
Abstract
Abstract
Recent reports on the feasibility and safety of single-incision cholecystectomy have challenged the conventional multiport access to the gallbladder. Nevertheless, the proximity of different instruments and the laparoscope may lead to interference that potentially compromises the safety of the operation. This article describes the use of a customary flexible restraint system for the gallbladder fundus to achieve triangulation by means of a three-instrument technique and an optimized view to the Calot's triangle.
Introduction
We describe a new technique of independent fundal retraction of the gallbladder using a thin and space-saving customary restraint system.
Operative Technique
The articulated restraint system (DB2C; Chirurgical Concept, Mery-sur-Cher, France) and its connection to the left side of the operation table are shown in Figure 1. The retractor is rigid at its back end, and at its front end it is tridimensionally flexible and lockable in any position. The connection of the retractor to a straight 3-mm grasper used for gallbladder fundal retraction is shown in Figure 2.

Restraint system (DB2C; Chirurgical Concept) for gallbladder fundus retraction, fixed to the left side of the operation table.
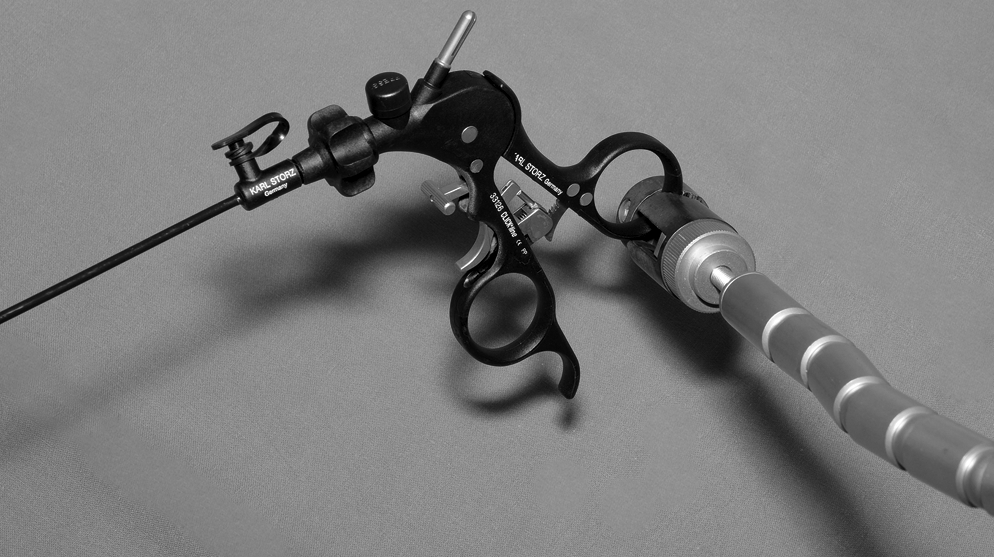
Connection of the restraint system to the hand grip of the 3-mm grasper.
Single-port access cholecystectomy is performed using the re-usable X-Cone Single-Port Laparoscopic Device (X-Cone™; Karl Storz GmbH, Tuttlingen, Germany) (Fig. 3). This metal device is composed of two tapered L-shaped half shells (one with an insufflation tap) and sealed with a silicone rubber cap. After a 20-mm vertical skin incision in the umbilicus, via an open approach, the port is trocar-like placed into the abdominal cavity, creating an autostatic X-shaped funnel. For sealing, a rubber cap offering five gas-proof working channels is applied. One of the five working channels permits the introduction of instruments up to 12.5 mm. A 50-cm-long, 30°, 5-mm laparoscopic camera (Karl Storz) is introduced via the right working channel. After the gallbladder is identified, attention is directed to the gallbladder fundus, which is retracted upward using a straight 3-mm grasper inserted via the lowest working channel. This technique is comparable to fundal exposition known from standard multiport cholecystectomy. For a static fundal retraction, the hand grip of the grasper is then connected to the flexible retractor and the retractor is locked in this position (Fig. 4). For infundibular manipulation, a curved roticulating grasper (Karl Storz) is used, placed via the left working channel. Independent fundal retraction combined with the roticulating function of the curved (infundibular) grasper enables perpendicular distraction of the cystic duct from the common bile duct and an optimal exposition of the anterior and dorsolateral view to the Calot's triangle (Figs. 5 and 6). For dissection and isolation of the cystic duct and the cystic artery, a 5-mm scissors (Karl Storz) is used. The cystic duct and the cystic artery are doubly clipped using a 10-mm clip applicator (Challenger Ti™; Aesculap AG, Tuttlingen, Germany) inserted via the middle working channel, and then transected. During these procedures the fundus is statically retracted with the 3-mm grasper. Besides optimal exposure, this technique offers maximum range of motion for the additionally inserted instruments, minimizing extracorporeal conflicts of the hands. Further, the assistant can use both hands for optimal camera work, including radial work with the light cord (Fig. 7). For dissection of the gallbladder from the liver bed, the restraint system may be removed and the 3-mm grasper managed by the surgical assistant. After complete dissection, the gallbladder is placed in an endobag (Inzii™; Applied Medical, Rancho Santa Margarita, CA) and removed at the port site. The fascial defect at the umbilicus is then closed using interrupted absorbable sutures (Vicryl 0; Ethicon GmbH, Norderstedt, Germany), and the skin incision is closed with a 4-0 absorbable subcuticular suture.
