
Abstract
Abstract
Background:
Single-incision pediatric endosurgery (SIPES) is gaining popularity for routine ablative operations such as appendectomy and cholecystectomy in a number of centers. We have employed this technique for Nissen fundoplication for the first time as a major reconstructive procedure. This study describes the technical evolution of SIPES fundoplication at our center, discusses the challenges, and evaluates the outcome.
Materials and Methods:
After IRB approval was obtained, data were prospectively collected on all SIPES fundoplications performed in our hospital from September 2009 through August 2010. The surgical techniques, operative times, blood loss, complications, conversion rates, and outcomes were recorded.
Results:
SIPES fundoplication was attempted in 10 children (ages 3 months to 11 years, median 21 months; weight 3.45–51 kg, median 9 kg). Fundoplication was performed as the sole procedure in 4, and combined with a gastrostomy in 6 patients in which case the gastrostomy was used as an additional trocar site. On average, total operative time was 104 ± 31 minutes, and reached a baseline around 90 minutes after five procedures. The mean estimated blood loss was 6 ± 5 mL, and postoperative length of stay 2.6 ± 1.4 days. Different trocars, liver retraction methods, and suturing techniques were employed. Extracorporeal knot tying was used in six operations. There were no intraoperative complications, but unplanned additional trocars or access sites were added in 2 cases, leaving 3 patients in which the procedure was carried solely through the umbilicus. Reflux symptoms subsided in all patients, but 1 patient had recurrence at 12 months postoperative and underwent conventional laparoscopic redo-fundoplication.
Conclusion:
Laparoscopic Nissen fundoplication can be accomplished successfully and safely using single-incision endosurgery in children with good antireflux efficacy and without leaving any appreciable scar. Extracorporeal knot tying appears to be superior to other methods. So far, the failure rate is not higher than in conventional laparoscopic Nissen fundoplication.
Introduction
At the start of this study, over 120 SIPES cases in children had been performed in our center, 4 and the division generally performs between 100 and 150 laparoscopic Nissen fundoplications per year. The resulting experience was the basis for performing this study, in which we prospectively evaluated the technical feasibility and outcome of SIPES Nissen fundoplication.
Materials and Methods
Institutional Review Board approval was obtained (Protocol number X090814001). Data were prospectively collected on all SIPES fundoplications performed in our hospital from September 2009 through August 2010. It included patient age, gender, weight, diagnosis, operative technique, operative time, estimated blood loss, conversion (insertion of additional trocars), complications, length of stay, and outcome.
Patient selection for SIPES Nissen fundoplication was based on attending preference, as was equipment selection. Generally, SIPES fundoplication was attempted in all consecutive patients with an indication for fundoplication. Without formal exclusion criteria, SIPES fundoplication was not attempted in redo cases, patients who had prior abdominal surgery (except for placement of a ventriculoperitoneal shunt in 1 patient), or who had anatomic reasons such as significant scoliosis or contractures. In cases where a gastrostomy was planned along with the fundoplication, the future gastrostomy site was used as an additional trocar site. Postoperatively, patients were discharged home when patients tolerated full enteral feeds and pain was manageable with analgesics by mouth or gastrostomy tube (ibuprofen and/or acetaminophen).
Different methods for knot-tying were developed, evaluated, and practiced in an in vitro training model before applying them on the patient in the clinical setting.
Patients were followed in an outpatient clinic and photodocumentation of the abdomen was performed at each visit.
Results
Over the study interval, SIPES fundoplication was attempted in a total of 10 children (ages 3 months to 11 years, median 21 months; weight 3.45–51 kg, median 9 kg; 6 girls and 4 boys). Fundoplication was performed as the sole procedure in 4, and combined with gastrostomy placement in another 6 patients. On average, total operative time was 104 ± 31 minutes. While the first case took over 3 hours to complete, operative time declined and reached a baseline around 90 minutes after the first three to five procedures (Fig. 1).
