
Abstract
Abstract
Background:
Laparoscopic Roux-en-Y gastric bypass (LRYGB) is associated with a significant learning curve. We report the results of a systematic training program from a high-volume bariatric center measuring the outcome by comparing the results with data from a consecutive series of 1000 fast-track LRYGB.
Methods:
Using a stepwise training program, the Roux-en-Y gastric bypass operation was divided into an upper and lower procedure and subdivided into 11 well-defined steps. A laparoscopic surgeon without experience in upper-gastrointestinal surgery was mentored by an experienced bariatric surgeon. During 6-month full-time fellowship, 300 operations were performed.
Results:
The trainee surgeon performed 61 upper procedures and 121 lower procedures in which the mentor surgeon did the other part of the operation. In 110 patients, the trainee performed both procedures. Two percent had perioperative complications compared with 1% of 1000 patients. All were repaired and had an uneventful recovery. Two percent had postoperative complications <30 days compared with 2.8% in the clinic. In the trainees series, there were no leaks compared with 1% in 1000 patients. Operative time was 56/55/70 minutes for operation 0–100/100–200/200–300 compared with an average of 47 minutes registered in the clinic. Concerning time to discharge, there was no difference between patients operated by the trainee and the standard of the clinic.
Conclusion:
Using a systematic training program in LRYGB surgery eliminates morbidity of the learning curve without affecting the volume.
Introduction
Our purpose was to create the possibility for a new surgeon to do safe LRYGB in a high-volume unit as a 1-surgeon procedure. In this article, we report our experience and results from a high-volume training program involving 300 LRYGB during a mentored 6-month fellowship program, in which a surgeon with no previous experience in laparoscopic upper-gastrointestinal (GI) surgery was mentored by an experienced bariatric surgeon. The outcome was measured by comparing with the results of a consecutive series of 1000 fast-track LRYGB performed by the mentoring surgeons of the same institution.
Materials and Methods
The clinic
The Bariatic Center of Private Hospital Moelholm was founded in 2006 by a very experienced bariatric surgeon (J.F.L.). All patients underwent fast-track surgery, which includes mobilization within 2 hours after surgery, no tubes or drains, and discharge within 24 hours after operation.
Facts about surgeons
The trainee (T.S.) was an experienced laparoscopic colorectal surgeon with previous experience in colorectal, inguinal/ventral hernia repair and gall bladder surgery, but no previous experience with laparoscopic stomach surgery except suturing of perforated ulcers. The mentor was a very experienced upper-GI surgeon who had performed >1500 laparoscopic RYGB procedures.
Facts about the surgery and the fellowship program
The LRYGB learning program consisted of a 6-month full-time fellowship with mentored operations every day. The idea was to learn LRYGB step by step, by dividing the operation into an upper and a lower procedure with subdivision into 11 well-defined and graduated parts (Table 1). The vision was that the complication rate, the time of surgery, and the surgical volume of the clinic should be unaffected by the program. The standard operative time for LRYGB was 47 minutes in the clinic, and during the fellowship program, 15 minutes were added for each scheduled trainee operation, making it possible to keep patient flow constant. Before each operation, it was decided which step each surgeon would do. In cases of difficulty, the mentor shortly demonstrated how to manage the situation, after which the trainee continued the procedure as planned.
Operative details
Using four 12-mm port and one 5-mm port, access to the bursa omentalis was obtained by dissection of the minor omentum approximately 4 cm distally to the cardia using the Harmonic scalpel. A pouch less than 30 mL was created by dividing the stomach with a 45- and 60-mm linear stapler using blue cartridges in the direction of the angle of His. In cases of a large omentum, it was divided in a longitudinal direction. After identifying the ligament of Treiz, a biliary limb of 75 cm was measured, and an ante-colic, ante-gastric gastro-jejunostomy was created using a linear stapler with a 45-mm blue cartridge. The remaining opening was closed by a continuous 3-0 vicryl suture in two layers. A 150-cm Roux limb was measured, then the jejuno-jejunostomy was created using a 45-mm linear stapler with a white cartridge, and the remaining opening was sutured with a 3-0 vicryl suture in two layers. A small opening was made in the intestinal mesentery between the gastro-entero anastomosis and the entero-entero anastomosis and the intestine above it was divided, thereby turning the omega loop into an ante-colic ante-gastric Roux-en-Y. Finally, a suture was placed at the top of the staplerline at the gastro-jejunostomy to decrease any tension on the gastro-jejunostomy. Leak test was performed with a swap behind the anastomosis and methylene blue injection through a gastric tube. Finally, all ports were removed under visual inspection and pneumoperitoneum was desufflated.
