
Abstract
Abstract
Objective:
An incidental finding of atypical endometrial hyperplasia (AEH) in women who have undergone laparoscopic supracervical hysterectomy (LASH) is a rare phenomenon, and it is unclear whether laparoscopic extirpation of the cervical stump (LECS) is justified in these patients.
Methods:
LECS due to AEH found incidentally in the morcellated uterus after LASH.
Results:
A total of 332 women underwent LASH between January 2002 and September 2010. Five of the women (1.5%) underwent secondary LECS procedures due to histological evidence of AEH or focal atypical endometrial cells found incidentally in the morcellated uterus. No atypical endometrial cells were histologically diagnosed in the cervical stump in any of the cases, nor were any endometrial cells found in the cervical stumps in any of the 5 patients. There was no abdominal evidence at all of any disseminated endometrial cells. In all 5 cases, cytological examination of peritoneal fluid confirmed the absence of adenocarcinoma cells.
Conclusions:
No signs of AEH were found in the removed cervical stumps. However, women should receive counseling regarding the need for secondary LECS to minimize any risks in such cases.
Introduction
Among the laparoscopic techniques available, laparoscopic supracervical hysterectomy (LASH), in particular, is currently undergoing a certain renaissance. The current intense debate on whether leaving the uterine cervix in situ confers advantages with regard to the pelvic floor and the risk of prolapse of the uterus need not be discussed in further detail here. However, no clear long-term advantages of leaving the cervix in situ have been reported. 3 The simpler operating technique with this method, which allows shorter operating times and lower intraoperative complication rates, as well as rapid convalescence and lower postoperative morbidity for the patients, is particularly attractive. 4 These advantages suggest that the LASH procedure may be superior.
Potential problems associated with leaving the cervix in situ have not been specifically studied, but they need to be taken into account when women are receiving counseling regarding different hysterectomy procedures. Atypical endometrial hyperplasia (AEH) is a very rare histopathologic finding, and the condition is potentially carcinogenic. Endometrial cancer is already present in 10%–53% of patients in whom AEH is diagnosed at biopsy.5–7 However, there are no current data regarding the risk of cervical stump adenocarcinoma after LASH when AEH is found in the body of the uterus incidentally after the procedure, or regarding any possible increase in risk due to morcellation of the uterus.
The aim of this study was to evaluate the rate of incidentally found AEH in women after LASH and whether laparoscopic extirpation of the cervical stumps (LECS) is a valuable and justified procedure in those women.
Materials and Methods
Between January 2002 and September 2010, a total of 332 women underwent LASH. The study was approved by the local institutional review board. All women underwent preoperative transvaginal ultrasound examination regardless of the menstrual cycle. Hysteroscopy and curettage before LASH were conducted in the women when the endometrial thickness was higher than 10 mm, and/or an inhomogeneous appearance was described during preoperative transvaginal ultrasound or when the women reported menstrual bleeding anomalies with regard to the duration or rhythm. All surgeons conducting the procedures were experienced in laparoscopic surgical techniques. The surgical technique of the LASH procedure has been previously described in detail.8,9 In brief, the round ligament is divided first, followed by the fallopian tube and the utero-ovarian ligament; both the anterior and posterior leaves of the broad ligament are divided with scissors after bipolar diathermy. The uterine vascular pedicle is also cut through with scissors after bipolar diathermy. The corpus uteri is separated from the cervix in the isthmic area of the uterus by using a monopolar needle. The corpus uteri is removed after morcellation with an electric morcellator. Histological examination of the morcellated uterus identified 5 women with AEH, as an incidental finding. The AEH was diagnosed as defined by the World Health Organization classification: atypical endometrial proliferation with clear cytological atypia not fulfilling the diagnostic criteria of endometrial carcinoma. The diagnosis by an experienced pathologist specialized in gynecological pathology was verified in every case by a second pathologist. No special or immunohistochemical stains were required.
