
Abstract
Abstract
Background:
To explore the feasibility and safety of gas-free single-port transumbilical laparoscopic cholecystolithotomy.
Methods:
An incision of 1.5–2.0 cm was made through all layers of the umbilicus, and a specially designed silicone plug with three 5-mm ports was inserted. The surgical space was created by lifting the right abdominal wall with an abdominal suspension set. A laparoscope, S-type dissector, grasper,electric needle, and needle-holder were used to perform a cholecystolithotomy. The procedure was performed in 8 patients with gall stones.
Results:
All stones were successfully removed. No postoperative complications, such as bleeding or bile leakage, occurred. The operative time was 45–120 minutes (mean 77.5 ± 24). The mean length of hospital stay was 2 days, and no postoperartive analgesics were used. There were no visible scars on the abdominal wall.
Conclusions:
The gas-free single-port transumbilical laparoscopic approach was safe and feasible for cholecystolithotomy. This approach expands the applications of laparoendoscopic single-site surgery and avoids the use of highly concentrated CO2 in the body and its potential side effects.
Introduction
Although the pneumoperitoneum platform is relatively safe for patients, high CO2 inflation pressure causes functional impairment of the heart and lungs and blood acid-base disturbance during surgery, leading to reduction of tidal volume, tachycardia, and hypercapnia. The CO2 in the pneumoperitoneum may also lower the pH in the surgical field, resulting in local immune suppression.3–6 The pneumoperitoneum may result in intraoperative atelectasis that reduces pulmonary gas exchange 7 and in some cases, the positive end-expiratory pressure is needed in the laparoscopic gallbladder surgery to improve the ventilation. 8 To avoid these effects of pneumoperitoneum, some surgeons prefer the gas-free approach for cholecystectomy. 9 This approach has been successfully employed in conventional laparoscopic cholecystectomy.10,11 We also successfully performed gas-free laparoscopic cholecystectomy and found that it improved the post-operative recovery.12,13 To expand the applications of LESS surgery, we proposed gas-free transumbilical single-site laparoscopic gallbladder surgery. Here we report on the feasibility and safety of gas-free transumbilical single-site laparoscopic cholecystolithotomy from our preliminary experience with 8 cases.
Patients and Methods
Clinical data
Eight female patients were admitted for laparoscopic cholecystolithotomy from November to December 2009. Their ages ranged from 29 to 54 years (36.8 ± 8.8 years old), and they had a body mass index of 18.8–22.6 (20.2 ± 1.3). All of these patients had presented with upper abdominal discomfort, the source of which was diagnosed as a solitary gallstone with mild chronic cholecystitis. The diagnoses were based on history, physical examination, laboratory tests, and radiological imaging. The diameter of the gallstones ranged from 1–2 cm, and the thickness of gallbladders was less than 3 mm. The functional contraction of the gallbladder was determined by ultrasonographic evaluation. All the patients in this study had requested preservation of the gallbladder and removal of the stones only. The laparoscopic cholecystolithotomy for selected patients was approved by the institutional review board of the ethics committee of Shanghai East Hospital. The patients provided written informed consent. All surgical interventions were performed by the same operative team at Shanghai East Hospital.
Surgical technique
Preoperative preparation included colon preparation by enteroclysm. The patients underwent general anesthesia after tracheal intubation and then stomach decompression by gastric tube. The operator stood on the patient's left side, and the assistant stood on the patient's right side. The patient was placed in the reverse Trendelenburg position, and the operating table was rotated to bias with the right side up.
A tri-channel single laparoscopic port was inserted through a 1.5-cm, all-layer umbilical incision (Figs. 1 and 2). Instead of a pneumoperitoneum, three 15-cm-long and 1-mm-diameter stainless steel wires strong enough to lift the anterior abdominal wall without bending were tunneled subcutaneously through a 1- to 2-mm skin incision on the right side of the abdomen near the gallbladder. One wire ran parallel to and 2 cm above the right costal arch; the second ran from 5 cm under the xiphoid to 4 cm above the umbilicus; and the third was placed from the cross point of the anterior axillary line and right costal arch inferiorly to the level just superior to the umbilicus and parallel with the second line. The anterior abdominal wall was then lifted superiorly and slightly outward (i.e., away from the surface of the abdomen) by the traction rods. The traction was maintained with the help of the arch and clamp bars of the extension retractor set. (Fig. 3)

Silicone tube.

