
Abstract
Abstract
Objectives:
The objective of this study was to describe use of the medial umbilical ligament (MUL) as a reinforcing flap to cover the internal ring (IR) during laparoscopic herniorrhaphy in children with indirect inguinal hernia.
Methods:
Laparoscopic high ligation of the IR was performed in a cohort (A) of 110 children with 140 indirect hernias between October 2001 and December 2004. We then developed “recurrence risk criteria” to explain four recurrences (2.8%). These criteria include previous recurrence, an IR ≥1.5 cm in diameter (anterior–posterior), and older children in their teenage years (13–18 years). From January 2005 to February 2010, we carried out similar repairs in 226 consecutive children (cohort B) with 307 indirect hernias, except that we reinforced the IR with an MUL flap if one of the three recurrence risk criteria were met (n=36). Of these children, 15 had an enlarged IR, 10 had recurrences, and 11 were teenagers.
Results:
The median patient age was 6.2 and 6.5 years in Groups A and B, respectively; there were four recurrences of 140 repairs (2.8%) in Group A, with a mean follow-up of 55 months (2–110 months). There were no recurrences in Group B including 36 MUL reinforcements with a mean follow-up of 32 months (5–74 months).
Conclusion:
Indirect hernias closed with our technique of laparoscopic high ligation of the IR will recur in 2.8% of children. Based on risk factors that we have developed, children prone to recurrence can be selected for MUL flap reinforcement of the IR, which may bring the recurrence rate close to zero.
Introduction
Materials and Methods
This study was approved by the ethical committee of the hospital for children. All laparoscopic herniorrhaphies were performed by 2 senior pediatricians.
From October 2001 to December 2004, 110 children with indirect inguinal hernias underwent laparoscopic ligation of the IR alone. Thirty cases were bilateral for a total of 140 repairs. From January 2005 to February 2010, laparoscopic ligation of the IR was carried out in 226 consecutive children; 81 were bilateral for a total of 307 hernias. Of these, 36 patients (including 15 children with an IR ≥1.5 cm in antero-posterior diameter, 10 with previous recurrences, and 11 teenagers) had their ipsilateral MUL detached and used as a flap to reinforce the IR of the involved side(s). The first 110 patients were allocated to Group A and the later 226 were in Group B. There were no patients with a recognized cause for increased abdominal pressure (cystic fibrosis and vengtriculo-peritoneal shunt).
The patients were placed supine in Trendelenberg position under general anesthesia. A 5-mm port and 30-degree laparoscope were introduced through the umbilicus and the capnoperitoneum of 10–12 Torr was created. The bilateral IRs were inspected.
One 3-mm (the finest tube we got) and a 5-mm (for needle holder) working port were inserted at the lateral borders of the rectus muscle at the level of the umbilicus. The diameter of the IR was measured with a fine plastic ruler (Fig. 1). Under telescopic vision, a 1.5-mm groin incision was made over the medial margin of the IR and an Endoclose needle (Ethicon Co.) with 2/0 prolene was introduced percutaneously and advanced medially beneath the peritoneum to pass a circumferential ligature avoiding the epigastric vessels. The needle skipped over spermatic vessels and vas deferens in the extraperitoneal plane with help of the forceps. At the nadir of the IR, the needle penetrated peritoneum into abdominal cavity and the prolene loop was released inside it (Fig. 2). Then the needle was reinserted laterally to regrasp the prolene (Fig. 3) and pulled out through the groin incision, where a knot was tied and buried, completing high ligation of the IR. The round ligament was included in the ligation in girls.