Mentoring details
In the first 10 procedures, the trainee only sutured the jejuno-jejunostomy, and the mentor performed the other parts of the operation. In the next 30 cases, the trainee also did the stapling of the anastomosis, thus commencing the whole lower step. After this, he started doing the upper step in every second operation, thereby shifting with the mentor. In cases of difficulty (perigastric fat, high body mass index [BMI], technically difficult cases), the mentor shortly demonstrated how to manage the problem, and then the trainee continued the operation. This two-step procedure was followed to operation no. 190, and then the trainee started doing the whole procedure using 2 nurses as assistants.
Facts about the patients
In the last 110 operations where the trainee did the whole procedure, only female patients were selected and super-super obese patients were not included. All patients underwent preoperative clinical investigation by an endocrinologist experienced with obesity cases, the surgeon, and a dietician. To reduce the intraabdominal fat and reduce complications, the patients were scheduled to lose 8%–10% of the primary weight and the date of the operation was planned. They stayed in close contact with the dietician who supervised the preoperative weight loss. All patients were supposed to be discharged on the first postoperative day. The patients were followed by phone at 1 and 4 weeks postoperatively and seen at the clinic at 4 and 12 months postoperatively, subsequently followed yearly by questionnaire. All data were entered prospectively in the obesity database at Private Hospital Moelholm.
Results
Three hundred patients underwent laparoscopic RYGB in the 6-month fellowship period (Table 2). The results were compared with the results prospectively registered in the database of the clinic of a consecutive series of 1000 procedures. The median age was 40 and the median BMI was 44.3 among 246 female and 54 male patients. Concerning the preoperative risk, there was no difference between the groups. In the trainee group, there were 281/19 ASA II/III patients. Twenty-three percent had diabetes (medically treated) and 34% had medication because of hypertension. Sixteen percent of the patients had previous upper-GI surgery and 43% had previous lower-GI surgery. The trainee performed the upper procedure in 61 cases and the lower procedure in 129 cases and did all steps in 110 cases (Table 3).
Median (range).