Laparoscopic extirpation of the cervical stump
The LECS procedure was carried out on analogy with the total laparoscopic hysterectomy procedure by using the Hohl instrument (Karl Storz, Ltd., Tuttlingen, Germany) and has been previously described in detail.8,9 Briefly, the Hohl instrument is introduced into the cervix. In this way, the adapter encloses the vaginal part of the cervix. The lower parts of the broad ligament, including the uterine artery, are transected after bipolar coagulation, if necessary. The procedure is conducted analogously on each side. After this, the Hohl instrument is elevated into the abdomen, so that tension is created at the cervicovaginal junction. This results in dislocation of the vaginal fornices (and the vaginal part of the cervix) from the bladder and from the distal part of the ureter, as well as lateralization of the bladder pillars over the edge of the adapter. The anterior fornix of the vagina is easily identified and is separated with the monopolar needle along the edge of the adapter in the vaginal part, directly at the uterine cervix. The vesicouterine space does not have to be dissected in all cases, and the uterosacral ligaments can also be preserved. The Hohl instrument together with the cervix is then withdrawn into the vagina and removed through it. A laparoscopic suture to close the vagina is possible, as well as a suture from the vaginal side. A detailed description of the use of the Hohl instrument is also presented in EndoWorld Gyn no. 16-D. 10
For LECS, the operating time was measured from the insertion of the Hohl instrument to skin closure at the last trocar site. Hemoglobin values were measured on the day before the operation and on the first postoperative day. Complications were classified as follows:
• Intraoperative complications: transfusion-related hemorrhage, injury to the bladder, intestine, ureter, or vessels, and anesthesiological problems • Conversion to abdominal hysterectomy • Postoperative complications: infection or temperature higher than 38°C, hematomas, revisions/secondary procedures, deep venous thrombosis, fistula formation, and wound healing disturbances
After the procedure, histological examination using routine hematoxylin–eosin staining of the removed cervix was performed.
Statistical presentation of the data
All the data are presented as means plus or minus standard deviation and 95% confidence intervals (CI), unless otherwise noted. All the statistical analyses were carried out using the Statistical Package for the Social Sciences (SPSS, version 18.0 for Windows; SPSS, Inc., Chicago, IL).
Results
During the study period, 332 patients underwent LASH. The patients' mean age was 45.5±5.3 years (95% CI, 45.0–46.3), and their mean body mass index (BMI) was 25.3±4.3 kg/m2 (95% CI, 24.6–25.6). Leiomyomas were the most frequent reason for LASH. The symptoms of the patients are presented in Table 1.
LASH, laparoscopic supracervical hysterectomy; LECS, laparoscopic extirpation of the cervical stump.
Laparoscopic extirpation of the cervical stump
A total of 5 women underwent secondary extirpation of the cervical stump (LECS), because AEH was found incidentally in the morcellated uterus. All patients had an unremarkable pap smear and revealed no symptoms of any cervical dysplasia. One woman revealed a suspicious endometrium on ultrasound and received hysteroscopy and abrasion before LASH. These patients' mean age was 50.9±10 years, with a mean BMI of 24±2.31 kg/m2. The time from LASH to LECS was 3 months in 4 women and 5 months in one woman with an average latency period of 3.4 months.
The surgical data for the women who underwent LECS due to AEH are shown in Table 2. Four women underwent LASH due to symptomatic leiomyoma. They had regular menstrual periods and denied experiencing any anomalies with regard to the duration, or rhythm of their menstrual bleeding. Three women (37, 41, and 45 years old) did not have any exogenous hormone supplementation. One woman (51 years old) reported the use of homeopathic medications with “agnus castus” because of menopausal symptoms. Further, no ovarian disorders were reported in the medical history of all 4 women. The normal-appearing endometrium showed maximum thicknesses of 6.6–7.7 mm. LASH was performed without any complications. Histopathological examination of the specimens showed multiple myomas without necrosis or mitoses. Additionally, AEH or focal atypical endometrial cells were found during the final histopathologic examination of the morcellated uteri, but there was no evidence of endometrial cancer.
Surgical data are given as means±SD and 95% CI.
CI, confidence interval; SD, standard deviation; ECS, extirpation of the cervical stump.
The fifth woman (56 years old) in the group presented at the hospital due to hypermenorrhea. The woman suffered from menopausal symptoms and performed an oral hormonal therapy with 2 mg Estradiol and 1 mg Norethisteron acetate per day, as prescribed by her gynecologist. The ultrasound examination showed a normal-appearing endometrium, which was homogeneous and clearly visible in the whole uterus with a maximum thickness of 11 mm. Hysteroscopy and curettage of the uterus were performed before LASH because of the increased thickness of the endometrium. The hysteroscopy revealed a normal endometrium without any macroscopic abnormalities. The histopathologic findings were unremarkable. No hyperplasia or atypical cells were found. Due to heavy bleeding during the next weeks, the patient insisted on undergoing LASH, which was performed 12 weeks later, while she continued her hormonal therapy until LASH. After complete histological processing by the same pathologist, a diagnosis of simple endometrial hyperplasia with focal atypia was made (Fig. 1). However, there was no evidence of malignancy.