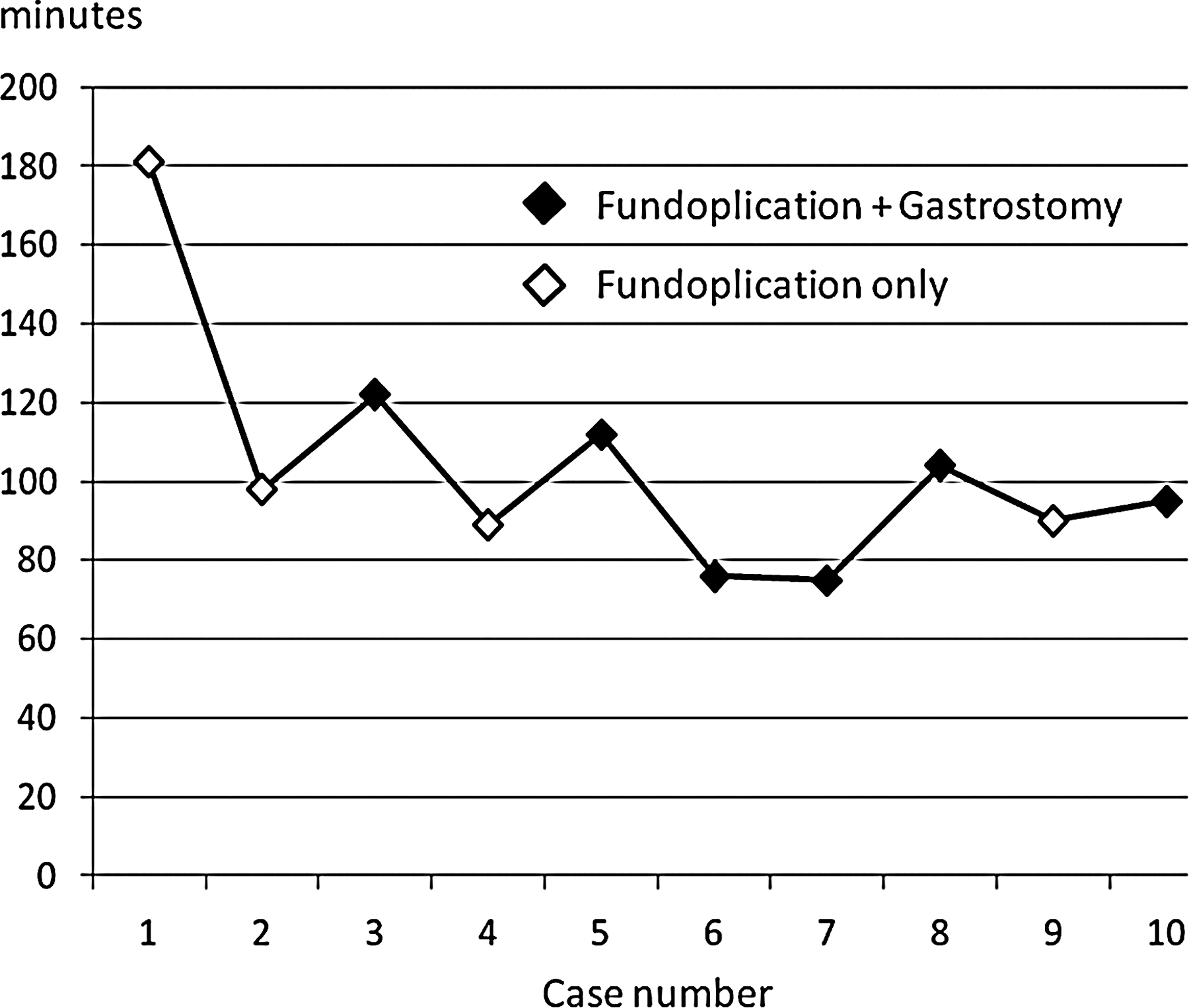
Operative times for single-incision pediatric endosurgery Nissen fundoplication in chronological order of cases. A plateau is reached early, indicating a steep initial learning curve.
