
Abstract
Abstract
Introduction:
Nonanatomical tumorectomy that includes the lesion is commonly performed for the malignant tumor located at the segment 5 (S5) of the liver. Although anatomical resection has theoretical advantages, anatomical S5 segmentectomy is a technically demanding procedure, and it becomes more difficult if it is performed laparoscopically. We report here on laparoscopic anatomical S5 segmentectomy using the Glissonian approach.
Patients and Methods:
A 53-year-old man was admitted for a hepatic mass that was incidentally found on a health screening test. The laboratory studies show negativity for viral markers and a normal level of alpha-fetoprotein level. The preoperative liver function was Child-Pugh class A. Abdominal computed tomography revealed a 5.2-cm mass that was located in segment 5. The lesion shows enhancement on the arterial phase, which was washed out on the delayed phase. Laparoscopic anatomical S5 segmentectomy was planned with the preoperative diagnosis of hepatocellular carcinoma.
Results:
The operative time was 300 minutes. The estimated intraoperative blood loss was about 300 mL, and an intraoperative transfusion was not necessary. The postoperative pathology confirmed a 6.0 × 4.5 × 3.0-cm neuroendocrine carcinoma with a cholangiocarcinoma component. The patient was discharged on the 9th postoperative day without any complications.
Conclusion:
This case shows the feasibility of performing laparoscopic anatomical S5 segmentectomy.
Introduction
Recently, the number of reports on laparoscopic liver resection has rapidly increased.6–8 Although laparoscopic liver resection is technically demanding, the procedure has been applied to more difficult procedures such as posterior sectionectomy and central bisectionectomy.9–14 Adapting the Glissonian pedicle approach can be useful for these anatomical major liver resections.11,15–17 However, even with the recent developments of laparoscopic major liver resection, there are still few report on laparoscopic anatomical monosegmental resection on the right side of the liver. 18 Herein, we report on a case of a total laparoscopic anatomical segment 5 (S5) segmentectomy using the Glissonian pedicle approach. To the best of our knowledge, this is the first report on this procedure.
Case Report
Patient
A 53-year-old man was admitted for an incidentally detected hepatic mass on a health screening test. The patient had a history of hypertension and alcoholic liver cirrhosis. The physical examination was unremarkable. The laboratory studies showed negativity for hepatitis B and C viral markers and a normal alpha-fetoprotein level (2.5 IU/mL). The preoperative liver function was graded as Child-Pugh class A and the indocyanine green retention rate at 15 minutes was 9.0%. The levels of total bilirubin, aspirate aminotransferase (AST), and alanine transaminase (ALT) were within the normal ranges. Abdominal computed tomography revealed a 5.2-cm single-nodular tumor that was located in S5 with enhancement on the arterial phase and washing out of the enhancing lesion on the delayed phase (Fig. 1). The preoperative diagnosis was hepatocellular carcinoma (HCC). We then performed laparoscopic anatomical S5 segmentectomy.