American Society of Anesthesiologists classification.
HglA1C > 0.063 and/or antidiabetic medical treatment.
Trainee and mentor performing different parts of the procedure.
Trainee doing the whole procedure.
The operative time increased from 56 minutes in operations 0–100 wherein the mentor did one part of the operation to 70 minutes during the last 110 operations wherein the trainee did all steps in the operation assisted by 2 nurses compared with the mentor's average operative time of 47 minutes (Fig. 1). Two percent had perioperative complications compared with 1% in a series of 1000 patients (Table 4). Four patients needed reoperation, of which 2 had intraperitoneal bleeding, 1 patient had a stenosis of the jejuno-jejunostomy, and 1 had a lesion on the small intestine. All were repaired and had an uneventful recovery. Two underwent gastroscopy because of internal stapler bleeding. There were no conversions and no cardiopulmonary events in either series. Two percent had postoperative complications at <30 days compared with 2.8% of the consecutive series of 1000 patients (Table 5). In the trainee series, there were no leaks compared with 1% in the clinic.
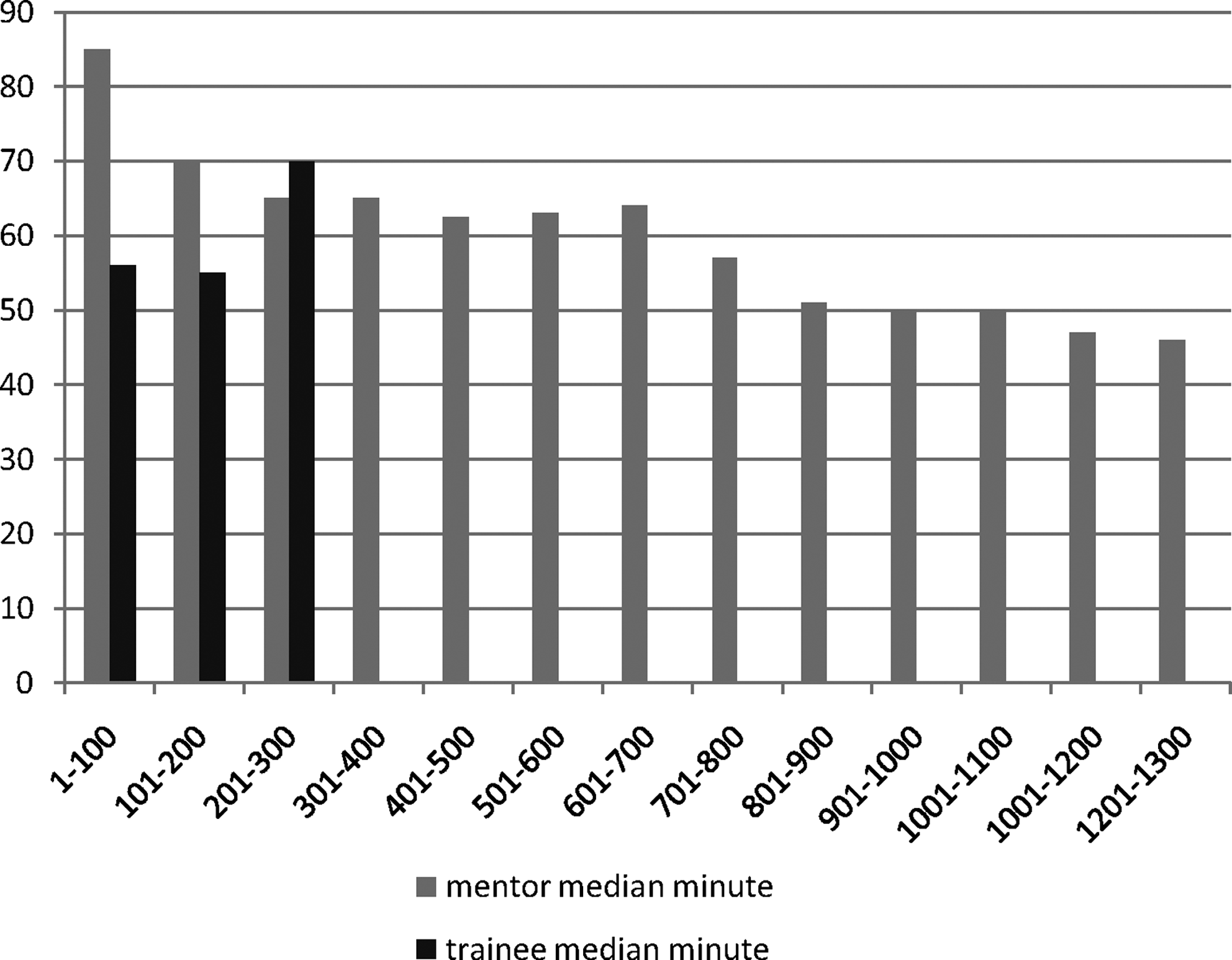
Operative time of mentor and trainee.
Within 30 days, 1 patient presented with a marginal ulcer that was treated with proton pump inhibitors (PPI) and 1 patient was diagnosed with an abscess at the gastro-jejunostomy, which did not require operation (Table 5). Concerning time to discharge, there was no difference between patients operated by the trainee and the standard of the clinic (Fig. 2). Follow-up data from all patients in our database were checked with our national patient registry, thus securing a complete follow-up.
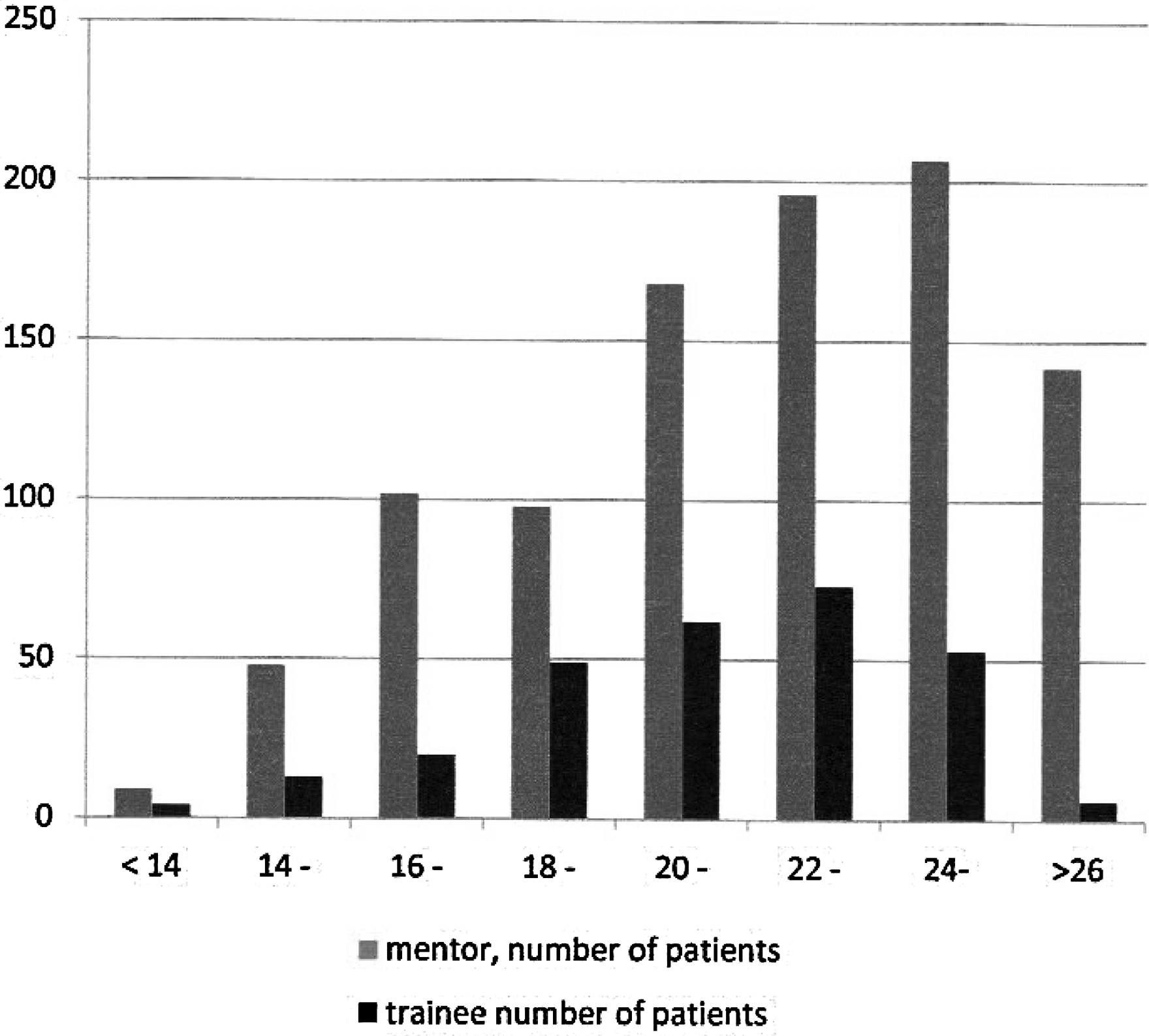
Time to discharge after laparoscopic Roux-en-Y gastric bypass (hours).
Discussion
The main finding of our structured bariatric fellowship program was that it was possible to eliminate learning curve-related morbidity using a systematic mentoring strategy in which a new surgeon was gradually introduced to the different steps in LRYGB. Combining a very specialized bariatric surgeon with a highly motivated laparoscopic trainee in a full-time fellowship program at a high-volume center resulted in morbidity and complication rates much comparable or lower than those previously reported.4,14,15 The trainee was taught stepwise to do the operation, ending up managing the whole procedure