On average, the estimated blood loss was 6 ± 5 mL, and the postoperative length of stay was 2.6 ± 1.4 days. The dissection phase of the operation was accomplished without difficulty and was similar in all patients. We generally take down the gastrohepatic ligament, dissect the right esophagocrural space, divide the most cranial portion of the gastrosplenic ligament along with the short gastric vessels, and complete the retroesophageal dissection from the left. As shown in Table 1, different proprietary trocars, liver retraction methods, and suturing techniques were employed. Extracorporeal knot tying was used in six operations. There were no intraoperative complications, but additional trocars were added in 2 cases.
GERD, gastroesophageal reflux disease; FTT, failure to thrive; CP, cerebral palsy; DR, developmental retardation; y, m, year, month; y/n, yes/no; SILS port (Covidien) and TriPort (Olympus).
The initial dissection of the abdominal esophagus, including division of the short gastric vessels and creation of the retroesophageal window, was found to be fairly straight forward, especially using a 45° telescope. A minimal mobilization approach to the esophagus was employed due to recent evidence to support that this lessens long-term fundoplication failure. 4 Suturing was the most challenging part of the operation, and was accomplished using four distinct methods (Fig. 2), which all had advantages and disadvantages to be discussed.
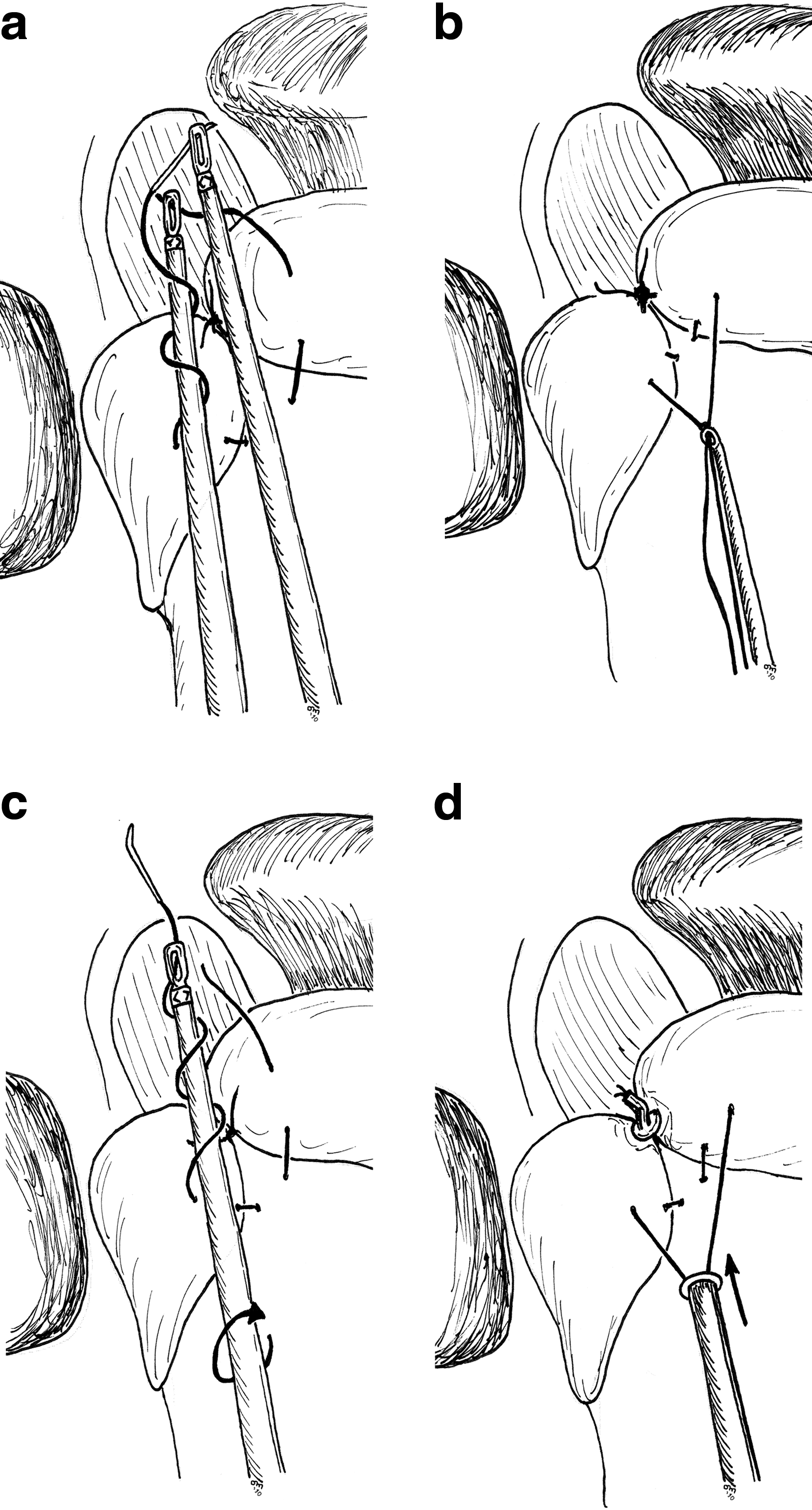
Different single-incision pediatric endosurgery suturing techniques applied in this study. In the Magic Wand technique
After an average follow-up time of 8.5 months (range 1–14 months, median 9 months), the umbilical incision was inconspicuous. Reflux symptoms subsided in all patients, but 1 patient (patient 2) had recurrence at 12 months after the procedure and underwent conventional laparoscopic redo-fundoplication. This patient had undergone dilatation of a lower esophageal stricture 3 months postoperatively that had resulted from long-term gastroesophageal reflux.
Discussion
To our knowledge, this is the largest series of single-incision laparoscopic fundoplications in children or adults published so far. Despite the limited number of patients and the inconsistent techniques employed, this study highlights many important aspects, challenges, and solutions of SIPES Nissen fundoplication.