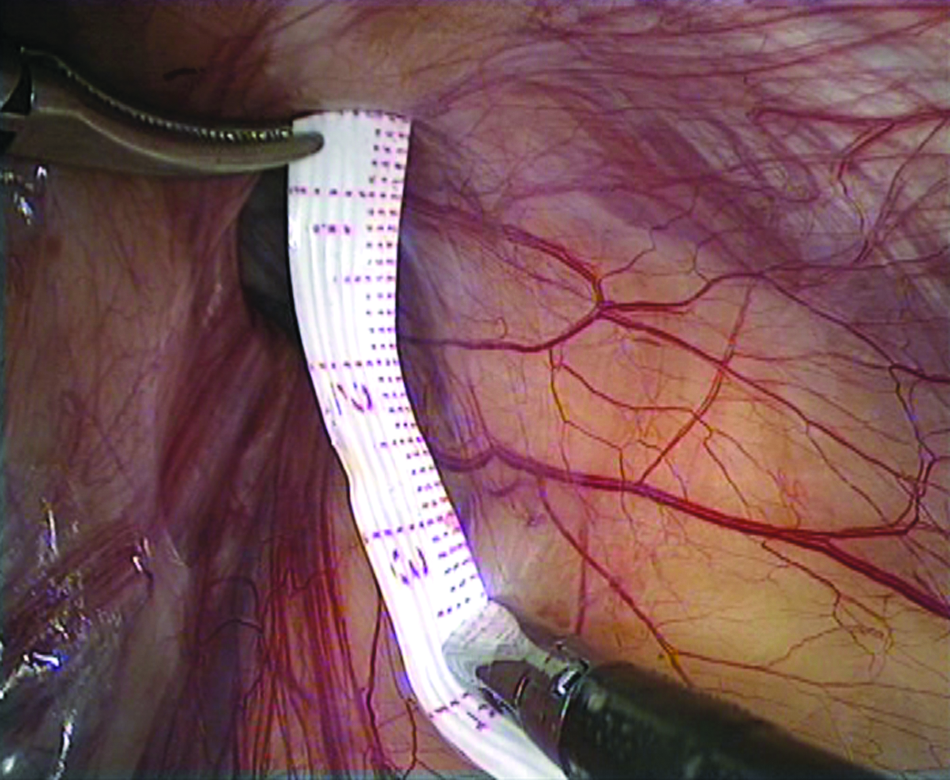
Measuring the size of IR in anterior–posterior diameter. IR, internal ring.
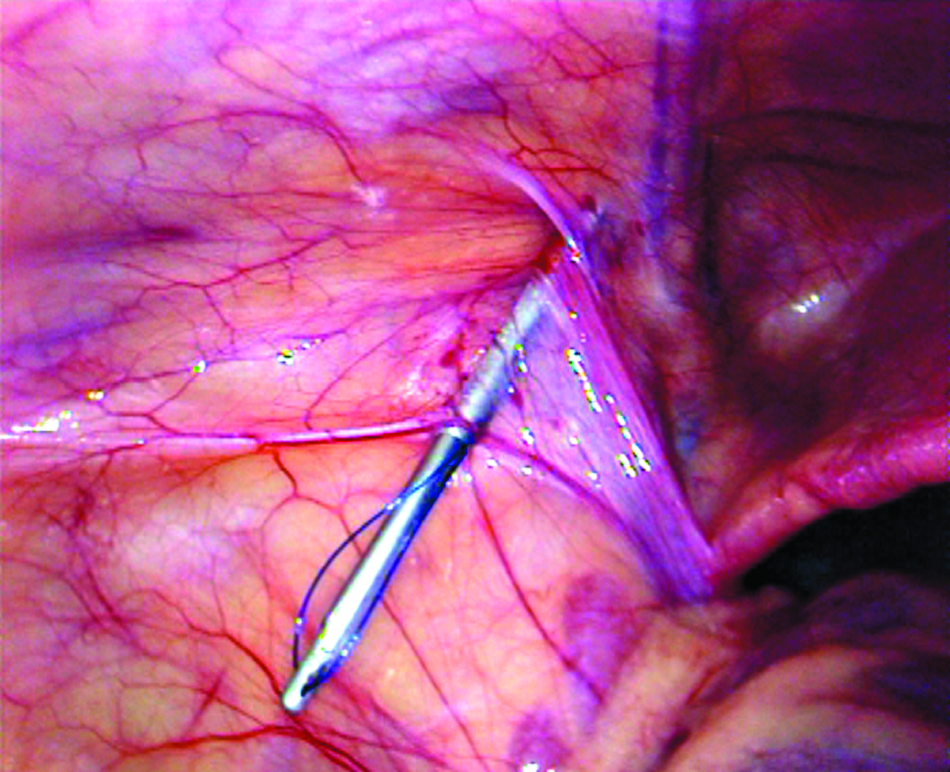
Endoclose needle with prolene advancing medially.
