arms by the side. Carbon dioxide pneumoperitoneum of 8 mm is created with a Veress needle. A transversely placed curved incision with concavity upward is centered over the lower half of the umbilicus and the lower flap is undermined (Fig. 1). A 10-mm trocar is inserted along with two 5-mm tube trocars, flanking it on either side, and positioned in a straight transverse line with a distance of 0.5 cm in between the transfacial punctures and directed toward the side of the hernia (Fig. 2). The right 5-mm trocar (patient's right) accommodates, alternately, rigid scissors, graspers, and a needle holder and the left 5-mm trocar accommodates a grasper. It is important to use tube nonvalve 5-mm trocars (Fig. 3). This prevents the clashing of the trocars. If all the three trocars were to be of valve type, the thick valvular parts will clash with each other because the distance between them is only 0.5–1 cm.
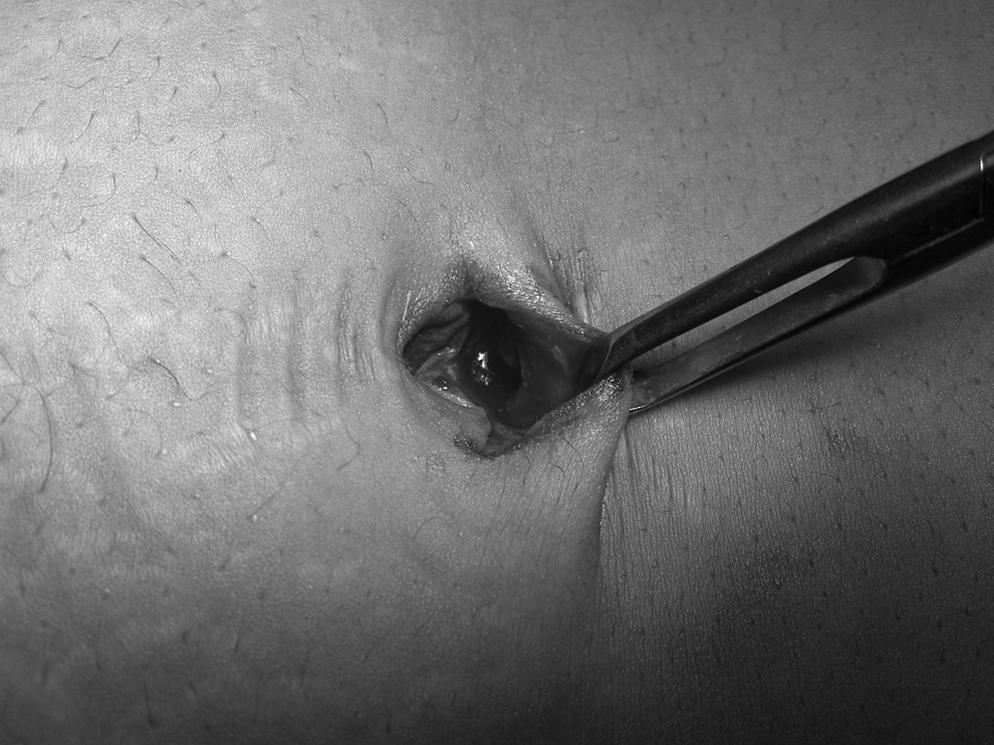
Lower umbilical flap.

Port placements.

Five-millimeter nonvalve ports.
The surgeon stands on the side opposite to the hernia just as in standard laparoscopic TAPP repair. The camera assistant stands positioned caudal to the operating surgeon.