For one, the dissection phase of the operation is easily accomplished, whereas the reconstruction part can be quite difficult. In our first patient, dissection of the hiatus and esophagus was performed in <60 minutes. After unsuccessful attempts at suture placement over the next hour, the decision was made to insert two additional trocars to complete the wrap. Because laparoscopic Nissen fundoplication at our hospital is usually performed using a total of five incisions, this was already a step ahead towards a less-invasive operation.
Generally speaking, several tricks and tactical maneuvers can be utilized to overcome some of the drawbacks of operating through a single umbilical incision. 5 These include using a long telescope and different instrument lengths to increase hand separation, and working in a more anteroposterior direction. It is also important to have enough intraabdominal domain. In patient 6, gross bowel distension after several attempts of a endotracheal intubation prompted conversion to standard conventional laparoscopic technique in the first 5 minutes of the operation.
Suturing with instruments in parallel alignment turned out to be the most complex task of the operation. Despite many attempts, wrapping a C-loop of suture around a counter-instrument without angulation proved impossible. In the Magic Wand technique (Fig. 2a), using the needle as an articulation device allows the surgeon to wrap the suture around an instrument in very tight places, but the surgeon's hands come in close proximity to each other and a great deal of dexterity is required. In our series, this was the quickest way of tying the sutures (resulting in a total operating time of 75 minutes including the gastrostomy, patient 7). Using a dynamic or static articulating grasper simplifies the process. Automatic suturing devices use a rivet mechanism to secure the suture in place (Fig. 2d). They are easy to use, but the disadvantage is a relatively high cost and the fact that foreign bodies are left in situ. Although we have no experience with it, the retained rivets may complicate performing a future redo-fundoplication if needed. Using extracorporeal knot tying and a reusable knot-pusher (Fig. 2b) is simple, fast, and cheap. It has become our method of choice for SIPES fundoplication. The Spaghetti technique is unique because the knot can be started with a single instrument (Fig. 2c). This is particularly useful for securing the first fundoplication stitch. Once the free end is grasped, the second instrument stabilizes the needle end of the suture to pull the free end through and tighten the knot.