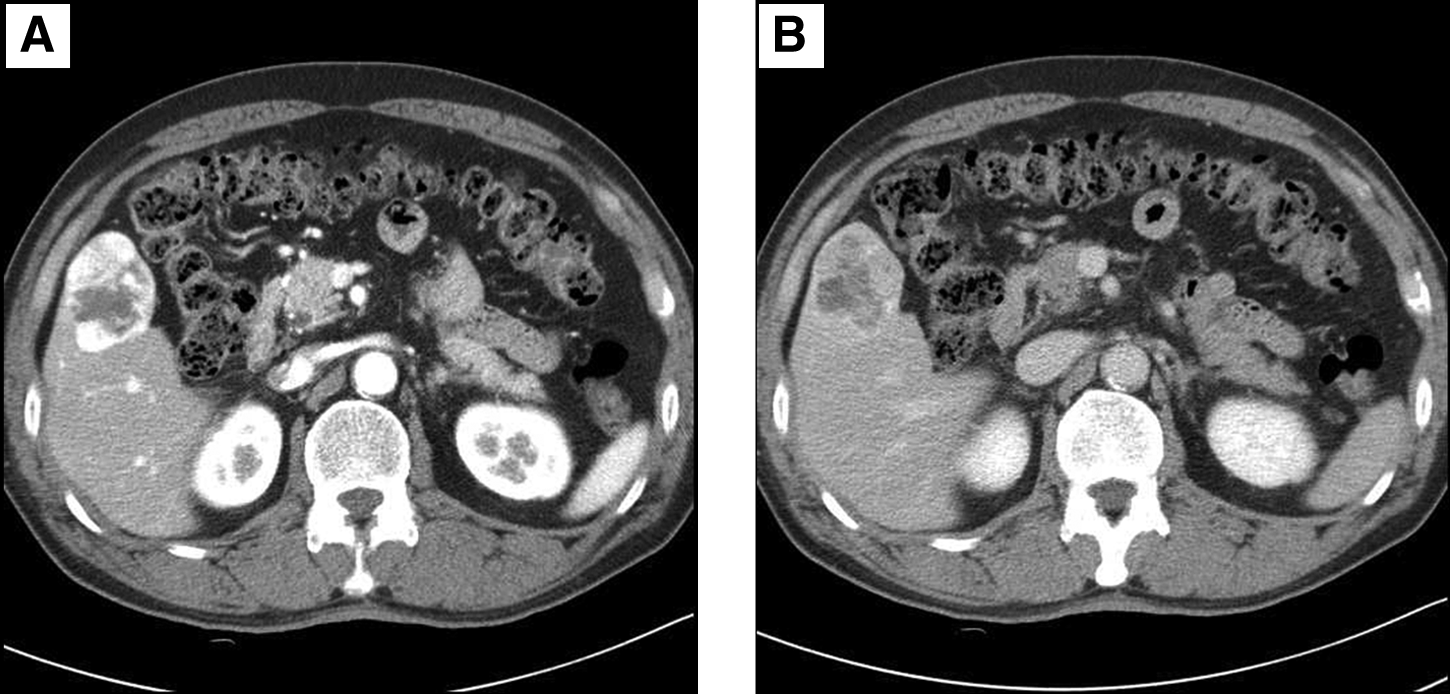
Abdominal computed tomography shows a 5.2-cm single nodular tumor with enhancement during the arterial phase
Operative technique
Under general anesthesia, the patient was placed in the lithotomy position with a right-side-up adjustment. A pneumoperitoneum was created with the insufflation of CO2 through a 12-mm umbilical port, and the intra-abdominal pressure was maintained below 12 mmHg. Four additional ports (one 12-mm port, two 10-mm ports, and one 5-mm port) were placed, as shown in Figure 2. A flexible laparoscope (Olympus, Tokyo, Japan) was used. After performing a cholecystectomy, intraoperative ultrasonography (USG) was performed to confirm the location of the tumor and its relationship with the adjacent structures. The Glissonian pedicle to the right anterior section was then isolated by meticulous dissection (Fig. 3). With a temporary clamp of the right anterior Glissonian pedicle, the ischemic margin of the right anterior section was marked with electrocautery. Transection of the liver parenchyma at the medial margin was started. The superficial hepatic parenchyma was transected using a Harmonic Scalpel® (Ethicon Endo-Surgery, Inc., Cincinnati, OH), and the deeper portion of the parenchyma was transected using a laparoscopic CUSA® (Valleylab, Boulder, CO). The right anterior Glissonian pedicle was further dissected peripherally while the liver was retracted ventrally. The Glissonian pedicle to S5 was isolated (Fig. 4) and the discolored S5 area was marked with electrocautery after temporary clamping of S5 Glissonian pedicle. The S5 Glissonian pedicle was then divided between Hemo-lock clips (Weck Teleflex Medical, Research Triangle Park, NC). Transection at the lateral and superior side of the S5 was then performed. The small branches of the hepatic vein that were encountered during the parenchymal dissection were divided between 5- or 10-mm Hemo-lock clips or LigaSure® (Valleylab). Once the resected specimen was completely divided, it was inserted into a vinyl bag and extracted though an extended incision of the subumbilical port. After careful hemostasis, fibrin glue (Greenplast®; Green Cross Corp., Seoul, Korea) was applied to the raw surface. After irrigation of the surgical field, a drain was inserted and the wound was closed in layers.