The placement of the specially designed three-channel port.
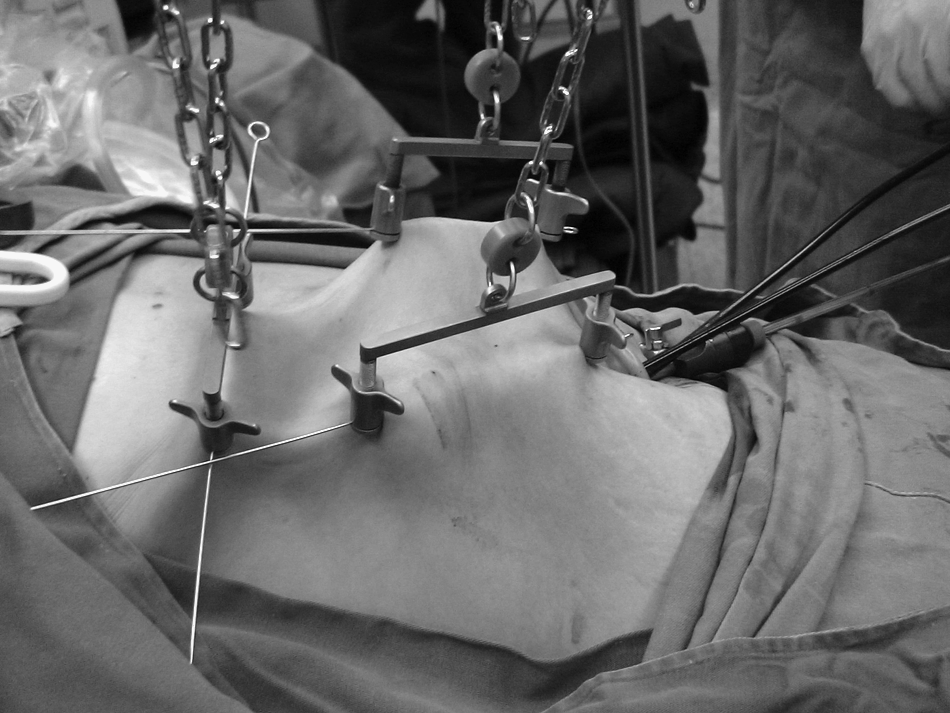
Abdominal wall suspension device.
The tri-channel single laparoscopic port consists of three 5-mm lumen surrounded by an elastomer sleeve that allows the smooth insertion of instruments and accessories. A 5-mm semi-flexible video scope (Olympus LTF-VP, Tokyo, Japan) was inserted through the 5-mm lumen and used to expose the surgical area with adjustments of the flexible tip of scope. The lifting height and position of the wires were also adjusted to maximize exposure of surgical area. An S-type dissector and grasper or an electric needle and needle-holder were inserted through the other two 5-mm lumens.
After lifting the gallbladder, a 1- to 2-cm incision was made on the fundus by electrocautery, followed by aspiration of the bile juice. The single stone was removed with a grasper. Before suturing the gallbladder incision, the gallbladder was explored for remnant stones or sand by inserting the fiber choledochoscope. After carefully rinsing the gallbladder to avoid any blood clot formation and remove sand, the incision on the fundus of gallbladder was round-sutured with 3-0 absorbable Vicryl. The surgical area was rinsed with saline until it was clear, followed by aspiration of all fluids. The stone was placed in a sample sack and subsequently extracted through the umbilical incision. The umbilical incision was sutured with absorbable stitches (Fig. 4).

The umbilical incision was sutured with absorbable leptonema.
