
Abstract
Abstract
Background:
Component separation technique (CST) enables rectus abdominus medialization, but may cause wound complications. Few published outcomes exist involving laparoscopic CST. Our aim was to examine feasibility and outcomes involving open and laparoscopic (lap) CST during ventral incisional hernia repair (VIHR) and present an algorithm for ventral herniorrhaphy.
Study Design:
Our design was a retrospective cohort study. Over 22 months, 28 patients underwent one of the following: (i) unilateral (U-) lap CST with open VIHR [n=5], (ii) bilateral (B-) lap CST with open VIHR [n=7], (iii) B-lap CST with lap VIHR [n=8], or (iv) B-open CST with open VIHR [n=8]. Indications for open VIHR included mesh removal, concomitant visceral procedure, wound revision, thin/ulcerated skin, abdominal wall tumor, frozen abdomen, and/or off-midline hernia. During open VIHR, CST was performed in the Ramirez fashion. Lap CST was performed before intraperitoneal access in lap VIHR and after retrorectus dissection in open VIHR. Patient surveillance consisted of clinical encounters and telephone interviews.
Results:
Groups were similar regarding age, body mass index, American Society of Anesthesiologists classification, hernia width, operative time, and hospital stay. Six of the 20 patients who underwent open VIHR developed wound complications, and two required early reoperation. Four of the six with concomitant visceral procedures had wound complications. No laparoscopic VIHR patients had a wound complication. Based on 11 months' follow-up, one open VIHR patient has concern for recurrence.
Conclusions:
Laparoscopic CST is feasible during open and laparoscopic VIHR, but it appears most beneficial for wound healing after laparoscopic VIHR. During open VIHR, laparoscopic CST may not substantially reduce wound complications.
Introduction
In patients with wide rectus muscle separation, a lap repair creates an adynamic central zone that may result in mesh eventration and a persistently dysfunctional abdominal wall. Van Sickle and colleagues 4 determined that rectus diasthasis worsens in 8% of patients with large midline hernias after lap VIHR using a standard intraperitoneal mesh technique. Laparoscopic approximation of the rectus fascia before intraperitoneal mesh placement has been reported with excellent results by Franklin, 5 but this technique is not feasible in patients with large defects. In patients with large defects and loss of domain, there is often insufficient abdominal wall in which to secure an intraperitoneal mesh. Thus, standard laparoscopic VIHR is not a functionally restorative operation in such patients and has a higher recurrence rate.
Open separation of components, as championed by Ramirez, 6 has enabled rectus muscle medialization in patients with midline defects up to 20 cm in size. Reports of this technique have revealed overall hernia recurrence rates ranging from 0% to 53%, although better results are seen with mesh reinforcement, and overall wound complication rates range between 10% and 53%.7–11 When Gonzalez and colleagues 7 compared open component separation technique (CST) with standard laparoscopic VIHR using permanent mesh, laparoscopy compares favorably due to reduction in wound complications. It is believed that creation of the lateral skin flaps in open CST greatly increases the rate of wound complication, and can result in catastrophic skin necrosis when perforator vessels are not meticulously spared. Biological meshes have been designed to address those patients in need of mesh reinforcement, but who have high risk of wound complications.
More recently, the CST has been performed laparoscopically. Potential benefits of the laparoscopic CST over an open approach include decreased wound complications and easier avoidance of perforating blood vessels. The laparoscopic CST has shown promise in both a porcine model and a human cadaver model. 12 There are few existing reports of patient outcomes after open VIHR with laparoscopic CST, but analysis of these reveals an overall wound complication rate of about 25%.13–15 From our institution, we recently reported a case series of four patients who had laparoscopic CST employed with laparoscopic VIHR, without hernia recurrence or wound complication. 16
With multiple methods of VIHR available, the question may not be which technique is better. Rather, we might ask which technique is more appropriate for a given clinical scenario. Therefore, our aim is to examine the feasibility and outcomes involving both open and laparoscopic (lap) CST during both open and lap VIHR. After reviewing the data, we planned to identify clinical decision points to create an algorithm that might help surgeons individualize the management for each patient with a large symptomatic midline ventral hernia.
