
Abstract
Abstract
Multiple hereditary exostoses is a rare autosomal dominant disorder characterized by the growth of multiple osteochondromas. We describe the thoracoscopic remodeling of a spiculated costal exostotic lesion responsible for spontaneous recurrent hemothoraces in a 17-year-old male patient with multiple hereditary exostoses.
Introduction
Case Report
A 17-year-old male patient with a known diagnosis of MHE, status post–multiple resections of upper and lower extremities osteochondromas over the last 7–8 years, presented to the emergency department with an acute onset of pleuritic chest pain. On physical examination, he was afebrile and had no acute distress. Vitals signs included a heart rate of 89 beats per minute, blood pressure of 124/77, and a respiratory rate of 24 breaths per minute. His oxygen saturation was 100% on room air by pulse oximetry. Decreased breath sounds of the left hemithorax were noted upon auscultation. Multiple exostotic growths were noted on his upper and lower extremities, anterior and lateral ribs, and scapula. Laboratory studies were notable for a hematocrit level of 37.8%. A chest X-ray (Fig. 1) followed by a chest computed tomography scan (Fig. 2) revealed the presence of a 7×7×10 cm3 posterior left pleural effusion consistent with hemothorax. The patient was admitted for observation. A decrease in hematocrit level to 31% in association with mild tachycardia (90–100 beats per minute) and a chest X-ray showing persistence of the hemothorax necessitated a diagnostic video-assisted thoracoscopy and further evacuation of the hemothorax. After induction of general anesthesia, the left main stem bronchus was occluded using a double lumen endotracheal tube, and the patient was positioned in the right lateral decubitus position. Five-millimeter ports were placed in the left 6th intercostal space at the midaxillary line and in the 5th intercostal space anterolaterally. Care was taken to avoid port placement in the proximity of any palpable exostotic rib lesion. During the procedure, several exostotic lesions were noted to protrude into the pleural space. There was no visible injury to lung parenchyma or visceral pleura and no sites of active bleeding, although >200 cubic centimeters (cc) of old blood and clot was evacuated. None of the exostotic lesions was removed. A 20F chest tube was placed under direct visualization. The patient did well postoperatively, with no evidence of further bleeding. The chest tube was removed on postoperative day 2, and the patient was discharged home on postoperative day 2 in stable condition.

Chest X-ray showing left-sided hemothorax.

Chest computed tomography image depicting rib exostosis and hemothorax.
Four days following discharge, the patient returned to the emergency department complaining of an acute onset of similar pleuritic chest pain. He was afebrile and his vital signs included a heart rate of 91 beats per minute, blood pressure of 99/70, and a respiratory rate of 16 breaths per minute. His oxygen saturation was measured at 97% on room air. Auscultation showed decreased breath sounds over the left lower lung field. The hematocrit level was 31.5%. A chest X-ray revealed a new moderate left basilar pleural effusion. The patient was taken to the OR for thoracoscopy using the former port sites, and 450 cc of blood and clot was evacuated. Although the lung tissue itself appeared intact, the previous exostotic costal lesions were again identified; one of these lesions was noted to be particularly spiculated and suspicious as the causative source of the bleeding (Fig. 3). The spiculated lesion was therefore remodeled (shaved flat with the underlying rib) using a 5-mm arthroscopic burr (Styker, Kalamazoo, MI), which was introduced through a third port site in the posterior axillary line, 5th intercostal space. Hemostasis was achieved with electrocautery. A 20F chest tube was again placed. Low-wall suction was continued for 4 days until complete resolution of the hemothorax. The chest tube was removed on postoperative day 6, and the patient was discharged home in stable condition. After 3 months of follow-up, there was no evidence of any residual or recurrent hemothorax.