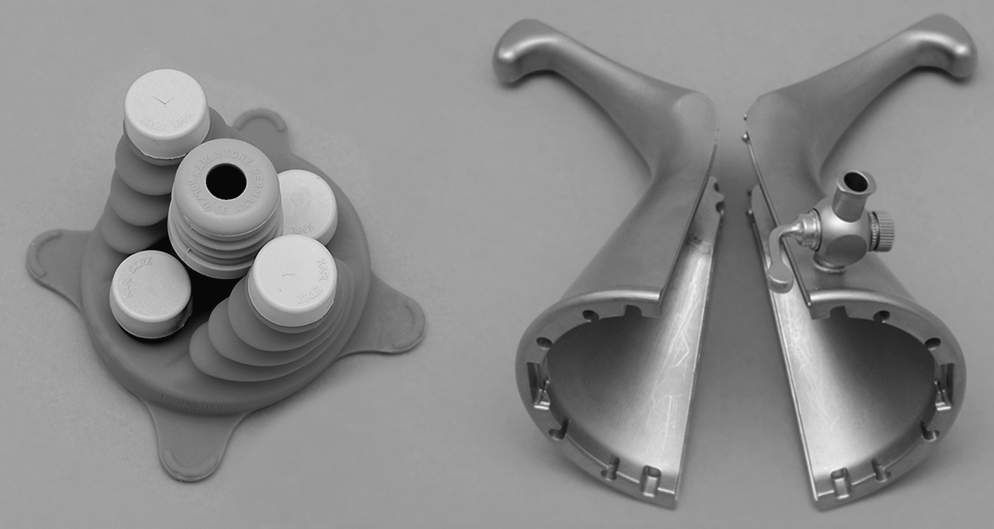
Reusable X-Cone™ Single-Port Laparoscopic Device (Karl Storz).

Three-millimeter grasper, inserted via the lowest working channel, connected to the restraint system for static gallbladder fundus retraction.
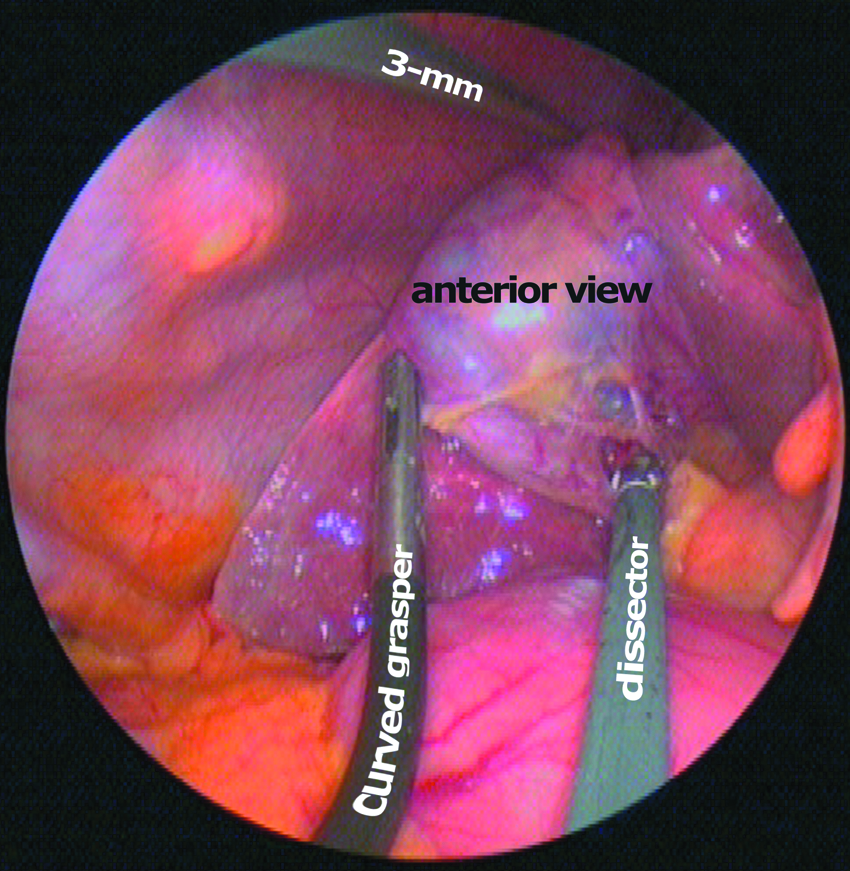
Exposition of the gallbladder infundibulum in a three-instrument technique (anterior view).