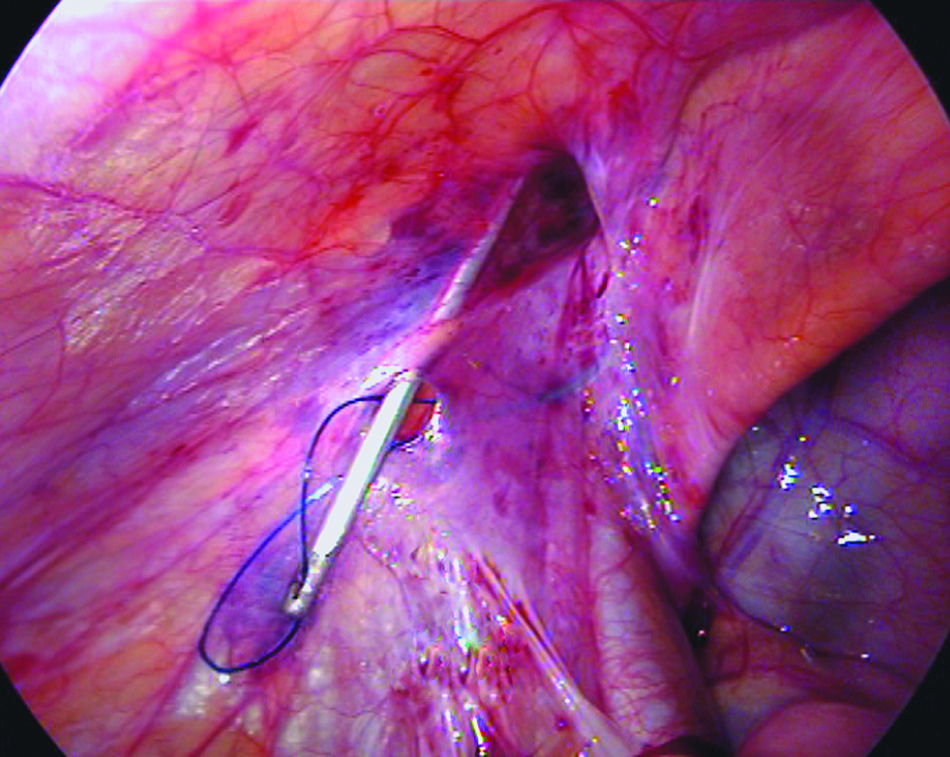
Regrasp of the prolene laterally.