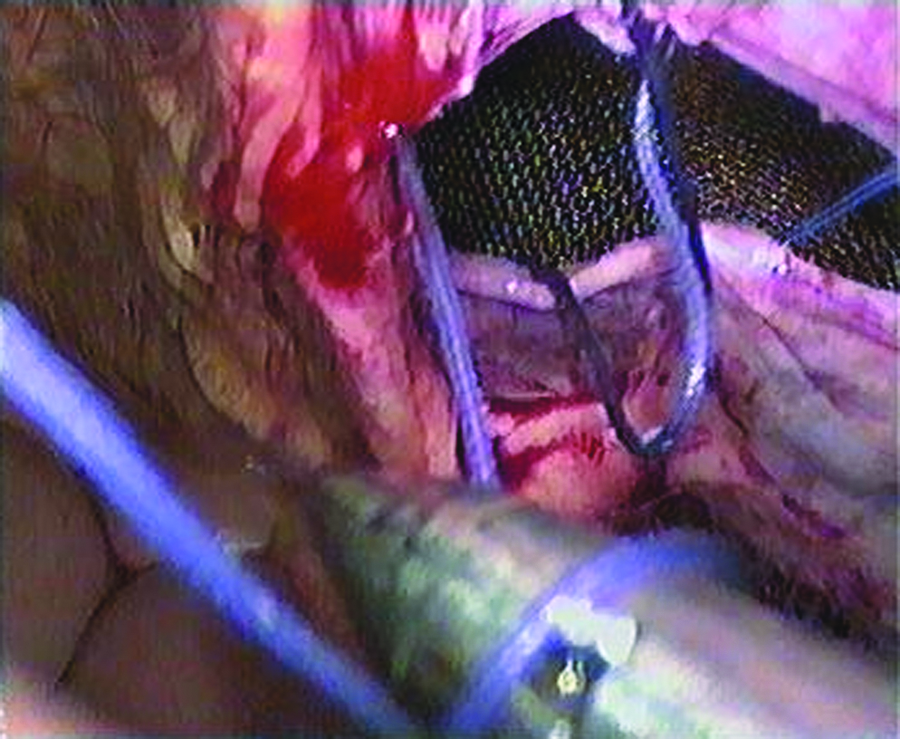
The steps of the repair are exactly the same as for a standard TAPP repair (STAPP). Just to emphasize the important steps, the parietal peritoneum is incised about 5 cm cranial to the deep inguinal ring and the incision is extended medially to the medial inguinal ligament and laterally to beyond the vertical line of anterior superior iliac spine. The lower peritoneal flap is then dissected away from the abdominal wall, with blunt and sharp dissection, but more by blunt dissection. The flap is dissected to the medial and lateral limits as in STAPP. Next, the sac is identified and dragged in by a hand-over-hand maneuver and separated from the cord structures with blunt and sharp dissection (Fig. 4). The peritoneum is further stripped off the psoas muscle until an adequate preperitoneal space has been created to place a 10 × 15 cm polypropylene mesh. The mesh is positioned to cover the Fruchaud orifice and extends upto the midline and is then fixed with two tackers, one at the pubic bone and other near the lateral and upper end, 2–3 cm above the anterior superior iliac spine. The lower peritoneal flap in the initial few patients was then tacked to the upper flap with tackers. In the subsequent patients, the flaps were approximated with intracorporeal continuous suturing using 3-0 vicryl. The suture is introduced into the abdomen directly through the abdominal wall at the medial or lateral end of the peritoneal incision. The needle, along with the suture of the estimated required length, is dragged in with a needle holder, and suturing is started with a bite of the lower flap (Fig. 5) and then of the upper flap (Fig. 6). The suturing is terminated with an intracorporeal knot (Fig. 7). The proximal end of the suture, which is still traversing the anterior abdominal wall, from where it was introduced, is now pulled up tight making the suture line taut. This end of the suture is then cut after tying an extracorporeal knot.
