
Abstract
Abstract
Purpose:
Various techniques for minimally invasive thyroid surgery have been described over the last decade. As interest in single-port access laparoscopic surgery (SPA™) continues to grow, the authors present their technique and short-term outcomes for single-port access transaxillary totally endoscopic thyroidectomy in the management of benign thyroid tumors in a series of 4 patients.
Patients and Methods:
Four consecutive patients from a prospectively maintained endoscopic thyroidectomy database were analyzed under an institutional review board-approved protocol. Clinical characteristics and short-term outcomes were reviewed.
Results:
All the patients were young women with no prior neck surgery. A single-port totally endoscopic thyroidectomy was performed for thyroid adenoma in 2 cases and for nodular goiter in 2 cases. Retraction, exposure, and extraction were possible in all cases. The average operating room time was 92.5 minutes. Postoperative pain scores on postoperative day 1 were all 1/10. No patient experienced complications. The median hospital stay was 1.75 days. The mean specimen size was 2.7 cm × 2.375 cm × 2.625 cm. The patients were uniformly pleased with the cosmetic results of the operation.
Conclusions:
Single-port access transaxillary totally endoscopic partial thyroidectomy appears to be safe and feasible. This technique may provide both an attractive way to reduce injury to the anterior neck tissue and a method for ideal cosmetic effect.
Introduction
Patients and Methods
Four consecutive patients were retrospectively reviewed from a prospective database of endoscopic thyroidectomy. Thyroid nodules were diagnosed preoperatively based on ultrasonography-guided fine-needle aspiration biopsy and neck computed tomography findings. A single-port totally endoscopic thyroidectomy was offered to patients according to criteria specifying young female gender, unilateral thyroid benign lesion with lesion diameter of less than 3 cm, strong desire for cosmesis, and lack of history of thyroiditis, neck surgery, or radiation therapy. A lesion located in the thyroid dorsal area (especially adjacent to the tracheoesophageal groove) owing to possible injury to the trachea, esophagus, or recurrent laryngeal nerve (RLN) was also excluded. All patients provided complete informed consent regarding the nature of the surgical procedure and risks involved before the procedures were performed. The study was performed under institutional review board approval. The demographic data for each patient are shown in Table 1.
The procedures were performed under general anesthesia, with the patients in the supine position. The neck is slightly extended and the lesion-side arm is stretched out at 90°. The viewing monitor was placed above the patient's normal-side shoulder, with the surgeon and the camera operator standing at the lesion-side below the stretched arm (Fig. 1). A 2.5-cm-long incision was made parallel to the skin folds on the anterior axillary line of the lesion side and a subcutaneous skin flap from the axilla to the anterior neck area is dissected over the anterior surface of the pectoralis major muscle and clavicle by electrical cautery under direct vision. After exposing the medial border of the sternocleidomastoid muscle, the dissection is approached bluntly through the superficial space of the sternocleidomastoid muscle to reach the surface of the strap muscle above the ipsilateral lobe of the thyroid. Through this incision, a specially designed port device with multiple channels (Single Port-Covidien) was installed. To maintain a working space, CO2 was pumped into the cavity through the gas channel of the port and pressure was maintained at 7 mm Hg. Conventional trocars were used, including two 5-mm trocars and a 10-mm standard trocar. The three trocars were placed through the channels in an inverted equilateral triangular configuration, 1 cm apart, with the camera placed at the apex. A 30° 10-mm rigid laparoscope (Stryker Endoscopy) was used throughout the procedures. A grasper is inserted through one 5-mm trocar, while a Harmonic scalpel is inserted through the other 5-mm trocar for dissection (Fig. 2).

Team setup: S, surgeon; CO, camera operator; As, assistant; An, anesthetist; M, monitor.