Materials and Methods
Our design is a retrospective cohort study approved by the authors' institutional review board (09-006304), with data obtained from a single tertiary-care referral center. Between July 2008 and April 2010, 28 patients underwent one of four procedures: (i) unilateral (U-) lap CST with open VIHR, (ii) bilateral (B-) lap CST with open VIHR, (iii) B-lap CST with lap VIHR, or (iv) B-open CST with open VIHR. CST was chosen for large midline hernias with functional impairment.
Procedures and indications
Lap CST utilizes two trocars per side, and begins with separation of the external and internal oblique muscles, with subsequent deployment of a structural balloon. The lateral intramuscular space is developed sharply from the inguinal ligament to well above the costal margin, and the external oblique fascia is incised lateral to the semilunar line. This approach is designed to preserve all perforating blood vessels. A thorough description of our technique used in lap CST with lap VIHR has been described previously. 16
Lap CST was performed before intraperitoneal access in lap VIHR, and we explain preoperatively that the redundant overlying skin is not resected and instead is allowed to remodel over time. Lap CST was performed after the adhesiolysis and development of the retrorectus space in open VIHR. In open VIHR, we first perform adhesiolysis and hernia reduction, followed by development of the retrorectus space through release of the posterior rectus fascia. At this point, we assess the need for component separation. If component separation is needed and feasible laparoscopically, then we proceed with lap CST. All 20 patients with lap CST had their midline fascia reapproximated. Indications for open VIHR included presence of thin or ulcerated skin or need for wound revision (n=7), need for a concomitant visceral procedure (i.e., gastrointestinal or genitourinary) (n=6), need for mesh excision only (n=3), presence of a “frozen abdomen” (n=2), presence of an abdominal wall tumor (n=1), and presence of an off-midline hernia (n=1). Concomitant visceral procedures were planned and included two patients with small bowel resections, one patient with ileocolic resection and end ileostomy, one patient with unilateral salpingo-oophorectomy, one patient with sleeve gastrectomy, and one patient with sleeve gastrectomy and transposition of ileal conduit. There were no inadvertent enterotomies.
Open CST was utilized in patients who had hernia sac extending laterally beyond the semilunar line based on physical exam or CT scan, and it was used in patients who required extensive skin mobilization for skin ulceration. Open CST was performed in the fashion of Ramirez, with every effort made to preserve dominant periumbilical perforator vessels coursing from the anterior rectus fascia to the skin. The retromuscular space was preferentially used for lightweight or midweight polypropylene mesh placement, whereas composite polyester mesh was preferentially used during intraperitoneal placement. The midline was reapproximated in six of eight patients who had an open CST with open VIHR, whereas the other two were bridged and left with 4 and 8 cm defects, respectively, to avoid tension. Unilateral CST was performed when contralateral rectus muscle atrophy or extensive contralateral scars were present.
Patient factors
We reviewed the operative log at our institution and identified 28 patients who had a CST procedure during VIHR. From their medical records, we gathered demographic data, including age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) classification, and width of hernia defect based on preoperative CT imaging or intraoperative measurement, if CT scan was not performed.
Outcomes variables
The operative records for all procedures were reviewed to determine the type of VIHR performed, estimated blood loss (EBL), operative time, type of mesh used, and concomitant procedures. In addition, the postoperative records were reviewed to determine the quantity of blood transfused, LOS, and symptoms present at the time of all postoperative follow-ups. Finally, patients without follow-up in 2010 were contacted by telephone to address their current conditions. Patients with concern for hernia were offered clinical appointments for a physical examination.