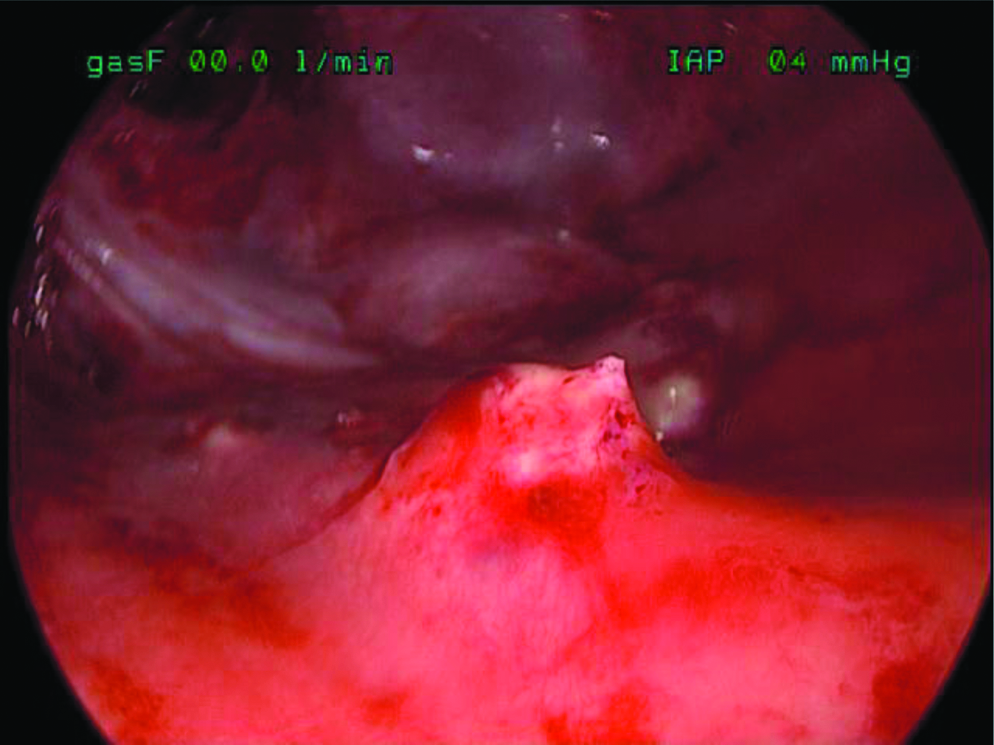
Intraoperative finding of a spiculated rib exostotic lesion.
Discussion
Osteochondromas are the most common pediatric bone tumors. These benign tumors are usually solitary and grow by endochondral ossification. Although they are typically located at the periphery of the growth plate of long bones, they have been reported to exist in a variety of other locations. 1 MHE is an autosomal dominant disorder of variable penetrance caused by a mutation in the tumor suppressor gene EXT1 or EXT2, wherein patients develop multiple osteochondromas during childhood and adolescence. 2 These lesions typically cease to grow by adulthood. For unknown reasons, males are more often affected than females. Although often asymptomatic, these tumors can cause angular deformities, impinge on joints, and damage underlying soft tissues. An estimated 75% of patients have clinically obvious deformities, most commonly of the forearm. 3 Soft tissue injury is much less common, although there are case reports that describe spinal cord compression by exostoses, and it has been estimated that 7%–9% of MHE patients are at risk for spinal cord compression by vertebral exostotic lesions. 4 Bleeding is a rare but serious risk in patients with osteochondromas. Damage is thought to occur when the cartilaginous cap of the tumor begins to reabsorb during ossification, exposing the new underlying sharp bone. 5 In a review in 1999 of 97 cases of exostosis with bleeding complications, only 3 of the described cases reported costal involvement, as in our patient. 5 Similar thoracic trauma has also been reported by other authors: we reviewed 14 English-language case reports of hemothorax caused by rib exostoses.6–19 In these case reports, all patients were 21 years old or younger, and 12 were males. Diagnosis was made by computed tomography imaging or thoracentesis. Twelve of the 14 cases (86%) were managed surgically. The two nonoperative patients were treated with pleural drainage alone. The surgical cases were either treated preoperatively with chest tube drainage or brought directly to the operating room. Complete or partial rib resection was described in 8 cases and isolated exostosis removal was described in 4 cases.6,12,14,18 Thoracoscopy was used either in place of, or in conjunction with, thoracotomy in 4 cases.7,11,12,14 Most case reports did not describe their method of removal in detail, but a rongeur surgical instrument was used in 1 thoracoscopic case and 1 open case.6,14 Simansky et al. described in detail their use of a rongeur instrument through a port site incision. 14 A similar surgical concept of thoracoscopic rib-sparing resection of the lesion was employed in only 3 cases, 2 of which took place over a decade ago.12,14 We did not find any reports of thoracoscopic remodeling of the exostotic lesion using an orthopedic drill, as was used in our patient.
In summary, a patient with exostoses who presents with an acute onset of respiratory difficulty should raise concern for a hemothorax. In the case reported here, the source of bleeding remains unknown; one can assume that as the lung parenchymal injury site was simply not identified, the bleeding originated from an intercostal or tributary vessel in the visceral or parietal pleura. In the setting of a hemothorax, we believe that suspicious (e.g., spiculated) rib exostoses should be remodeled or removed to minimize the risk of recurrent bleeding. The use of an arthoscopic burr to shave the exostotic lesion and smooth the spiculations is technically feasible and provides the advantage of flattening the spicule while sparing the affected rib. Thoracoscopy is an excellent choice for addressing this clinical situation as it allows good visualization for evacuation of the hematoma as well as for treating the exostosis, while sparing the patient a formal thoracotomy.
Footnotes
Disclosure Statement
No competing financial interests exist.