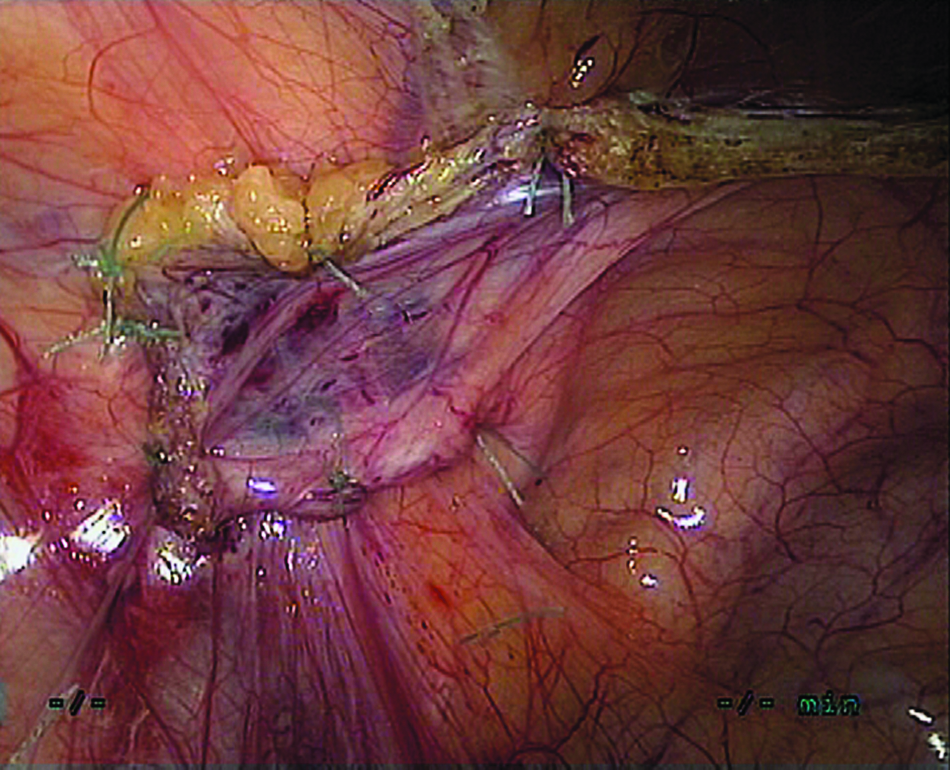
For 36 patients with risk factors for recurrence in Group B, the MUL was dissected from the undersurface of the anterior abdominal wall from the umbilicus back to Cooper's ligament and used as a flap to cover the ipsilateral IR (Fig. 4) by placing 6–8 interrupted 4/0 nonabsorbable polyviolene sutures (Surgical Specialties Corporation) at 1–2 cm intervals around the peritoneal margins of the IR (Fig. 5). The capnoperitoneum was then released and the ports were removed. Only the fascia of the umbilical incision was closed with an absorbable stitch and the skin wounds were closed using skin adhesive strips.
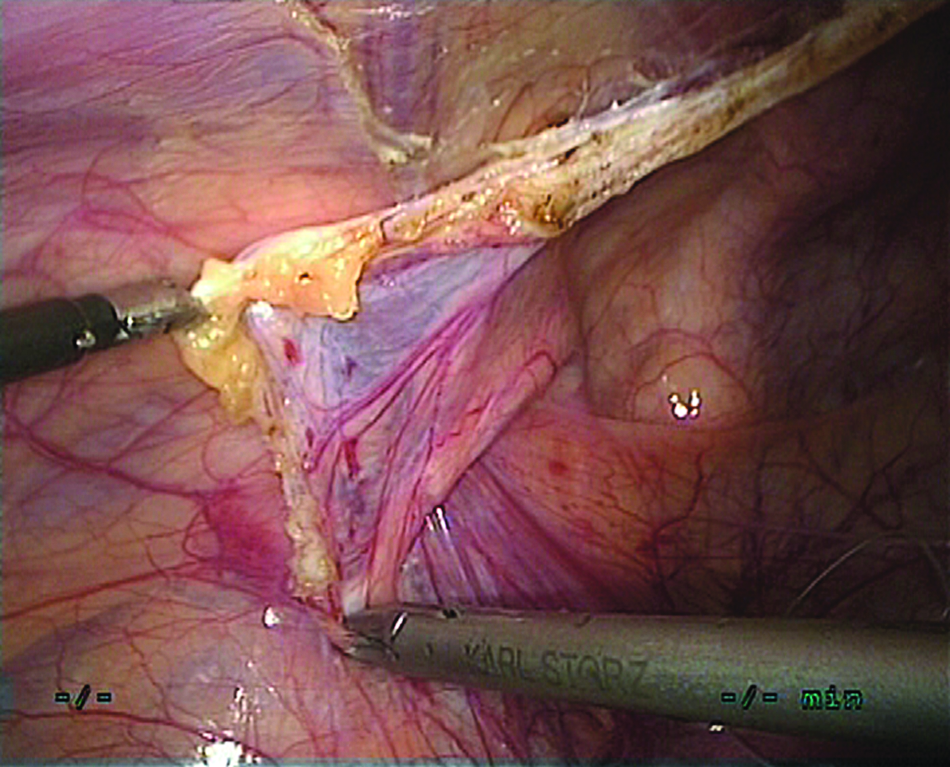
Medial umbilical ligament flap harvested and spread to cover the IR as reinforcement.