as a single surgeon, using only nurse assistants without affecting the operative time or the volume of patients in the clinic. The two-consultant approach has been used by others 16 ; however, our detailed strategy with a planned stepwise introduction has not been previously described, and to our knowledge, nurse assistants have not been reported to be the standard in any other institution.
It is well known that learning curve-related complication rates may be as high as 26%.4,17,18 This has prompted several institutions to develop training programs, leading to a substantial decrease of learning curve-related complication rates (ref. 6 [8%–13%], ref. 12 [7%–13%], ref. 13 [18%–23%], and ref. 19 [14%]). Compared with these data and the largest prospective studies available,3,20 our complication rates of 2%–3% are very low. We believe that the main reason for this is the high volume of our clinic, with up to 12 LRYGB per day.
As previously shown, in LRYGB surgery it is well documented that low-volume surgeons/hospitals are associated with substantial higher risk of complications for the individual patient.21,22 During our training program, the possibility of doing the same operation every day within a limited timeframe made it possible for the trainee to remember and correct yesterdays faults, thus acquiring the abilities to do the procedure in a fast and safe way.
The conditions for our program was a high-volume clinic, an efficient organization with well-defined tasks for the whole surgical/anesthesiological team, careful patient selection during the first period of the trainee's individual surgery (female, not super-super obese), high motivation of the fellow and the staff, as well as interpersonal respect and good humor between the trainee and the mentors. The ability to give and gain surgical expertise during training demands meticulous planning of the procedure in which every step of the operation is described, and the expectations between the mentor and the trainee is thoroughly discussed and agreed upon before starting the program. The staff should be very familiar with the fellow and his/her abilities and introduced to the strategy as early as possible. The trainees should be very much aware of their abilities and limitations when confronted with a new potential difficult procedure such as LRYGB, with a willingness to abandon old “surgical habits” if they are found inappropriate when performing surgery in a new area.
