
Abstract
Abstract
We report a case of hepatoptosis in an 11-year-old boy with a longstanding history of intermittent abdominal pain, nausea, and flatulence. The diagnosis of hepatoptosis was established by upper gastrointestinal series, abdominal ultrasound, and contrast enema so that the working diagnosis of malrotation or situs inversus could be excluded. The patient underwent laparoscopic hepatopexy with fixation of the ligamentum falciforme hepatis to the right diaphragm and fixation of the ligamentum teres hepatis with the distal part of the ligamentum falciforme hepatis to the anterior abdominal wall. We describe a new operative procedure for hepatoptosis and focus on this rare disease.
Introduction
On the other hand, there are reports on congenital cases with absence of the coronary and suspensory ligaments. 2
The symptoms of hepatoptosis are variable. They include dyspeptic symptoms, abdominal pain, nausea, dyspnoea, flatulence, constipation, and jaundice.1,2 However, some patients do not have any symptoms. As all symptoms are rather nonspecific, diagnosis is not easy. 2
Case Report
An 11-year-old boy presented to our outpatient department with recurrent abdominal pain and constipation. Symptoms and complaints were longstanding and had been present for nearly 3 years. He was referred from an external hospital with suspicion for malrotation or situs inversus. For further investigation, an upper gastrointestinal study, a barium enema, and an ultrasound of the abdomen were performed. There were no signs for malrotation, but the ultrasound demonstrated abnormally located bowel loops in the right upper abdomen and the liver located in the midline. The spleen was in normal position. Therefore, the diagnosis of floating liver was made.
Because of persistent symptoms, correlating with the ultrasound findings, we saw an indication for operative treatment. To minimize abdominal trauma, we decided to perform a laparoscopic procedure.
Laparoscopic hepatopexy was performed via a typical subumbilical incision and a 10-mm trocar was inserted for introduction of a 30° angular optic (Fig. 1). Two more 5-mm working trocars were inserted in the right and left upper abdomen. The falciforme ligament was fixed to the right portion of the diaphragm by three 2-0 Ethibond sutures (Fig. 2). Then, a percutaneous puncture of the abdominal wall with an Ethibond 0-0 suture was done to fix the distal falciforme ligament and the ligamentum teres hepatis to the abdominal wall (Fig. 3). Afterward, the knot was buried under the skin. Further, we revised the small intestine to exclude malrotation.
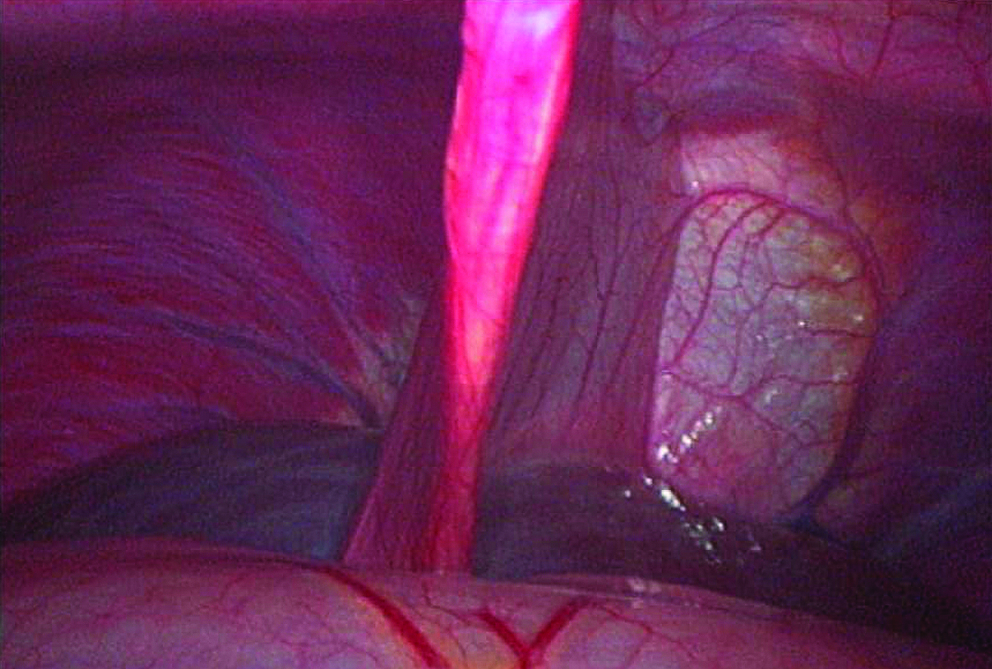
Preoperative situation.