Medial umbilical ligament flap was fixed with peritoneum around the margin of IR.
All patients returned to visit the doctor at 1 week, 1 month, and 3 months after the operation. Approximately 97% patients received a subsequent phone call for long-term follow-up.
Results
The median operation times for laparoscopic high ligation of the IR only versus this operation plus MUL flap covering/reinforcing the IR were 15±9.3 and 47±11.5 minutes, respectively. Considering the difficulty to evaluate objective postoperative pain in children, we did not use visual analog scales or finger pain score model in our patients. The patients in the two groups had no difference in terms of postoperative pain, as they only stay overnight in hospital postoperatively. During a mean follow-up of 55 months (2–110 months), four recurrent hernias (2.8%) were found in Group A, two hernias recurred within half of a year and another two recurrences appeared between 1 and 2 years. No recurrence of hernia was found in Group B, with a mean follow-up of 32 months (5–74 months). There were no observed or reported cases of testicular atrophy during follow-up.
The demographics, surgery procedures, and recurrences of two groups are presented in Table 1. From the previous review documents and our experiences of laparoscopic pediatric inguinal hernia repair in Group A, the age group of teenagers, size of IR (≥1.5 cm), and previous recurrence in children were defined as three main risk factors for recurrence postoperatively.
IR, internal ring; MUL, medial umbilical ligament.
Videos of surgery accomplished in the two groups were reviewed. The risk factor distributions in the two groups are shown in detail in Table 2. The encouraging results from Group B presented no recurrences.
Discussion
Three risk factors for recurrence risk criteria defined
Of the 4 recurrent patients in first 110 cases, two recurrences happened in children with IR ≥1.5 cm in diameter within 6 months, another 1 child with previous recurrent indirect hernia, and a teenager with a recurrence at 1.5 years postoperatively. Most recurrent hernias in children are thought to be errors in technique—failure to identify or ligate the sac. 3 In our experience, there tended to be loosening of the knot in children with an IR ≥1.5 cm. 4 However, another potential cause is expressed by the metaphor “closing curtain with window left open”—a large defect/weakness in the transversalis fascia may persist behind the IR closure and contribute to its ultimate failure.
Ein et al. 5 reported that teenage recurrence rate (5%) was four times greater than the overall series (1.2%). For teenagers presenting with indirect inguinal hernias, we posit a component of musculo-fascial weakness including the inguinal floor, especially in hernias of long duration.
In boys with recurrent hernias, reoperations are difficult and careful dissection of dense fibrous tissue resulting from the previous surgery is mandatory. There is a definite risk of damaging the vas deferens and testicular vessels in the midst of the dense fibrous tissue. 6 To prevent injuring of these important structures during repair of a recurrence, it is easy to omit part of the circumference or tear the peritoneum at IR, resulting in small gaps between stitches, which may later contribute to recurrence. 7 These gaps usually occurred at the medial part of IR, which was the location of our recurrences. 8
Therefore, IR ≥1.5 cm, teenage presentation, and previous recurrence were considered as three risk factors for pediatric laparoscopic indirect hernia repair in our unit.