The primary outcome was immediate postoperative wound complication, as defined by those wounds that develop a hematoma requiring transfusion, or an abscess or fluid collection requiring any intervention within 30 days. Postoperative pain or seromas not requiring drainage were not considered wound complications. Secondary outcomes were EBL, operative time, number of units of blood transfused during hospitalization, LOS, and 30-day readmission. For those patients with >30 days of follow-up, secondary outcomes included length of follow-up, hernia recurrence, required mesh explantation, and presence of abdominal wall complaints. Our final secondary outcome was to develop an algorithm to help determine which operative approach may be selected for each patient with a large VIH.
Statistical analysis
For continuous variables, including age, BMI, width of hernia defect, operative time, EBL, LOS, and length of follow-up, analysis of variance was used to analyze differences among the four groups. For ordinal data, as with the number of units of blood transfused, the number of patients requiring readmission within 30 days, and the number of patients with wound complications, a chi-square test was performed. A chi-square test was also performed for categorical data, including ASA score. For dichotomous variables, including gender, logistic regression was used to analyze difference between the four groups. Percentages are given for those patients with hernia recurrence, required mesh explantation, and/or presence of abdominal wall complaints. Statistical analysis was performed using Statistical Analysis System software (Version 9.1.3) and OpenEpi (Version 2.3), with P<.05 considered statistically significant.
Results
Patient demographics
As demonstrated in Table 1, the patients in each exposure group were similar with regard to age, gender, BMI, and ASA classification. With regard to the width of hernia defect, the average size within groups ranged from 10.2 to 14.3 cm, with no significant differences among groups.
Values are expressed as mean.
U, unilateral; B, bilateral; CST, component separation technique; VIHR, ventral incisional hernia repair; Lap, laparoscopic; BMI, body mass index; ASA, American Society of Anesthesiologists classification; NS, not significant.
Type of mesh
Table 2 demonstrates the type of mesh used, if any, during herniorrhaphy. For those patients who underwent open VIHR, the retromuscular space was used for lightweight or midweight polypropylene mesh placement in 14 patients, and intraperitoneal composite polyester was used in an additional four patients. Finally, intraperitoneal biological mesh was used in one patient, and one patient underwent primary fascial closure without mesh. In the group of patients who had a lap CST with lap VIHR, six had a composite polyester mesh placed and two had polytetrafluoroethylene placed.
PTFE, polytetrafluoroethylene.
Primary and secondary outcomes
As demonstrated in Table 3, no difference between groups was seen regarding operative time, EBL, LOS, or transfusion requirement. However, we noted some difference in operative times between patients who had a concomitant visceral procedure and those that did not (4.66 versus 3.81 hours, respectively). Overall, there were two 30-day readmissions and six (early and late) wound complications. Wound complications consisted of one hemorrhage requiring transfusion, one wound infection requiring surgical debridement, one infected seroma requiring drainage, one recurrent Crohn's-related enteric fistula requiring reoperation, and two late seroma infections (at greater than 2 months follow-up) requiring debridement and negative pressure wound therapy. None of these patients required mesh explantation, as the exposed mesh beneath the anterior rectus dehiscence granulated in after negative pressure therapy. Of these six patients with wound complications, four had a concomitant visceral operation. The rate of wound complications in patients undergoing visceral operation was 67% (four of six). None of the eight patients repaired by a combined lap CST and lap VIHR had a wound complication.
Values are expressed as mean.
EBL, estimated blood loss; LOS, length of stay.
