
Abstract
Abstract
Background:
Ascites leaks (AL) in patients with end-stage liver disease (ESLD) are associated with significant morbidity and mortality regardless if they are medically or surgically managed.
Patients and Methods:
In a pilot study, 14 ESLD patients with AL underwent treatment with fibrin glue injection around the leak after failing conservative therapy. The end point of this study was the cessation of AL in the short term and the maintenance of a leak-free abdomen in the long term, allowing for medical optimization of the patients.
Results:
Median age of the 10 men and 4 women was 50 (range 26–67) years. Underlying ESLDs were chronic hepatitis C (n=5), alcoholic LD (n=2), cryptogenic cirrhosis (n=2), and miscellaneous (n=5). There were six leaking incisions posthernia repair (three umbilical and three inguinal), two leaking/ruptured umbilical hernias, four leaking paracentesis sites, one leaking Jackson–Pratt (JP) drain canal, and one leaking laparoscopic trocar site. Average AL volume per day was 1000 (range 400–2000) mL. All leaks were immediately resolved with a 3–5 mL fibrin glue injection. Five recurred and required a second injection (four within 24 hours). Mental status improved in 7 patients (West Haven Criteria: grade II to I [n=6], grade III to I [n=1]). Median model of end-stage liver disease scores improved from 23 (range 8–33) to 20 (range 14–26). There were no infections, bleeds, or other injection-related complications. Average follow-up for these patients was 441.6 days (range 2–852). Five patients underwent liver transplant (LT) median 15 (range 4–270) days postinjection; 2 of them died. Another 3 patients died (2 from sepsis and 1 from metastatic cancer).
Conclusion:
Fibrin glue injection for the control of AL is a simple and safe bedside procedure that quickly controls AL, allowing for patient recovery in anticipation of further care.
Introduction
Patients and Methods
Patients with AL were identified by the transplantation and hepatology services and referred to the surgeons for treatment at the University of Virginia Medical Center between July 2007 and June 2008. A total of 15 patients were referred and 14 were included in this pilot study with the exclusion of 1 patient who had a wound infection at the leaking site at time of referral. Severity of liver failure before injection was assessed by calculating the model of end-stage liver disease (MELD) score and the Child-Pugh Score for every patient at the time of fibrin glue injection. Hepatic encephalopathy was evaluated using the West Haven Criteria.
This study was approved by the local ethics committee. Data are given in percent of the cohort for discrete parameters and median with range and/or mean with standard deviation for continuous parameters. Statistical analysis was performed using SPSS, a P value of <.05 was considered statistically significant. Continuous parameters of related samples were analyzed using the nonparametric Friedman test.
Inclusion/exclusion criteria
Inclusion criteria were a diagnosis of ESLD diagnosed on clinical, biochemical, and/or histologic findings, presence of ascites diagnosed with either ultrasonography or computed tomography, and presence of an AL confirmed on physical examination and failure of improvement with conservative management. Exclusion criteria were presence of wound infection at the planned injection site and severe coagulopathy (international normalized ratio [INR]>3.0) or thrombocytopenia (platelet count <20,000/mL).
Preinjection management
Conservative management in these patients consisted of forced diuresis. Paracentesis had been performed in 8 patients removing median 1500 (range 200–5000) mL ascites. In 5 patients, an attempt to close the leak with a stitch had failed.
Technique
Fibrin glue injections were performed at the bedside using sterile techniques.16,17 Tisseel glue (Tisseel™; Baxter Healthcare Corporation) was mixed as per the product instructions. Although this is a novel use of this substance, this is not an off-label use of the product, which clearly defines subcutaneous injections for a wide range of situations. Patients were placed in supine position and the abdomen was sterilized using chlorhexidine solution and draped in a sterile fashion. In case of a hernia, all contents were gently reduced into the abdominal cavity. The leaking area was identified. Approximately 5 mL of fibrin glue was injected subcutaneously and deeper into the peri-leak tissue using a 19 gauge needle obliterating the tract. Injection was continued while withdrawing the needle from the tissue at the site to ensure seal of the needle puncture. A 4×4 gauze pressure dressing was applied for 48 hours.
Postinjection follow-up
The end point of this study was the cessation of AL in the short term and the maintenance of a leak-free abdomen in the long term, allowing for medical optimization of the patients. Laboratory values (Total bilirubin, creatinine, albumin, and prothrombin time) and clinical status (including West Haven Criteria for assessment of encephalopathy) were monitored postinjection every day until the date of discharge. MELD and Child-Pugh scores were calculated on postinjection days 1, 3, and 7 or at discharge. The wound was inspected upon removal of pressure dressing on postinjection day 2. Routine follow-up occurred at our hepatology outpatient clinic and by telephone correspondence for an average of 441.6 days (range 2–851).