The position of the trocars.
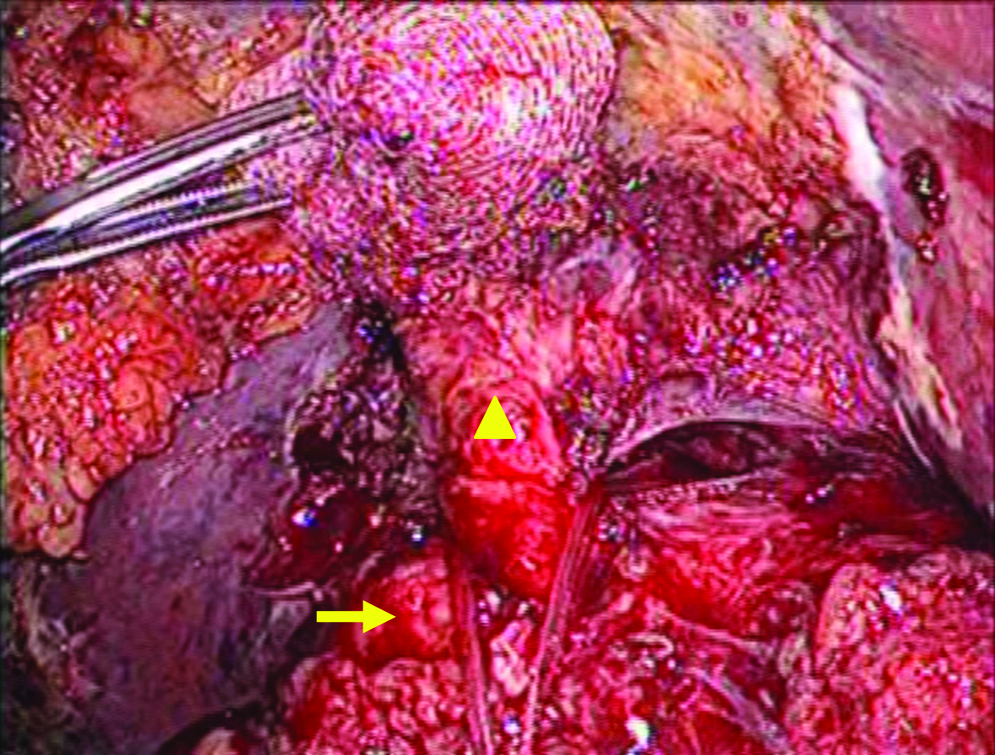
Laparoscopic view of the dissection of a right anterior (arrowhead) and right posterior Glissonian pedicles (arrow).