Regarding our long-term follow-up, all patients have been recently examined or contacted by telephone; however, our data are based on 23 patients who underwent at least one physical examination at greater than 30 days after herniorrhaphy. For those patients, the mean and median lengths of follow-up (by telephone or in person) are 10.7 and 11.2 months, respectively, with a range of 1.6–21.2 months. Only one of these patients (4.3%) has a concern for recurrence. This patient required negative pressure therapy to the periumbilical aspect of the wound to granulate the lightweight polypropylene mesh, and by telephone states that he has an asymptomatic bulge at this site. In addition, three patients (13%) have had abdominal wall complaints related to transfixation suture sites, three patients (13%) had a diasthasis or bulge of the abdominal wall distant from the hernia repair, and five patients (22%) had an abdominal wall pulling sensation or other discomfort. Further, one patient (4.3%) repaired by a lap CST and lap VIHR underwent laparotomy for a perforated ulcer at 12 months with a primary fascial closure and polytetrafluoroethylene mesh excision. Finally, we developed an algorithm for the optimal use of the lap CST for myofascial advancement during VIHR, as shown in Figure 1.
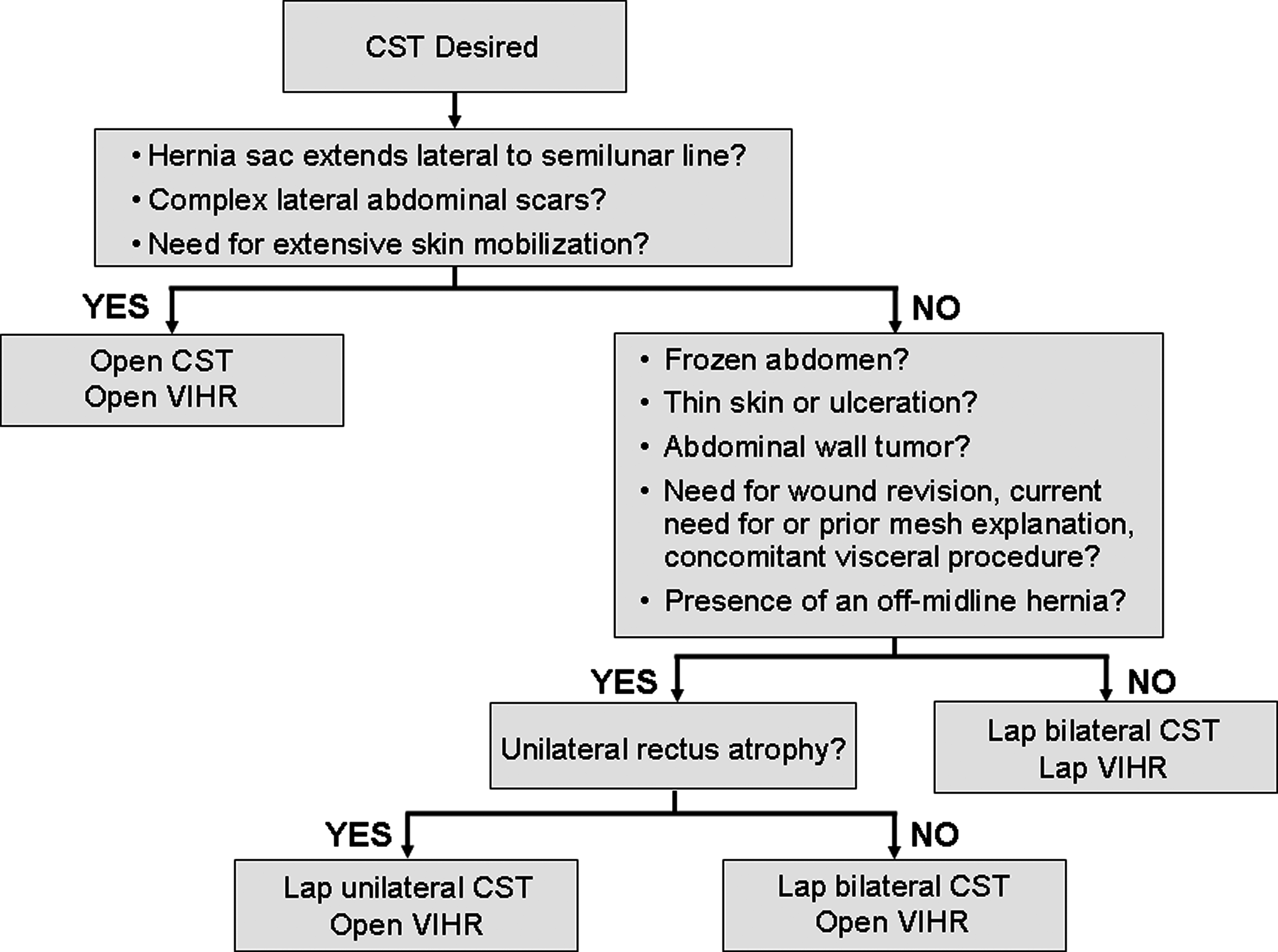
Suggested algorithm for deciding the optimal approach to component separation technique (CST) during ventral herniorrhaphy.