The deficiency of simple ligation of the IR
The principle for the repair of indirect inguinal hernia in children is high ligation of the IR. Although the laparoscopic approach theoretically provides high ligation of the IR more proximally than open repair, lower rates of recurrence have been reported with this approach. 9 In 6361 children with inguinal hernias operated on by 1 senior author, 1.2% recurrences were reported. 5 In our first cohort, 2.8% (4/140) had recurrence. De Lange et al. 10 advocated that a hernioplasty is necessary for the children with insufficient IR in open repair. A similar initial conclusion may be drawn in laparoscopic approach: the procedure of simple laparoscopic ligation of the IR is not sufficient enough for all the children; some require reinforcement of the IR.
Ligation of the IR combined with MUL flap covering the IR is a reliable herniorrhaphy procedure for children with risk factors and teenagers
Sneider et al. 9 proposed that limiting elective pediatric laparoscopic hernia repair to <6 years old would decrease recurrence rates; we chose to improve the procedure rather than limit patient selection. Pursuing more reliable laparoscopic repair in infants younger than 18 months, Endo et al. 11 advocated double ligation of hernia sac to secure the laparoscopic ligation of the IR. Yip et al. 12 developed a flip-flap hernioplasty to improve laparoscopic pediatric hernia repair. We suspect that the lack of reinforcement of the IR is a common shortcoming of these procedures.
MUL flap covering the IR as a reinforcement developed in this study provides a reliable defense against recurrence of indirect hernia. The MULs are remnants of obliterated umbilical arteries composed of a fibrous cord and a peritoneal membranous web—a double peritoneal membrane between the cord-like MUL and peritoneal surface of anterior abdominal wall. 13 High ligation of the IR combined with a reinforcement of MUL flap provided excellent postoperative results. Twenty-five young children with risk factors and 11 teenagers with inguinal hernias underwent laparoscopic ligation of the IR combined MUL flap covering the IR; no recurrence in Group B (0 in 307 repairs) suggests the effectiveness of the procedure. Although the procedure of MUL flap covering IR would take about 30 minutes longer, the “zero” recurrence made the additional procedure well deserved. As the laparoscopic suturing maneuvers improved, the operating time would be shorter.
Advantages of laparoscopic MUL flap covering the IR
The MUL is located on the medial part of femoral ring and IR, arising as a branch of internal iliac artery and ending at the umbilicus. The ipsilateral umbilical ligament is easily dissected off the abdominal wall and spread to cover the femoral ring and IR in a tension-free way. The MUL flap provides reinforcement for the IR as well as the femoral ring. 2 The immediate postoperative result was satisfactory and postoperative pain was not serious than that in high ligation of the IR. A mean follow-up of 32 months confirmed zero recurrences in Group B.
The IR was reinforced by a flap of native tissue instead of synthetic mesh in the study. Partrick et al. 14 reported no recurrences in his series of 35 teenagers with an indirect inguinal hernia repair using a polypropylene mesh plug inserted in IR and a similar mesh onlay covering the posterior wall. Considering the unfavorable effects of synthetic mesh in male patients, 15 the autologous MUL flap is preferred and adopted without any adverse effects on male fertility.
In addition, an MUL flap covering ipsilateral IR plays an important role in strengthening the defense against recurrence of indirect hernias by keeping the inguinal channel in tilt position and the hernia sac collapsed whenever under the stress of intra-abdominal pressure.
Of course, not every child needs to undergo the reinforcement procedure. With our experiences, the children with risk factors discussed earlier and teenagers are recommended.
Conclusion
Laparoscopic high ligation of the IR combined with MUL flap covering the IR as reinforcement for indirect inguinal hernia in selected children and teenagers is a feasible and effective procedure that may bring the recurrence rate of pediatric laparoscopic herniorrhaphy close to zero.
Footnotes
Acknowledgment
The authors thank Dr. Baird Mallory, Medical Director of Maine Medical Partners–Pediatric Surgery, for his constructive idea in making this manuscript more practical and for his generous revision and editorial help with the manuscript.
Disclosure Statement
No competing financial interests exist.
An abstract of this work was presented at the 6th International Congress of the Asia-Pacific Hernia Society (APHS) in Seoul, Korea, October 16, 2010.