Exposition of the gallbladder infundibulum in a three-instrument technique (dorsolateral view).
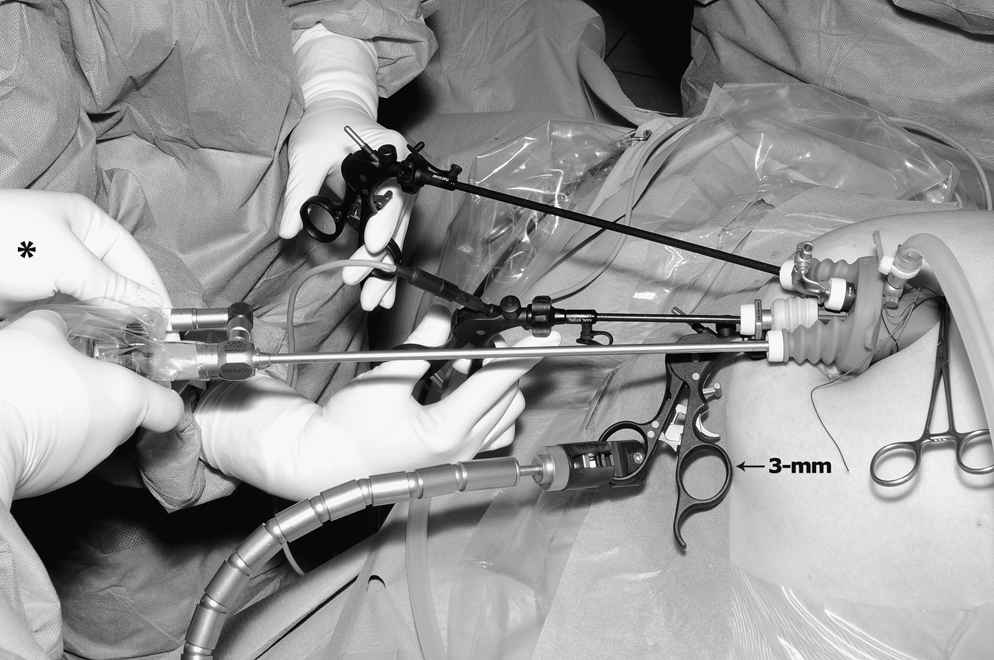
Optimal extracorporeal range of motion for the applied instruments. The assistant can use the free left hand (*) for radial work with the light cord.
Discussion
With the development of single-port cholecystectomy as a less invasive access to the gallbladder, surgeons were forced to become familiar with in-line viewing and a limited ability of triangulation, both resulting in a potentially compromised view to critical structures in the Calot's triangle. Given the different techniques that have evolved in single-port surgery (with versus those without an access device), the use of an access device itself may limit the range of instrument motion, as all instruments need to be passed through the “bottleneck” of the port. Using the X-Cone, we experienced that this drawback (of any access device) is outweighed by the stable instrument guidance and the gas-tight sealing.
In a recent report, Podolsky and Curcillo clearly demonstrated the superiority of a three-instrument technique in achieving and maintaining an optimal exposure of the hepatocystic triangle, when compared with 2-instrument use. 4 However, increasing the number of instruments inserted via a single incision (in the umbilicus) again confines the ability of unhindered instrument motion. This problem may even increase when using an access device, as mentioned above. Consequently, attempts have been made to avoid collision of instruments (and the laparoscope) while achieving the best operative exposure, including instruments of different lengths, articulated instruments, flexible-tip cameras, transperitoneal sutures, or magnetic aid.5,6 Nevertheless, some of the reported techniques 6 raise concerns regarding bile spillage. 7
The use of a thin, lockable retraction system for the gallbladder fundus enables (1) good triangulation by means of a three-instrument technique, (2) an increased range of instrument motion for the surgeon by eliminating one of the assistants' hands from the limited area of the external instrument handles, and (3) superior camera work afforded by use of both of the assistant's hands. A safe anterior and dorsolateral view of the hepatocystic triangle was achieved by the roticulating function of the curved grasper. Further, we were able to largely use customary equipment for conventional multiport cholecystectomy. The re-usability of the retractor and its connectability to the hand grip of a standard 3-mm grasper do not increase costs of the procedure. Finally, the restraint system introduced here is not prerequisite when using the X-Cone device but has emerged as a practical additional tool in recent single-port cholecystectomies performed by our group. We anticipate that this might also apply for other single-port access techniques.
Footnotes
Acknowledgment
We thank A. Kellersmann and H. Bergauer for technical assistance with the graphical material.
Disclosure Statement
K. Krajinovic and C.-T. Germer received travel grants from Karl Storz. For J. Reibetanz and A. Wierlemann, no competing financial interests exist.