Discussion
Although we have demonstrated the feasibility of the laparoscopic CST during laparoscopic VIHR based on eight patients, we have been equally critical in determining the potential benefit, if any, in performing a laparoscopic CST during an open VIHR. The laparoscopic CST has been performed during open VIHR and reported in small case series. In previously reported cases, the majority of patients had herniorrhaphy performed under contaminated conditions, and it was therefore not surprising that no series was free of complications or recurrences.13–15 Similarly, our results demonstrate six wound complications among the 20 patients who underwent open VIHR. More specifically, four of the six wound complications occurred after lap CST. However, four of the six patients with wound complications had a concomitant visceral procedure, and all early postoperative infectious complications occurred in this group of patients. Patients undergoing lap CST and lap VIHR were at lower risk of infectious complications, and all had uncomplicated recovery.
Unfortunately, the only metrics available for measuring success in hernia repair are perioperative complications and presence of recurrence at late follow-up. There are no valid metrics that can be currently used to measure improvement in abdominal wall function. Patients with large midline hernia defects are generally not at risk of incarceration, but have complaints related to the appearance of the hernia and the effect of rectus muscle separation on abdominal wall function. The authors believe that medialization of the rectus muscles in these patients is imperative to improving abdominal wall function. Further, the CST with myofascial advancement increases the abdominal wall circumference, to enlarge the intraperitoneal space in those patients afflicted with a loss of domain. Finally, the rectus medialization that follows the CST potentially diminishes the risk of subsequent mesh eventration.
It is unclear whether or not the sacrifice of the external oblique muscle function is justified for the purpose of rectus muscle medialization. One might argue, however, that there would be fewer and less severe wound complications if the rectus muscles are approximated above the prosthetic mesh. It is for this reason that the authors favor a lightweight or midweight polypropylene mesh placed as an underlay in the retromuscular space, as in the technique of Rieves and Stoppa. This is not always possible, as when there is an off-midline component of the hernia. The authors believe that a mesh separated from the viscera by the posterior fascia and peritoneum would granulate under negative pressure wound therapy, should that type of therapy become necessary. This is ideal in the face of wound infection, and our experience bears this out. When mesh is placed in the intraperitoneal position, the authors use polyester covered by an anti-adhesion barrier, although the ability to reliably salvage this type of mesh within a deep wound infection remains to be seen.
Regarding the use of a unilateral CST, the authors believe that CST should be added to the operation to improve the functional aspect of the abdominal wall. In the case of an atrophic rectus muscle due to extended Kocher or Chevron type incision, the authors feel that the oblique muscle integrity may provide more abdominal functionality than the atrophic rectus, and we are unlikely to sacrifice the oblique muscle unless absolutely necessary for wound coverage.