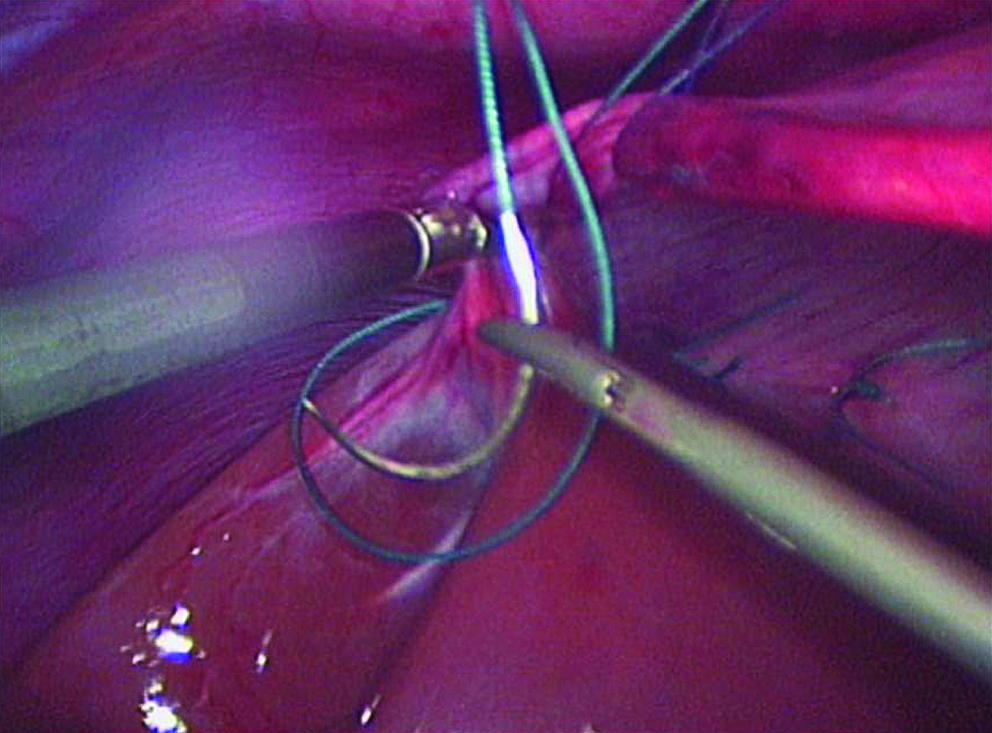
Fixation of the liver to the abdominal wall.