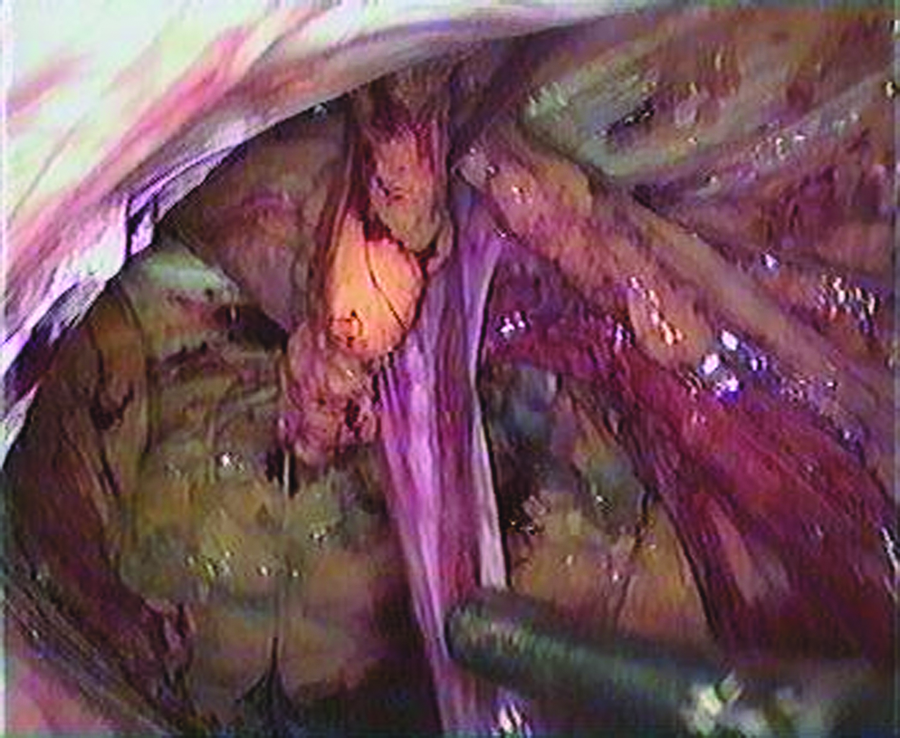
Sac dissected from cord structures and vas deferens.
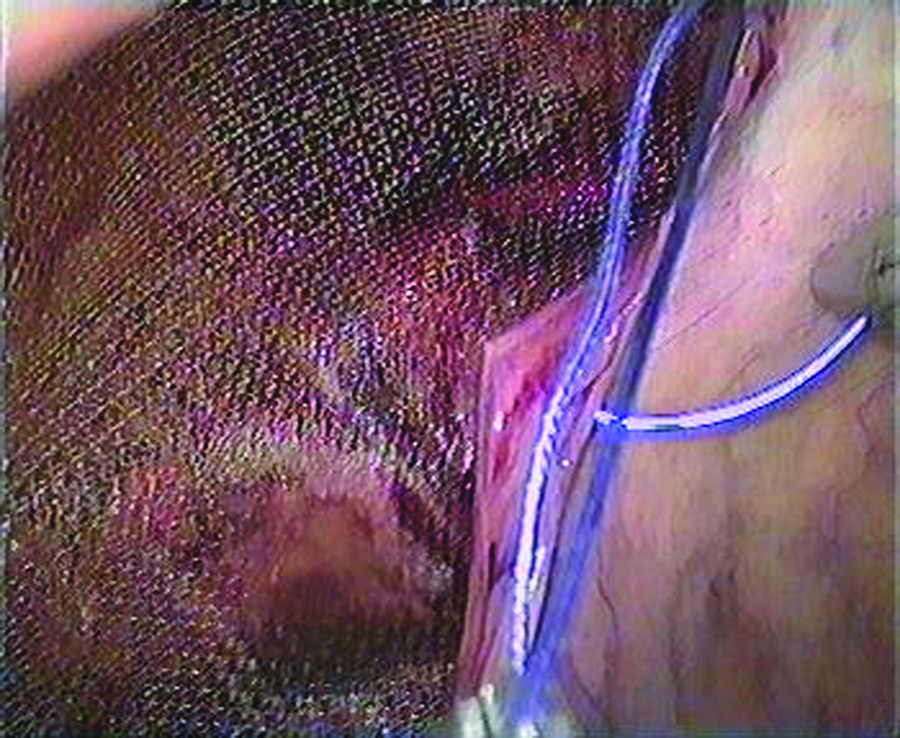
Intracorporeal suturing started laterally lower flap.