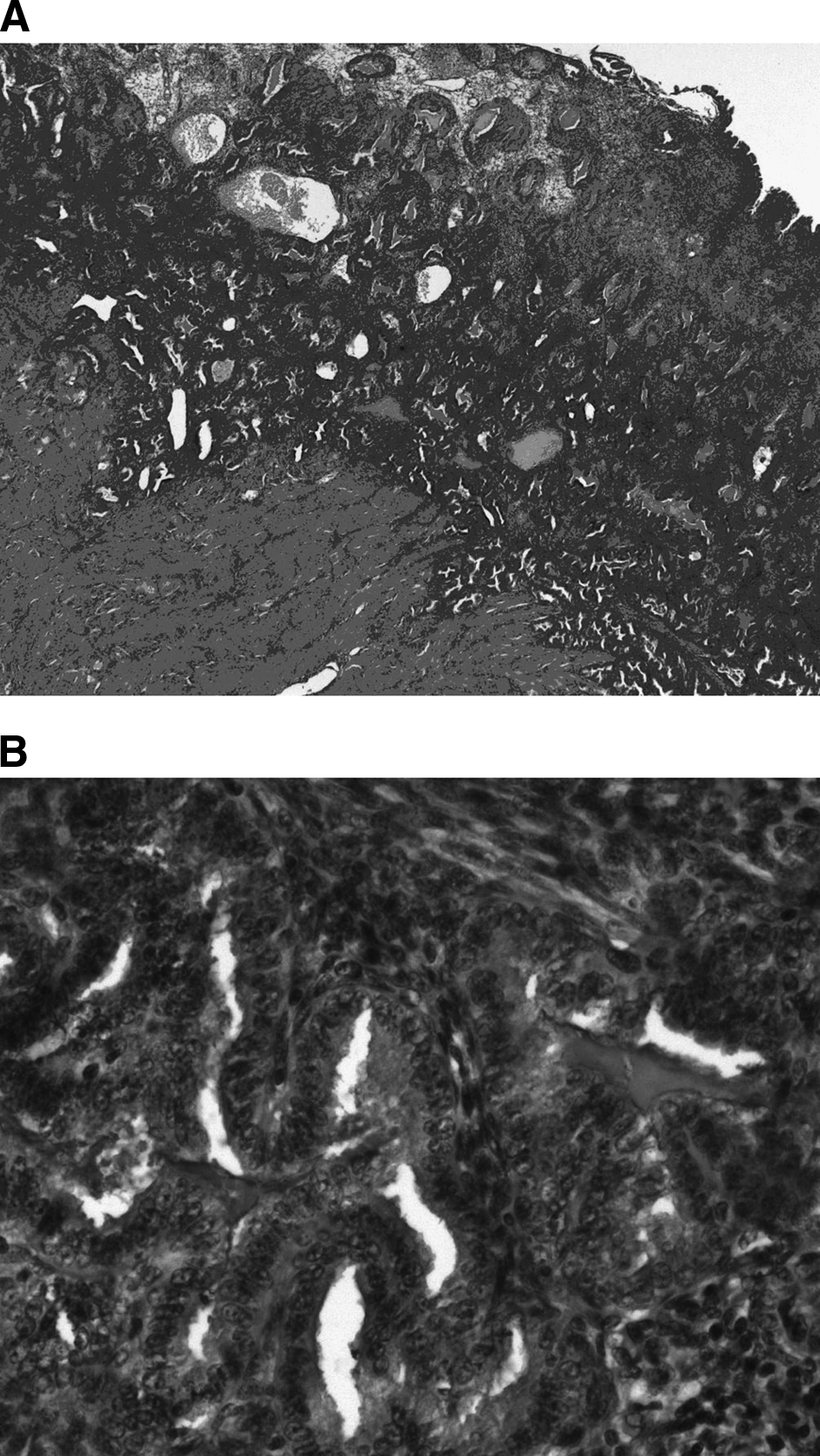
Hematoxylin–eosin, original magnification 20×
The LECS was carried out without any complications in all 5 of these patients. No abdominal evidence of disseminated endometrial cells was found at all. Cytological examination of the peritoneal fluid in all 5 cases confirmed the absence of adenocarcinoma cells. Histological examination of the excised cervical stumps showed unremarkable findings in all 5 women, and no endometrial cells were found in the cervical stumps in any of the 5 patients.
Discussion
This study reports 5 cases of AEH found incidentally after LASH in 332 women. AEH is normally a risk factor for endometrial cancer.5–7 However, the risk of cervical stump adenocarcinoma is unknown in women in whom AEH is found incidentally after LASH in the morcellated body of the uterus.
LASH is one of the safest hysterectomy procedures, with intraoperative complication rates near 1%. 4 In a prospective and randomized study, Morelli et al. observed no significant differences between laparoscopic subtotal and total hysterectomy with regard to complication rates or clinical outcomes during a 2-year follow-up period. 11 Their results are generally in agreement with our own experience in laparoscopic hysterectomy procedures.12–14 The general complication rates lie in the range of 1%–2%.4,8–14
Although leaving the cervix in situ is not acceptable to some women, as they do not wish to have any further bleeding, removal of the cervix is not acceptable to other women who have concerns regarding possible changes in their sexuality. In patients who wish to have the uterine cervix preserved, LASH offers an attractive alternative to complete hysterectomy.2,3 However, the possibility that problems may develop after LASH, resulting in a need for secondary surgical procedures such as extirpation of the cervical stump, has not been previously adequately investigated.