The choice between an open CST and a lap CST involves not only the approach to herniorrhaphy, but also the size of the hernia defect. The lap CST can provide rectus advancement similar to an open CST, as reported by Rosen, 17 but the development of the retrorectus space, during posterior rectus fascial release, broadens the rectus muscle to enable effective closure of wider defects. Therefore, in a patient with adequate preoperative weight loss and broad, mobile rectus muscles as demonstrated on CT scan, some large defects can be closed with a combined lap CST and lap VIHR. However, the midline approximation will be under some tension, requiring a large piece of intraperitoneal buttress mesh, and most patients would not be candidates for this approach. Otherwise, the surgeon should consider an open VIHR with development of the retrorectus space followed by the lap CST, to allow even greater rectus release and improved medial reach of the midline fascia.
We recognize certain limitations in our report. Our data are retrospective and is limited by our dependence upon patient reporting as a primary means of outcomes assessment. Although we have some data collected from actual follow-up patient examinations, we did utilize data based on telephone encounters without a physical examination. We recognize that it is difficult to determine if anatomic and/or functional problems exist, during telephone conversation, especially in determining recurrence. Nonetheless, based on our telephone follow-up, it appears that 1 of the 12 patients with lap CST and open VIHR may have recurrence, possibly due to degradation of the lightweight polypropylene mesh in attempts to salvage it with negative pressure therapy. Although the patient had a postoperative wound complication, the patient is asymptomatic. We believe that none of the patients who have had a lap CST and lap VIHR has recurred at this time. Further, we believe that none of the eight patients who have had open CST and open VIHR has recurred at this time, although our length of follow-up is somewhat less than the other groups. It is our experience that patients have similar degrees of late postoperative abdominal wall complaints regardless of approach, but that patient satisfaction with successful functional repair is subjectively quite good.
In addition, we are limited by both the small size (n<10) and heterogeneity of the groups. The small size of our groups makes it difficult to state with any certainty that one approach is superior to another. Specifically, among 20 patients who underwent open VIHR, there were 6 patients (two per group) who had a concomitant visceral procedure, whereas no combination lap CST and lap VIHR patients had concomitant visceral procedures. As expected, our operative times are higher in patients with concomitant visceral procedures than in those without concomitant procedures (4.67 versus 3.81 hours, P<.05). The increased operative time is likely attributed to the extensive lysis of adhesions and/or concomitant visceral procedures.
The body of research surrounding the CST demonstrates no definitive standard for the operative approach or the choice of fascial incisions. Fortunately, our outcomes helped us to identify useful decision points that allowed us to create an algorithm that might help surgeons individualize the ideal procedure to treat each patient with a symptomatic midline ventral hernia. Figure 1 proposes an algorithm for this preoperative decision-making process. If a patient has a hernia sac lateral to the semilunar line or a need for extensive skin mobilization, an open CST with open VIHR is recommended. This is advantageous, despite the fact that extensive skin mobilization may necessitate sacrifice of one or more perforator vessels, and this has been shown to correlate with a 10-fold increased risk of wound complications. 18 Because the CST must be performed initially in the combined lap CST and lap VIHR, there is a theoretical risk of visceral injury in patients with hernia sac lateral to the semilunar line. In these patients, excision of the sac would provide sufficient exposure to perform the external oblique release, and the laparoscopic approach is likely not beneficial. Similarly, if the patient has a lateral abdominal scar that is complex or has healed secondarily, then an ipsilateral open CST is advisable. Otherwise, the lap CST is feasible and performed bilaterally if there is no sign of rectus atrophy, and is combined with a lap VIHR in the advantageous abdomen. In addition, a lap CST can be done with an open VIHR if there is evidence of skin ulceration, dense intraperitoneal adhesions, an abdominal wall tumor, or an off-midline hernia. An open VIHR also suits those patients who require wound revision, mesh explanation, or a concomitant visceral procedure. Therefore, in patients who require an open approach to VIHR, the laparoscopic CST remains feasible. Although the lap CST may not offer a substantial improvement in wound complications when compared with an open CST, it appears justified by the reduced theoretical risk of catastrophic skin necrosis.
Footnotes
Disclosure Statement
No competing financial interests exist.