Results
To explore the feasibility and safety of gas-free single-port laparoscopic gallbladder surgery, we applied the technique to cholecystolithotomies. All stones were successfully removed without converting to traditional laparoscopy surgery. The operative time ranged from 40 to 120 minutes (77.5 ± 24 minutes). No instances of injury or bleeding occurred. Indeed, the exposure of the surgical area was satisfactory with the new technique. After surgery, none of the patients required analgesic medications including acetaminophen. The patients all recovered rapidly without postoperative complications, such as bile leakage, bleeding, or wound infection. All the patients could get out of bed and drink water 6 hours after surgery. All the patients were discharged on the second day after surgery. The surgical scar was almost completely concealed within the umbilicus (Fig. 5), providing a satisfactory cosmetic result.

Cosmetic result, 2 days after surgery.
Discussion
Minimally invasive surgical techniques have allowed for a reduction in the morbidity and recovery time associated with surgery and with better cosmetic results. The first report of natural orifice trans-luminal endoscopic surgery in 2004 was not advocated in by academic surgical societies until the success of transvaginal endoscopic cholecystectomy in 2007. No-scar or covert-scar surgery has become increasingly popular and expanded to various operative procedures. Most of these approaches have focused on single-port surgery. More than 20 existing approaches have been described and reported for single-port surgery.14–17 As a result, the term LESS surgery had been developed to cover all these single-port surgeries.14–17 LESS surgery is certainly attractive, but many issues still need to be solved. Based on our experiences in developing single-port transumbilical endoscopic surgery, 18 the main disadvantages relate to the technical difficulty of the surgery that results in doubling the operation time for a three-port covert transumbilical endoscopic surgery. The resulting long duration of the pneumoperitoneum in this newer technique will be a great concern to anesthetists, patients, and surgeons.19,20
For conventional laparoscopic surgery, a gas-free approach has been successfully developed. Several reports describe successful laparoscopic cholecystectomy with an abdominal-wall lifting technique.10,11,13 In this pilot study, we evaluated the feasibility and safety of a gas-free LESS technique in 8 cases of laparoscopic cholecystolithotomy. All eight operations were successfully completed without any complications, and the patients were discharged 48 hours after the operation. These results suggest that this technique is feasible and safe in this setting.
In our preliminary experiences, we found the main difficulty was in establishing the operative field; without the pneumoperitoneum the abdominal cavity is smaller, and the intestine trend to move into the lifted space. To overcome this problem, we inserted three wires to lift a 15 × 15-cm2 area (as measured on the skin). In addition to two paralleled steel wires in the upper abdomen, a third suspension wire 2-cm above the right costal arch is especially important. This not only reveals the posterior aspect and body of the gallbladder, but also provides the surgical space for incising and suturing the gallbladder in cholecystolithotomy. We also found that the preoperative enteroclysm and gastric tube suction is useful to empty intestinal contents and prevent gastric dilatation. In addition, the surgery should be performed with satisfactory muscle relaxation. The angle of the reverse Trendelenburg and lateral tilt (with the left side lower) should also be greater than in conventional gallbladder surgery.
As with a conventional single-port operation, it is important to avoid interference between instruments. In the single-port laparoscopic cholecystectomy, one grasper retracts the gallbladder ampulla laterally and proximally, whereas the other device dissects the cystic triangle. Under these circumstances, not much interference occurs. However, in single-port laparoscopic cholecystolithotomy with pneumoperitoneum, an operation angle should be created for the instruments during the suturing of the gallbladder incision. To allow for this, we designed an “S”-shaped grasping forceps and needle holder forceps. Theoretically, two “S”-shaped devices can be more effectively coordinated in suturing the gallbladder incision. However, we found that one “S”-shaped grasper with another conventional straight needle holder clamp was sufficient for avoiding interference between instruments. Moreover, a 5 mm-diameter flexible laparoscope plays a key role in providing the best view of the single-port laparoscopic cholecystolithotomy.
Our initial experience suggested that gas-free LESS cholecystolithotomy is safe and feasible for patients with a normal body mass index, although it is more difficult than conventional LESS surgery. Further development of newer devices and instruments is necessary to make the procedure easier.
Footnotes
Disclosure Statement
No competing financial interests exist.