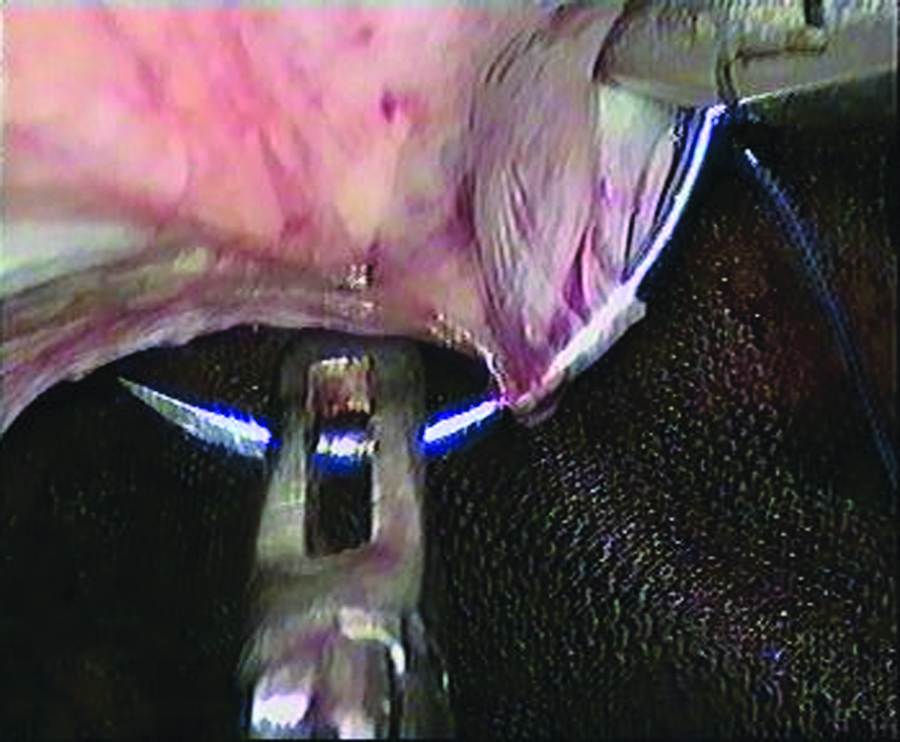
Needle passed through the upper flap.
Intracorporeal knotting.
The transfacial port-site punctures and the umbilical incision are closed using 2-0 vicryl over 40-mm ½ circle reverse cutting needle (Fig. 8). The extracorporeal knot is cut at the time of the first follow-up of the patient.

Closed umbilicus.
For the alleviation of postoperative pain, 100 mg Tramadol is administered in the i.v. fluid being supplemented. Subsequently, the dose may be repeated once if the patient feels pain within 24 hours of the operation. Opiods are not given after that. The patient is then shifted onto oral tablets of diclofenac and paracetamol combination, to be taken if required, for pain. Even at discharge, the tablets are recommended to be taken if required.
Monitored parameters include the operating time, per- and postoperative complications, number of injectable doses of analgesic, total duration of requirement of oral analgesics, and postoperative ileus and umbilical site infection. Long-term recurrence is assessed at 1 and 6 months and will also be assessed at 1 year postsurgery.