Results
There were 10 men and 4 women with a median age of 50 (range 26 to 67). Underlying liver diseases included chronic hepatitis C (n=5), alcoholic liver disease (n=2), cryptogenic cirrhosis (n=2), alpha-1 antitrypsin deficiency (n=1), nonalcoholic steatohepatitis (n=1), portal venous thrombosis (n=1), primary portal hypertension (n=1), and massive hepatic metastatic disease secondary to colorectal cancer (n=1). One patient had Child A, 4 had Child B, and 8 had Child C cirrhosis (1 had no cirrhosis). Tables 1 and 2 show demographic and clinical data of the 14 study patients.
MELD, model of end-stage liver disease; HCV, hepatitis C virus; ALD, alcohol liver disease; NASH, nonalcoholic steatohepatitis; PVT, portal vein thrombosis; PPHTN, primary portal hypertension; ND, not done; NA, not available.
LT, liver transplant; MOF, multi-organ failure; MRSA, methicillin-resistant Staphylococcus aureus; n/a, not applicable; NA, not available.
There were six leaking incisions posthernia repair (three umbilical and three inguinal including four cases of incarceration), two leaking/ruptured umbilical hernias, four leaking paracentesis sites, one leaking laparoscopic trocar site, and one leaking abdominal drain site. Median AL volume per day was 1000 (range 400–2000) mL. All of these leaks had failed a trial of conservative management (diuresis in 11, paracentesis in 8, and stitch in 5 cases). Leaks had been present median 3 (range 2–7) days. Preinjection INR averaged 1.8 (range 1.4 to 2.8). All leaks were immediately resolved with a 3–5 mL fibrin glue injection as described. Five leaks recurred and required a second injection within 24 hours of the first injection, and all second attempts were successful.
Within 1 week after injection, albumin levels steadily improved in 7 patients (50%), remained stable in 4, and worsened in the remaining 3 individuals; the overall changes did not reach statistical significance. Median serum creatinine improved from 1.2 (range 0.8–2.3) mg/dL to 1.1 (range 0.8–2.8) mg/dL on day 3, P=.824, n.s.; creatinine improved in 5 patients, remained unchanged in 4, and worsened in another 5. Median Child-Pugh scores improved from 11 (range 6–14) to 10 (range 7–11) on day 3 and 11 (range 8–12) on day 7, P=.029; 6 patients experienced improvement, 5 had no change, and 3 had worsening scores. The median MELD score improved from 23 (range 8–33) to 20 (range 14–36) on day 7, P=.064 (Fig. 1), the MELD score improved in 6 patients, remained unchanged in 4, and worsened in 4 patients.