Placement of the trocars.
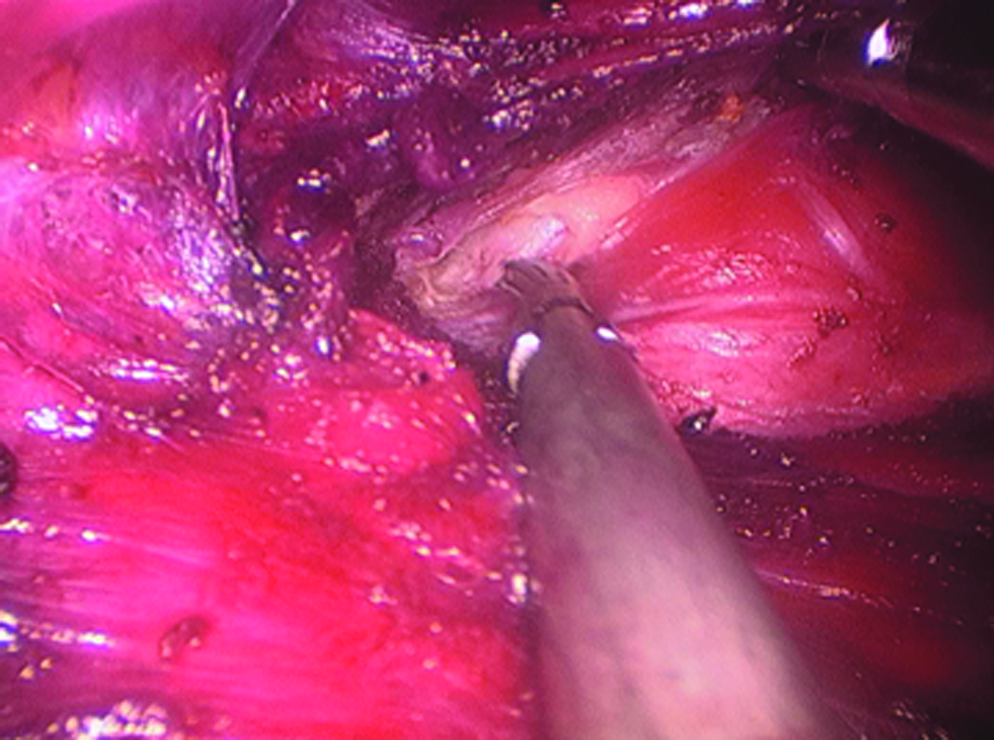
First, the Harmonic scalpel was used to widen the subcutaneous cavity between the platysma muscle and the strap muscle. Then, the lesion-side thyroid lobe was reached by vertical dissection of the strap muscle (Fig. 3). The operation proceeded in the same manner as conventional endoscopic thyroidectomy. All vessel dissections and ligations were performed using the Harmonic scalpel. Under endoscopic guidance, the lower pole of the thyroid lobe was drawn upward and medially using the grasper forceps, and inferior thyroid vessels were identified and individually divided. Then, the thyroid gland was retracted medially using the forceps, and the perithyroidal fascia is divided and sharply dissected using the Harmonic scalpel. Careful dissection was performed to identify the middle thyroid vein, and individual division was performed by Harmonic scalpel. Next, the upper pole of the thyroid was drawn downward and medially using the forceps, and superior thyroid vessels were identified and individually divided close to the thyroid gland to avoid injuring the external branch of the superior laryngeal nerve using the Harmonic scalpel (Fig. 4). Then, by approaching it from the inferior pole toward the superior pole, and from the lateral aspect of the gland moving gradually through the layers toward the trachea, the lesion-side thyroid was extirpated. Usually, the thyroid tissue near the tracheoesophageal groove should be preserved to prevent injury to the RLN. The resected specimen was extracted through the subcutaneous cavity to the skin incision (Fig. 5). Through the axillary incision, single drain was placed in the cavity left after careful lavage. The wound was closed cosmetically. The small incision scar in the axilla is completely covered when the arm is in its natural position.

Exposure of the thyroid.
Retraction of the thyroid and division of the superior thyroid vessels.

Extraction of the specimen through the subcutaneous cavity.
Results
All our patients were young women without prior neck surgery. There were no conversions to open or multi-incision endoscopic surgery. All patients were free of postoperative bleeding, dyspnea, RLN injury, hypocalcemia, and other complications. The median length of hospital stay was 1.75 days. The mean operative time for the entire procedure was 92.5 minutes (Table 2). Postoperative pain was assessed by visual analog scale. 2 The postoperative pain scores of the patients on day 1 were all 1/10 (Table 3). There were no wound infections in the cohort. Patients were uniformly pleased with the cosmetic results and less pain of the operation (Fig. 6). The follow-up period for the 4 patients was 4–5 months; until now, no significant complication was reported.