Results
Sixty-seven hernias were operated on 64 patients between October 2009 and July 2010. All patients were men, with an average age of 38.6 years. Hernia demographics are available in Table 1. The average operating time for unilateral hernia was 42.8 minutes (32–61 minutes), when tackers were used in the initial 5 patients, and 51.7 minutes (42–81 minutes) where intracorporeal suturing was done. In bilateral hernia, we preferred the tacker over the suture and the operative time period was 71.7 minutes (61–85 minutes). Complete sac retraction was possible in 56 patients. In the rest, the sac was transected after it was dragged in for about 4–6 cm and ligated. There were no peroperative complications or conversions. Injectable analgesic was required in 45 patients (70.31%). Twelve patients required a second dose. None of the patients required any form of oral analgesic after 36 hours.
Discharge time was 1.6 days (1–3 days). Serosangunious port-site discharge persisted in 3 patients for 3–4 days, but there was no wound site infection. There were no recurrences upto a maximum follow-up time of 9 months (Table 2).
U/L, unilateral; B/L, bilateral; IC, intracorporeal.
Discussion
SIL surgery (SILS), which was carried out for the first time in 1969, was a gynecological procedure. 1 Soon thereafter, the first surgical excision performed by the laparoscopic general surgeon through single incision was an appendectomy.2–4 But these were not truly single-incision surgeries, because an operating laparoscope was used in all these.
The first truly single-incision surgical procedure was an appendectomy performed in 2005 and the first SIL cholecystectomy was performed by Navarra 4a in 2007 and later by others.6,7 Since then, the repertoire of the SIL surgeon seems to be increasing by leaps and bounds, and during the last 2–3 years, the horizon has gradually expanded to include almost all advanced laparoscopic surgeries including urological applications,8,9 gynecological interventions, 1 colorectal surgery,10,11 and bariatric surgery.12,13 This, in large part, has been made possible by the advent of transumbilical ports, such as triport and airseal port, which have multiple entry points. The procedures have been further facilitated by the recent introduction of rotating instruments and curved instruments.14,15
However, reports of groin hernias being operated through a single incision are still very few and even those reported are reports of very small numbers of patients. In all the series reported, single-incision TEP repair appears to be the favored procedure, in contrast to TAPP.
The site of the incision differs, being supraumbilical, 16 infraumbilical,17–20 or transumbilical.21–23 We prefer the transumbilical approach, and in all our patients, the ports were introduced after the lower umbilical flap has been mobilized (Fig. 1). In all the reports, the incision size varies between 2.0 and 3.0 cm. Our incision size also varies between 2.5 and 3.0 cm. It is obvious that the transumbilical incision, rather than a supra- or infraumbilical incision, will result in a more cosmetic scar and a nearly normal looking umbilicus.
Most of the reports mention TEP repairs having been performed with special umbilical ports. Bucher 18 reported on 4 patients who were operated on through the Covidien port. Agarwal 19 reported on a larger group of 16 patients, in whom 19 TEP procedures were performed with the triport system, and Jacob 20 also performed all his TEP repairs through a Covidien port. In contrast, TEP with routine ports has been mentioned by Cugura et al., 21 who used three different transfacial ports through the same infraumbilical incision to complete their TEP. But three transfacial ports cannot be introduced into the preperitoneal space through an umbilical incision. The skin incision would have to be infraumbilical and thus the cosmetic advantage would be lost. So to retain the cosmetic advantage of an umbilical incision, TAPP appears to be a better option.
Series reports for SILTAPP repair for inguinal hernias are also very few and interspersed with case reports. Krischniak 17 reported on TAPP with a 3–5-mm port through an infraumbilical incision and routine rigid instruments. But this study was a feasibility study done on 3 cadavers. Menenakos et al. 16 reported on a patient with bilateral inguinal hernia, in whom they performed an SILTAPP. The incision was supraumbilical and triport access was used; however, the type of instruments has not been mentioned. 16 Ishikawa et al. 22 reported on a patient with inguinal hernia, in whom TAPP repair was done with the aid of radius surgical system for suturing. A series of 15 patients, in whom TAPP had been carried out, has been reported recently. 23 Routine ports and rigid instruments have been used in this study. We also perform all our procedures with routine one 10-mm and two 5-mm tube ports and routine rigid instruments. Krischniak 17 mentions the use of flexible instruments.