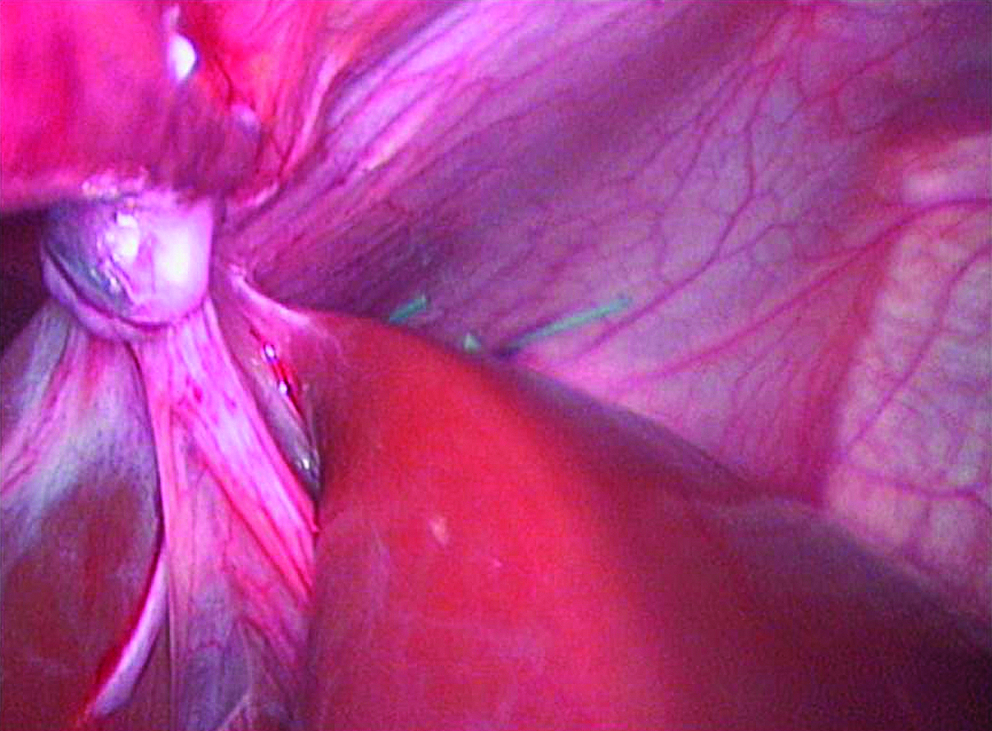
Postoperative situation.
The postoperative course was uneventful. The ultrasound check-up after 3 and 12 months demonstrated the liver in a normal midline position. The patient had no complaints of abdominal pain.
Discussion
The first case of hepatoptosis was described in 1754 by Heister. 3 At autopsy he found a displaced liver lying sagittally in the right upper abdomen with its convex surface in contact with the serosa of the right abdominal wall. This patient had symptoms of flatulence and abdominal fullness. 3
The entity of hepatoptosis has to be distinguished from Chilaiditi syndrome and enteroptosis caused by severe weight loss.4,5 Chilaiditi syndrome is an interposition of bowel between liver and diaphragm, usually the transverse colon or hepatic flexure. There are single reports about interposed small bowel. Most patients suffering from Chilaiditi syndrome are asymptomatic. Some nonspecific symptoms include abdominal pain, bloating, and constipation. 6 The entity of Chilaiditi syndrome, however, remains unclear. 7
Treatment for hepatoptosis consists of conservative therapy and several different operations. For conservative treatment, special bandages were used to sustain the displaced organ; however, the patient feels very uncomfortable. Further, there was an attempt to use tonics or hydrotherapy. With regard to these adjuvant therapeutic options, electricity was used as an additional treatment to increase the muscle tone of the abdomen. 2 However, we regard these measures as historic.
When conservative treatment failed, generally hepatopexy was performed. There have been several open approaches for hepatopexy.1,8 The first hepatopexy was performed by Michl in 1887. 8 Different approaches included ventrofixation of the liver with sutures through the right costal cartilage or suturing of the peritoneum to the anterior border of the liver. 1 Alternatively, scarification was done to the liver surface to achieve sufficient adhesions between the diaphragm and the liver.
The approach of Depage, the so-called laparectomy, included a resection of portions of the abdominal wall transversally as well as vertically to gain a reposition of the liver. 9
Péan reported a different approach in 1896. 10 He constructed a new space for the liver in the abdominal cavity by using parts of the transverse abdominal muscle and fixing the muscle parts to the posterior abdominal wall. 2
A review from 1924 described the ligamentum teres hepatis as the essential support for the replacement of the liver. 4
In concordance with their observations, we also used the ligamentum teres hepatis as an important structure for ventral fixation of the liver. But, in contrast to their report, we used a laparoscopic approach with a more extended fixation of the liver. Therefore, this is the first report of laparoscopic hepatopexy.
In our solitary case, the laparoscopic procedure was safe and effective for treatment of hepatoptosis. Further operations in other patients have to be carried out to confirm this new and safe procedure. However, it is a problem to acquire a patient collection large enough for significant results because, as mentioned earlier, hepatoptosis is a rare entity.
Footnotes
Disclosure Statement
No competing financial interests exist.