Setting the ports at the right place and angle is the first step to success, and this was trained and discussed from the start to give the trainee a systematic approach when measuring out where the ports should be placed. When learning a new procedure, one should always attend the easy part first with the lowest risk of complications, which is why the trainee started to train suturing the jejuno-jejunostomy. However, this may as well be a challenge in cases where there is tension on the anastomosis, bleeding or twisting from stapler lines, protrusion of the mucosa, secretion of the bowel, a large defect to suture, difficult access, etc, and this was the first step where the mentor demonstrated how to suture a difficult anastomosis in a safe way. Repeating this over and over again, the trainee gradually acquired the ability to suture different defects with correct placement of the sutures, avoiding the risk of stenosis or leaks. Safe handling of the bowel with graspers was trained meticulously and the trainee was given multiple small tricks to avoid any lesion or ineffective movements when measuring out lengths of the bowel limbs. Dissection of the pouch may be challenging when the cavity is small or the stomach is covered in adipose tissue. Focus of dissection in the correct direction toward the angle of His avoided any dissection into the mediastinum with subsequent risk of an esophageal lesion or lesion of the splenic hilus.
The operative time was kept within the schedule with 15 added minutes. Compared with the mentors first 300 operations, it was even lower, but this just reflects the efficiency of mentoring, as the mentor did not have any mentoring himself when starting to do LRYGB. However, our operative time was considerably shorter throughout the program than that reported by others,10,14,19,23 thus reflecting the mentor's experience and the ability to adopt not only the technical aspects of how this surgery is performed, but also the time to do it as well. The risk of cardiopulmonary complications during long-time pneumo-peritoneum in bariatric surgery is well known 24 and the importance of keeping a short operative time was demonstrated by the fact that we did not have a single cardiopulmonary complication. Apart from the surgery itself, the short operative time reflected a very close cooperation with the anesthesiologist and the assistants, each having their own screen making it possible for them to follow and foresee each step in the operation, thereby being ahead of the surgeon by providing instruments, tubes, or swaps instantly without any delay. Our experience is that a well-trained committed nurse assistant is invaluable when performing advanced laparoscopic surgery, because often they do have profound knowledge of the surgical equipment at hand and may therefore contribute with technical solutions to solve surgical challenges in difficult cases. They were involved in the fellowship program and the importance of using this gradual approach was reflected by the fact that the patient flow and the operative time were almost unaffected by the training program.
The high volume of patients made it possible for the trainee to see all kinds of solutions to variations encountered, such as unexpected position of the ligament of Treiz; short small bowel mesentery creating tension on the gastro-jejunostomy; handling of adhesions toward omentum, bowel, spleen, abdominal wall, etc; malrotation; hiatal hernias; or handling of a large liver.
The efficiency of the program was high seen from the organization and the fellows' point of view. LRYGB is a demanding procedure with a lot of pitfalls. Small errors may convert an easy operation into a major challenge and the need to clearly discuss and introduce the procedure stepwise has not been systematically described in any article. Selecting the right surgeon to do a new procedure may be a future challenge in any surgical clinic. Surgical trainees can be trained and tested in virtual trainers as abilities from these are transferable to the physical reality before attending live surgery, 25 just as airline pilots are tested before being allowed to sit behind any steering wheel. With a subsequent use of a mentoring surgeon, surgical skills can be further developed in the clinic. As a trainee and mentors, we had very clear expectations from one another as to how each operation should be performed, who should do which step, and how to manage difficulties.
In our experience, selection of the right patients during training is very important. Male patients have a higher BMI, the omentum may be very large, the small mesenterium may be short, and dissection of the pouch may be very difficult as the upper cavity and the distance to the angle of His may be deeper than expected. Thus exclusion of super-super obese patients and male patients in the program made it possible to acquire the necessary surgical skills without increasing morbidity, and presently, the trainee surgeon operates on male patients as well using the skills acquired from female patients.
Discharge at <24 hours post-op is the standard of our clinic and is used in other Scandinavian countries as well. 26 There was no difference observed in the training period, reflecting the unchanged morbidity observed.
In conclusion, using a structured bariatric training program it was possible to eliminate learning curve-related morbidity. We recommend stepwise introduction of new bariatric surgeons in selected patients when learning RYGB in close collaboration with the whole operative team in the training program.
Footnotes
Disclosure Statement
The authors do not have any financial or commercial interest in the study, and no financial or material support was given during the fellowship training program. The authors declare that they have no conflicts of interest.