Only a few studies have been published to date on secondary surgery after LASH, leading to LECS. In our department, the rate of secondary LECS after an initial LASH procedure was low in the period 2002–2009 at 3%. Those rates were reported also by other groups. For example, in a retrospective multicenter study, van Evert et al. reported extirpation of the cervical stump in 2% of women after LASH procedures. 15
Especially women with supracervical hysterectomy and uterine morcellation for presumed benign uterine disease who are later found to have malignancy during final pathology may represent a management dilemma. 16 In the present study, LECS procedures were performed due to AEH in 1.5% of patients who had undergone LASH. AEH is a very rare histopathologic finding, and the condition is potentially carcinogenic. Endometrial cancer is already present in 10%–53% of patients in whom AEH is diagnosed at biopsy.5–7 There are no current data regarding the risk of cervical stump adenocarcinoma after LASH when AEH is found in the body of the uterus incidentally after the procedure. Nor are there any data regarding a poorer prognosis due to morcellation, with at least a theoretical risk of concurrent endometrial cancer. If an endometrial carcinoma is present, morcellation of the uterus is contraindicated. Even with hysteroscopy alone, there is a significant rate of intraperitoneal dissemination of endometrial cancer cells. 17 Morcellation of the uterus would make the rate of intraperitoneal dissemination even worse, thus resulting in an upstaging of the disease in some women, whereas women who undergo completion surgery with restaging and are not upstaged appear to have a good prognosis. 16 In all 5 patients in whom AEH was found in the uterus after LASH, no atypical cells or malignancy were diagnosed in the secondarily removed cervix after LECS. LECS is a safe and feasible procedure using the Hohl instrument. However, it is not known whether the procedure is justified after LASH in women in whom AEH is found incidentally in the endometrium of the morcellated uterus. For AEH, the cumulative risk for progression to endometrial carcinoma increases from 8.2% (95% CI, 1.3%–14.6%) over 4 years, to 12.4% (95% CI, 3.0%–20.8%) over 9 years, and to 27.5% (95% CI, 8.6%–42.5%) over 19 years. 18 All of the women in whom AEH was found after LASH were, therefore, recommended to undergo LECS to minimize all possible risks.
Carcinoma in the endometrial layer can normally be diagnosed by hysteroscopy and curettage with a high level of specificity; false-negative findings are rare. However, this was not possible in one of the patients in the present study, as focal atypical cells in the endometrium were not detectable during hysteroscopy and curettage before the LASH procedure. The possibly initial false-negative result was not re-reviewed by a second pathologist, and the women continued their hormonal treatment regime after the hysteroscopy and curettage. These are the two limitations making the interpretation of this rare phenomenon impossible.
Before either total or supracervical hysterectomy is performed, it has to be ensured that the patient is not suffering from a malignant disease of the uterus or ovaries. Depending on the patient's history and the preoperative examination, most malignancies can be diagnosed or anticipated before surgery. Only women without bleeding disorders and those who have an inconspicuous Pap smear and an endometrium that is unremarkable on ultrasound should be offered the option of having the cervical stump left in situ. 19 Even other risk factors, for example, BMI of the patients, should not be unaccounted for this decision. In the group of obese patients (BMI≥30 kg/m2), there is a significant elevated endometrial caner risk (hazards ratio of 1.67) in comparison to the normal weight of the female population. 20 However, none of our 5 patients could be assigned to this high-risk obesity group. The relevance of an endometrial biopsy or of hysteroscopy and curettage before hysterectomy in unselected patients with unremarkable findings appears to be questionable. To date, no clear guidelines are available as to whether histological evaluation of the endometrium before LASH procedure should be recommended in all women or only in those with higher risks of developing endometrial cancer. In none of our women with LECS due to AEH, a specific disorder associated with anovulatory disorders (i.e., polycystic ovarian syndrome) or with an unopposed estrogen status was reported. Only 1 woman received an estrogen-progestin therapy. Nevertheless, the postoperative need for LECS after LASH needs to be placed in perspective in this context and should be offered to patients to minimize risks. Further, in patients with continued bleeding after LASH and with a nonsuspicious histology of the removed uterus, the extirpation of the cervical stump may be discussed individually, and LECS can be considered a possible alternative.
Footnotes
Disclosure Statement
No competing financial interests exist.