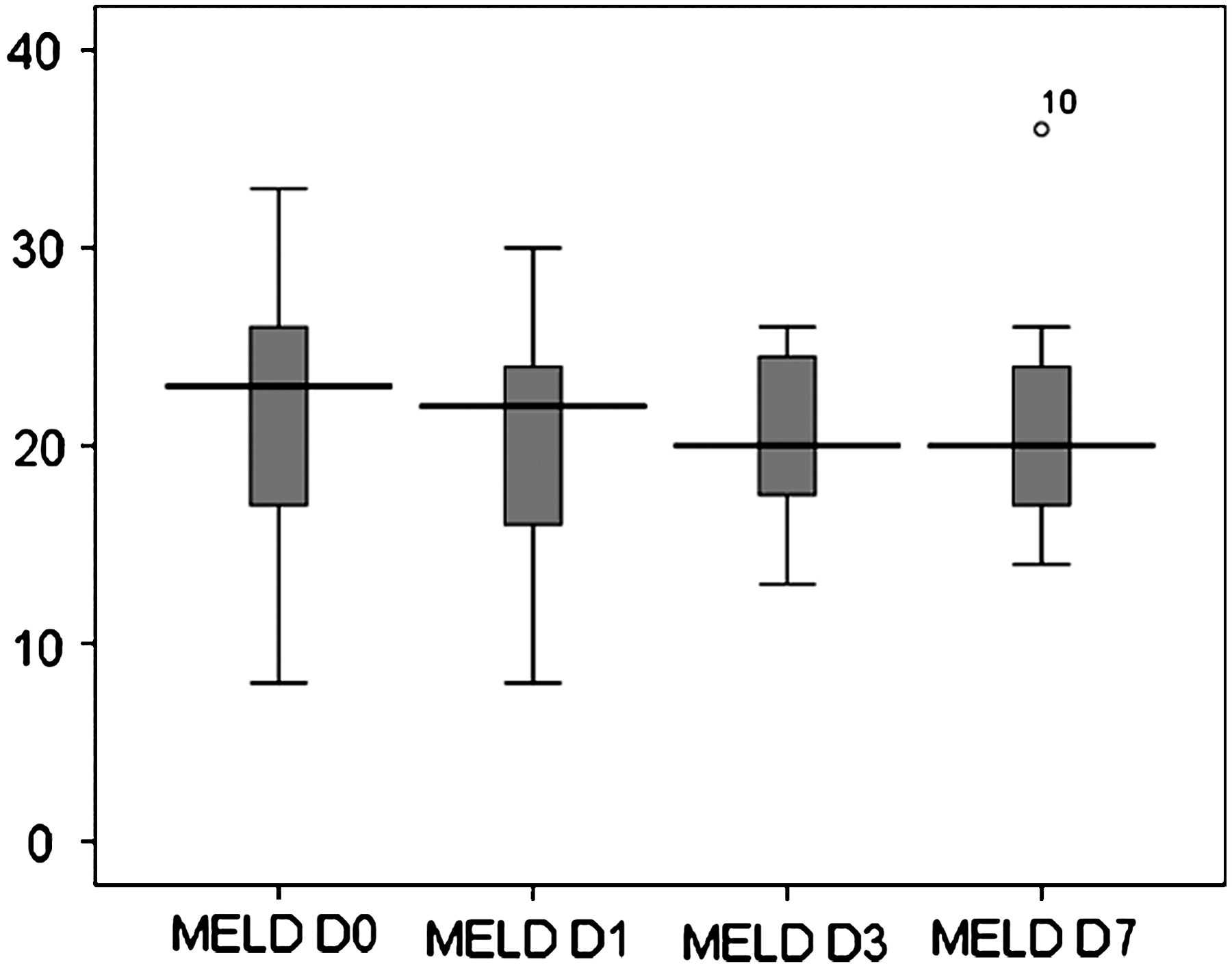
Box plots of model of end-stage liver disease (MELD) scores at baseline, 1, 3, and 7 days postinjection, P=.065, n.s.
Within 1 week after the injection, mental status improved in 7 patients; in the remaining, no changes were observed. Using the West Haven Criteria, mental status improved from grade II to grade I in 6 patients and from grade III to grade I in 1 patient.
Discharge occurred median 5 (range 2 to 15) days after injection. There were no infections and no other complications associated with the intervention. The average time of follow-up for the 14 patients was 441.6 days (range 2–852). Two patients were lost to follow-up 2 and 12 days after the injection. Five patients did succumb to their disease. None of the deaths were temporally related to the fibrin glue injection or a recurrent leak.
Both patients with ruptured umbilical hernias underwent repair (one elective one as an emergency procedure). The elective repair was performed 6 weeks postinjection after the patient had significantly improved in his general condition after closure of the leak. Repair consisted of continuous closure of the peritoneum, and interrupted suture closure of the fascia. This patient had no complications and continuous stable liver disease; he underwent liver transplant (LT) later on. The other patient developed acute abdomen due to incarceration of a small bowel loop within the large umbilical hernia 9 months after injection; however, there was no recurrent leak. He underwent emergency laparotomy and the necrotic small bowel segment was resected with side-side anastomosis. This anastomosis had a break down and the patient ultimately died from uncontrolled intra-abdominal sepsis. One patient died 5 weeks postinjection from methicillin-resistant Staphylococcus aureus (MRSA) pneumonia and the patient with the metastatic colonic cancer succumbed to his malignant disease within few days postinjection.
Five of the 14 patients underwent LT median 15 (range 4–270) days postinjection. One patient died during the LT from cardiac arrest unrelated to the fibrin glue injection and another from recurrent hepatitis C and multiorgan failure 15 months post-LT. The remaining 3 patients are currently alive with functioning grafts. All patients with hepatitis C developed recurrent liver disease.
At last follow-up 7 of the 12 patients, in whom data were available, were alive without evidence of recurrent leaks.