It is conceivable that the postoperative dilatation of the persistent distal esophageal stenosis led to fundoplication failure in patient 2. According to our own data, postoperative esophageal dilatation increases the risk of recurrent gastroesphageal refux after fundoplication by a factor of 10.8. 6
One study describes anecdotal single-incision laparoscopic fundoplications in adults using double precurved reusable instruments. 7 We have evaluated these instruments in vitro and found them less suitable for pediatric surgery because of the difference in size of pediatric patients, ranging from infants to teenagers. Because the distance between the umbilicus as a fulcrum and the operative field determines in which locations the instrument must be angulated, a different set of pre-bent instruments is theoretically necessary for every patient size. So far, different age-appropriate sets of bent instruments are not available, and would possibly be quite costly to produce because of the smaller numbers.
Although we mostly used standard straight instruments for the procedures, a dynamic (Realhand; Novare Surgical, Cupertino, CA) or static (Roticulator; Covidien, Norwalk, CT) articulating grasper was employed in 6 of the 10 operations. These tools are particularly helpful for pulling the fundus around the esophagus through the retroesophageal space by passing the empty grasper behind the esophagus from the patient's right to left, aiming the tip of the instrument anteriorly and grasping the fundus that is placed into its jaws using the surgeon's other instrument.
Liver retraction during single-incision laparoscopic fundoplication is problematic. Recently, a technique was described in 3 adult patients in whom a Penrose drain was tacked to the abdominal wall, suspending the left lobe of the liver with a mechanism like a hammock. 8 In our series, a dynamic grasper was used to hold the liver away when necessary in some cases. In the remainder, a 2-mm trocarless instrument (Mini-Lap Technologies Inc., Dobbs Ferry, NY) was passed under the liver and anchored in the diaphragm above the hiatus, suspending the liver on its shaft. In the future, magnetic retraction systems already described for single-incision laparoscopic cholecystectomy 9 may prove helpful for Nissen fundoplication as well.
Although Allemann et al. 10 have described the challenges of single-incision laparoscopic Nissen fundoplication in a porcine model and proposed robotics as a means to overcome them, we believe that the high cost involved currently makes the application of robotics for single-incision fundoplication in the pediatric clinical setting unrealistic.
In a recent meta-analysis, laparoscopic Nissen fundoplication for gastrooesophageal reflux disease in children has clear advantages over the open procedure in terms of earlier feeding, less morbidity, and earlier hospital discharge, 11 at a comparable cost. 12 At this time, the advantages of performing SIPES over conventional laparoscopic Nissen fundoplication are mainly cosmetic in nature. The benefit of virtually scarless surgery in neurologically impaired children who also require a gastrostomy is debatable. In general, this advantage must be carefully weighed against the added complexity of the case. Good intraoperative judgement is paramount to recognize at what time the SIPES approach should be abandoned and additional trocars placed in order to safely complete the procedure. Our study, however, shows that laparoscopic Nissen fundoplication can be accomplished successfully and safely using single-incision endosurgery in children. More patients will be needed to standardize the technique in order to conduct future comparative studies and cost analyses. Only a prospective study can truly evaluate any additional potential benefit of SIPES versus conventional laparoscopic fundoplication. So far at least, the efficacy and recurrence rate is comparable to the conventional laparoscopic technique. The excellent postoperative cosmesis makes this technique particularly suitable for neurologically normal children with gastroesophageal reflux refractory to medical therapy.
Footnotes
Disclosure Statement
Drs. Muensterer, Perger, Hansen, Lacher, and Harmon have no commercial association that might create a conflict of interest in connection with any of the products mentioned in this article.