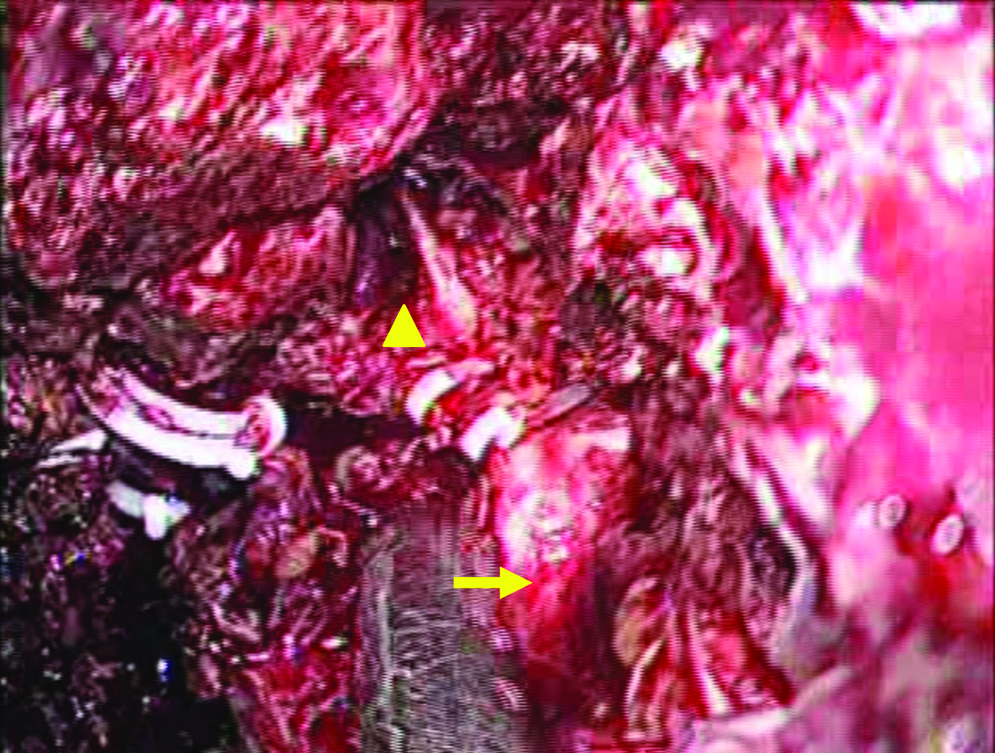
Laparoscopic view of the S5 Glissonian pedicle (arrowhead) from the right anterior Glissonian pedicle (arrow).
Results
The operative time was 300 minutes. The estimated intraoperative blood loss was ∼300 mL and an intraoperative transfusion was not necessary. On the postoperative first day, the levels of AST and ALT were slightly increased (AST, 179 IU/L; ALT, 217 IU/L) and they became normalized on the postoperative seventh day. The levels of total bilirubin were maintained within the normal range during the postoperative period. The follow-up computed tomography on the seventh postoperative day showed no congestion or ischemia in the remnant liver (Fig. 5). The postoperative pathology confirmed a 6.0 × 4.5 × 3.0-cm neuroendocrine carcinoma with a cholangiocarcinoma component and a 6-mm tumor-free resection margin (Fig. 6). The patient was discharged on the ninth postoperative day without any complications.

The postoperative computed tomography scan shows no abnormal findings in the remnant liver with preservation of the right posterior pedicle.
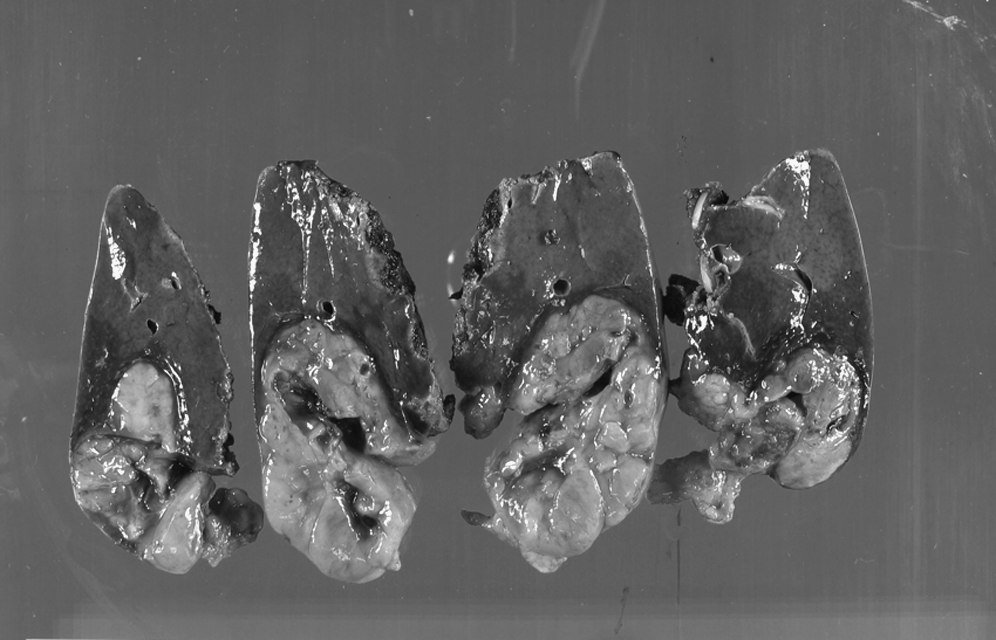
Photography of the resected specimen.