The peritoneal closure in STAPP is routinely performed using tacks and very rarely by intracorporeal suturing. There is a study of SILTAPP wherein the flap closure after mesh insertion has been done using a suturing system. 22 The other studies do not specifically mention the method of closure of the peritoneal flap and it probably means that it was with the conventional method of using tacks. Even in the study by Roy and De, 23 closure of the peritoneum was done by intracorporeal sutures in the first 2 patients only. Subsequently, they used tacks because they found suturing to be technically difficult. We have now operated on 64 patients, and after the first 5 patients in whom we used tacks for peritoneal flaps, we now do intracorporeal suture closure of the peritoneal flaps. The suturing in the initial stages was demanding, but once we learned to do it right, we could accomplish it fairly easily. Our completion of the whole procedure on unilateral hernias in 51.7 minutes, which included the suturing time, bears testimony to this assertion, as this time matches 54.11 minutes 23 and 45.5 minutes 1 reported for completion of SILTAPP where only tacks had been used. In contrast, an operative time of 120 minutes has also been reported for the same procedure with tacks. 16
The requirement of analgesics was apparently less than in an STAPP because only 40 patients demanded an injectable analgesic postoperatively and 16 of them required a second dose. None of the patients required any analgesic after 36 hours. There were no conversions, complications, or recurrences.
SILS procedures require some modification in the technique of standard laparoscopic approach. The problem of clashing of ports was offset by using two 5-mm simple tube trocars flanking the 10-mm trocar with 0.5–1.0 cm interval in between the transfacial punctures of the ports (Fig. 3). The problem of clashing of rigid instruments either outside or inside the abdomen is also minimized by the 1.5–2.0 cm interval between the two 5-mm ports through which the instruments are introduced. The triangulation is easily achieved by crossing of the instruments inside the abdomen, which is a necessary maneuver during the procedure. Thus, there is absolutely no change in the essential steps of the procedure when compared with an STAPP. There is a learning curve, which in our case was only about 20 patients in whom we had to learn to suture with closely parallel rigid instruments, but then we were graduating from other single-hole laparoscopic surgeries, which we have been doing since the last 10 months. Hence, the initial instrument handling had already been learnt. Even the problem of learning to suture can easily be circumvented if tacks are used to close the peritoneal flaps, but then the cost of surgery increases. The final scar at 1 month postoperatively was almost not visible and gave a very cosmetically acceptable result (Fig. 9). This has to be compared with the routine TAPP repair wherein three ports are used: the first 10-mm port is an infraumbilical port and the rest two are 5-mm ports on either side, in the same horizontal line, at the lateral border of the rectus. This results in three scar sites, which is a disadvantage when compared with the SILS scar, which is hardly visible and hidden in the folds of the umbilicus.

Umbilicus at 1 month.
Conclusion
We have demonstrated that SILTAPP is feasible, but the question is why is it needed and does it confer any benefit over the STAPP. Is it only a cosmetic improvement, which is remarkably true? The initial impression of a lesser degree of pain has not been statistically substantiated. Also, questions regarding the long-term incidence of possible postoperative port-site umbilical hernias and other possible complications can only be answered after long-term results of at least 3–5 years become available, which will take some time. But the most astonishing fact is that despite being fully informed about these lacunae, there is total patient acceptance of and preference for the SIL procedures. But then, this is hardly surprising, if we remember that even the acceptance of laparoscopic cholecystectomy as the gold standard was despite a statistically higher common bile duct injury rate in the initial stages and even now, when compared with the open procedure, and this was in a great part driven by the preference exhibited by the patients.
Footnotes
Disclosure Statement
No competing financial interests exist.