Postoperative axillary fossa incision.
Conventional endoscopic procedure: a retrospective analysis of the postoperative pain scores of the last 4 noncomplicated cases that underwent conventional three-incision endoscopic thyroidectomy dated before November 1, 2010.
Discussion
Conventional thyroid surgery today has reached a very high therapeutic standard and offers a very high level of safety,3,4 but it leaves a scar in the neck, which may be very visible in some people. To improve cosmesis, endoscopic techniques were developed.5–8 There are three likely directions of this evolution: expanded indications for the minimally invasive video-assisted thyroidectomy and parathyroidectomy, the further development of remote access surgery via several different routes, and the application of robotics to further assist the surgeon in accomplishing these techniques.
There have been numerous reports of remote access thyroidectomy using surgical ports placed in several locations including the anterior chest wall,9,10 subclavicular region, 11 or axillary region,12,13so that the scars are hidden by the patient's underwear. The axillary region has proved to be one of the most feasible approaches, although it requires patience and a particularly sophisticated skill set.
Remote access endoscopic thyroidectomy has always been cosmetic; however, it has not always been minimally invasive. The main reason for this is related to the requirement for adequate exposure of the lesion during the operation: when three ports are separately used on the thorax or breasts, three subcutaneous tunnels are formed within the anterior neck covering an area of at least 20 cm2. The 4 cases mentioned above were performed through a technique developed as an improvement on the previous endoscopic thyroidectomy. In these cases, the operations were done through a single tunnel with the incision placed below the armpit; therefore, a relatively smaller area of the subcutaneous tissue was dissected, causing fewer invasions and less postoperative pain when compared with the traditional three-incision technique of endoscopic thyroidectomy. The axillary incision was even more hidden, neatly achieving the double aim of minimal invasion and cosmesis.
During single-incision technique, the surgical instruments were placed close to each other, limiting their angles of movement and causing mutual interference or clashing of instruments, and therefore, the procedure was made relatively more difficult. In contrast, the operation time in this small series does not seem to be prolonged compared with conventional endoscopic surgery. This is due to the surgical team's extensive experience in single-incision laparoscopic technique, and also because this procedure requires less dissection of subcutaneous tissue compared to conventional endoscopic technique. Coordination between the surgeon and the camera operator in this procedure is vital; the endoscope viewing the operating field at a lateral angle and giving way to the main work instrument at the center of the field of view, coupled with minute adjustments by the surgeon and camera operator, should ensure smooth completion of surgery.
No postoperative bleeding occurred in these patients. The Harmonic scalpel was absolutely reliable in sealing the blood vessels where they were employed during endoscopic thyroidectomy. It is not imaginable to attempt endoscopic thyroidectomy without this device. There was no hypocalcemia detected in any patient. Measurement of calcium was not really a relevant parameter because all the cases enrolled were unilateral procedures, and thus, hypocalcemia would not even be possible. No RLN-associated complication occurred. Identification and handling of the RLN endoscopically is associated with a learning curve. In these preoperatively diagnosed benign lesions, we did not deliberately expose the RLN, and the thyroid tissue near the tracheoesophageal groove was also preserved to prevent injury to the RLN.
A clear disadvantage of this technique lies in the fact that we are dealing with a unilateral procedure. It is difficult to reach the opposite thyroid lobe by a single port in the axillary fossa. Gas is also required to maintain the space in this approach. Although there are many reports supporting the safety of CO2 insufflation into the neck,14–16 it does remain a point of controversy.
Single-incision endoscopic thyroidectomy is developing on the background of multiple-incision techniques and is an attempt to improve on the latter's cosmetic and minimal invasive values. The true essence of this procedure is not only replacing several incisions with a single one, but also combining the pursuit for cosmetic results and minimally invasive surgery into the field of thyroid surgery. Although robotic thyroidectomy is very well established and is becoming the new standard,17–19 the relative large and increased numbers of incisions of robotic surgery, high cost of robotic operation, and unavailability of robotic operation system in many countries limit the wide use of this technique. The author used conventional endoscopic instrument in accomplishing these four operations and is looking forward to develop new surgical techniques that are even less invasive, more cosmetic, and less painful.
Conclusions
Single-port access transaxillary totally endoscopic thyroidectomy appears to be safe and feasible. This technique may provide both an attractive way to reduce injury to the anterior neck tissue and a method for ideal cosmetic effect. Further studies are necessary to establish this technique as an accepted option in the endoscopic management of thyroid lesions in selected patients.
Disclosure Statement
No competing financial interests exist.