Discussion
As the malignant liver tumor is frequently associated with liver cirrhosis or chronic liver disease, it is desirable to minimize the volume of resection and save as much liver volume as possible. This strategy applies not only to open liver resection, but also to laparoscopic surgery.
When the tumor is located in S5 of the liver, there are several options that can be chosen for operative treatments. One is anatomical major resection such as right hemihepatectomy, right anterior sectionectomy, and central bisectionectomy. Although the above procedures are all anatomical resections, there are possible disadvantages that the resections of a significant liver volume may jeopardize the already compromised liver function and lead to hepatic failure when the liver function of the patient is already poor. Another option is nonanatomical S5 resection, the so-called tumorectomy or wedge resection, which is relatively simple and widely performed. The remaining option is anatomical segment V resection. Although there is still debate about the survival outcomes of anatomical resection compared to that of a nonanatomical one, anatomical liver resection has potential advantage in that all the tumor bearing area, including the portal pedicle, can be eradicated anatomically.1,2,4
There are two methods for anatomical liver resection. The selective dye injection method is a well-known procedure. 1 This requires precise dye injection to the portal branches under the guidance of intraoperative USG. However, this method is difficult to apply to laparoscopic surgery because the precise handling of needles and USG is limited in this situation. The Glissonian pedicle approach is another way of performing anatomical liver resection. Machado et al. reported straight-forward control of the Glissonian pedicle without hilar or parenchymal dissection using small incisions around the Glissonian pedicle. 15 The Glissonian pedicle can be clamped with the surrounding liver tissue by precise localization of the clamp through a small incision of the liver parenchyma and this maneuver could simplify the procedure and minimize bleeding.15,18 In contrast, our method is complete isolation of the Glissonian pedicle with meticulous dissection. 17 The Glissonian approach is a useful way of performing anatomical segmental resection of the liver, as was shown in this study. In addition, this method can be used in major liver resection as hemihepatectomy when the tumor is far apart from the hilar area.
The major concerns about laparoscopic S5 segmentectomy are how to precisely maintain a proper transection line. A proper transection line ensures a safe resection margin and preserves the vascular structures that drain to the remaining liver. Injury to these vascular structures can lead to troublesome bleeding, ischemia, or congestion of the remnant liver. Because there are no anatomical landmarks for S5 segmentectomy, selective isolation of the Glissonian pedicle to the S5 segment is crucial in anatomical S5 segmentectomy. Isolation of the S5 Glissonian pedicle requires two steps. First, the right anterior Glissonian pedicle is carefully isolated at the hepatic hilum. With temporary clamping of the right anterior Glissonian pedicle, the medial and lateral margins of the right anterior section can be identified. With further dissection of the right anterior Glissonian pedicle in the peripheral direction along with concomitant parenchymal transaction, the S5 Glissonian pedicle can be isolated. By clamping the S5 Glissonian pedicle, the anatomic S5 area can be delineated.
This case demonstrated that laparoscopically isolated S5 segmentectomy is a feasible operative procedure for selected patients, and especially for patients with limited liver function. Careful dissection and control of the S5 Glissonian pedicle can be done in a stepwise fashion and it makes laparoscopic isolated monosegmentectomy as feasible an operation as liver surgery by the open method.
Footnotes
Disclosure Statement
No competing financial interests exist.