Discussion
This study demonstrates that fibrin glue injection is a feasible approach to acutely treat AL of various origins in patients with ESLD. There is a low procedure associated risk and we were successful in all patients. This technique does not attempt a final solution of the underlying problem, but allows assessment of the patient in terms of best therapy. By this, we were able to list 5 patients for LT. One had elective hernia repair after he improved clinically after the AL had been controlled. There was a contraindication for LT in 1 patient with advanced liver metastases from a colorectal carcinoma and in 7 patients who were active alcoholics or had contraindications for LT due to psychosocial or medical reasons. Although we showed an average improvement in MELD scores over 7 days in 14 patients, 6 patients had an actual improvement in MELD score, 4 patients had no change in MELD score, and 4 patients had worsened MELD scores (Fig. 1). Two of the patients with improved MELD scores and two of the patients with worsened MELD scores went on to liver transplantation. One patient was transplanted whose MELD score was unchanged over the monitored 7 days postinjection. As a result, our data suggest that AL control with fibrin glue does not significantly affect transplant candidacy but it does allow for medical stabilization as a bridge to transplantation. Accordingly, of the 9 patients who were not transplanted, 4 died during follow-up in association with their ESLD. However, in all of them the AL had been successfully managed. One patient underwent emergency repair for incarcerated hernia and died from intra-abdominal sepsis in association with an anastomotic leak.
The current treatment for persistent AL with ESLD particularly if associated with hernias is layered surgical repair after the ascites has been optimally managed5,10–12,18; however, surgical approaches convey a significant operative risk. 19 As a result, alternative modes of therapy such as temporary closure using fibrin glue injection may be considered. 16 For patients who are listed for LT, the strategy targets for improving the patients condition until LT during which the underlying problem (ESLD) is corrected and a hernia could be closed. For patients who are not listed, the injection allows for clinical improvement and assessment if the patient is eligible for LT. For patients, who are not eligible for LT, one should aim to improve the patients' condition and then repair a hernia in an elective procedure.15,20
By injecting fibrin glue to stem the drainage of ascites, we have confirmed a sound new approach to this problem, which was first described by Melcher et al. 16 The advantages of this approach are several. The risk of this technique is low because of the minimal amount of tissue manipulation required compared with a layered closure and because there is no need for general anesthesia. Further, the injection of tissue adhesives does not require the correction of the associated coagulopathy. Even though we had exclusion criteria regarding hugely aberrant coagulopathies, our patients had an average INR of 1.8 (range 1.4 to 2.8). We injected all of these patients with no complications and would argue that these injections are no more traumatic than subcutaneous heparin injections and as a result can occur at almost any coagulopathy level. We recommend that the absolute contraindication for fibrin glue injection in patients with AL is active infection at the injection site. Relative contraindications, as mentioned above, would be coagulopathies (INR>3.0) or thrombocytopenia (platelet count <20,000).
Most importantly, the technique does not preclude repeat fibrin glue injections or surgical intervention at a later time, should the initial injection fail. This approach could be particularly advantageous in temporizing the patient's leak so that the patient may be optimized for surgical intervention including LT at a later time (antibiotics, ascites drainage, etc). A large proportion of our referred patient population had leaking incisions after hernia repair and in all cases we were successful with our therapy. If such leaks persist, there is a high likelihood for infection and/or recurrence of the hernia.
In our patient population 5 patients required re-injection of the leaking site due to persistent leak. In 4 of these 5 patients, the leak site was an open hernia repair incision and 1 patient had laparoscopic port leak sites. This suggests that the larger the peritoneal defect (i.e., incision), the greater the area of leak and the more likely the need for another fibrin glue injection. Second, preinjection ascites tap volume seemed to influence the need for repeat injections. The average preinjection tapped ascites volume on these 5 patients was 390 mL (range 0–1500 mL) compared with 3111 mL (range 0–5000 mL) in the 9 patients not requiring repeat injections. As a result, our data suggest that the greater the volume of ascites tapped prefibrin glue injection, the less likely an AL will recur. The application of Dermabond® at the time of injection did not seem to influence the recurrence of leak as 3 of the 5 patients did not have Dermabond® applied.
Lastly, fibrin glue injection is a bedside/outpatient procedure that is considerably less costly than going to the operating room or medically managing these patients with prolonged hospital stays. It must be recognized, however, that the injection of tissue adhesives does not correct the fascial defect in ruptured hernias and so herniation of intestinal contents, incarceration, or strangulation may still occur at a later time point. Also, with every injection there is the potential for the introduction of pathogens into the wound, which could have significant effects especially in this patient population. Further, the injection of a substance superficially could apply pressure to overlying skin and potentially cause skin necrosis making the problem worse. These complications were not seen in our patient population.
Conclusion
AL in the setting of ESLD and ascites can have serious consequences. Surgical management of these patients is associated with a considerable perioperative mortality rate. We have shown that the injection of fibrin glue in these patients can immediately stop the drainage of ascites. This relatively safe, inexpensive, and easily performed procedure can delay surgical intervention and aid medical optimization of the patient. It can serve, ultimately, as a bridge to LT and/or definitive surgical repair. It may be beneficial to initiate a prospective trial comparing our technique to conventional approaches to determine the final value of the procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.