
Abstract
Abstract
Background:
Laparoscopic ventral hernia repair is evolving rapidly worldwide to become a standard procedure. The purpose of this study was to compare the benefits, effectiveness, and postoperative outcome of laparoscopic transabdominal preperitoneal (TAPP) and intraperitoneal onlay mesh (IPOM) repair of ventral hernia.
Patients and Methods:
Prospectively collected data of 279 patients who underwent laparoscopic ventral hernia repair between January 2005 and December 2009, of whom 68 underwent TAPP and 211 underwent IPOM repair, were retrospectively reviewed. For each patient demographic, preoperative and postoperative data were studied. Statistical analysis was performed by Student's t-test, Fisher exact test, and chi-square test.
Results:
The study included a total of 279 patients, of whom 68 underwent TAPP procedure and 211 underwent IPOM procedure. Both the groups were comparable in age, sex, body mass index, American Society of Anesthesiologists score, mean fascial defect size, and mean size of mesh. Although the operating time was longer in TAPP group than IPOM group of patients, the overall cost of surgery in IPOM group ($752.3±355.7) was much higher than TAPP group ($903.6±28.0) of patients. Seroma formation was more common in IPOM group than TAPP group (8.5% versus 5.8%). There were 2 (2.9%) recurrences in TAPP group and 7 (3.3%) in IPOM group of patients. Mean postoperative hospital stay (1.5±0.6 versus 1.4±0.7 days, P=.35) and mean follow-up (22.7±13.4 versus 22.5±11.9 months, P=.90) were similar in both groups of patients.
Conclusion:
Besides the cost-effectiveness of TAPP procedure, it reduces the risk of complication related to intra-abdominal position of mesh and fixating devices. Before we label the TAPP repair of ventral hernia as the first choice, a comparative multicentric prospective trial with IPOM repair is warranted.
Introduction
In the laparoscopic repair, the mesh is either placed in an intraperitoneal location or in the preperitoneal/retromuscular space. The rise in the intra-abdominal pressure is evenly distributed along each square inch of the mesh and not along suture line, as happens in conventional suture repair. 4 This may account for the strength of the repair and decreased recurrence rates associated with it.
In intraperitoneal onlay mesh (IPOM) placement, the direct contact of mesh with abdominal contents cannot be avoided. Although polypropylene mesh is relatively inexpensive and well incorporated in the abdominal wall, it incites intense inflammatory reaction and adhesion formation. When it is used for intraperitoneal onlay mesh repair, it can cause chronic pain, 5 intestinal obstruction,5,6 enterocutaneous fistula, 7 and infertility 8 and can make future surgery difficult. 9 To overcome these complications, a new generation of meshes has been developed in recent years. The composite or dual-sided meshes offer a conventional material such as polypropylene or polyester in contact with the abdominal wall to promote tissue ingrowth and an inert, potentially adhesion resistant substance such as collagen or cellulose on the visceral side to interface with bowel. 10
Although these new-generation composite prosthetic meshes have definite advantages over polypropylene mesh, such as fewer bowel adhesion and low risk of fistula formation, the bigger disadvantage is their costs. So a low-cost option of transabdominal preperitoneal (TAPP) repair of ventral hernia with less-expensive polypropylene mesh is suggested.
Preperitoneal retromuscular positioning of polypropylene mesh results in negligible adhesion formation and low postoperative complications, 11 as peritoneum acts as an interface between the mesh and bowel.
Preperitoneal mesh implantation ensures adequate abdominal wall reinforcement because of immediate firm fixation of the prosthesis with the intra-abdominal pressure exerted via the peritoneal envelop. 12 In addition, it avoids complication related to the intraperitoneal mesh and the fixating devices.
One of the disadvantages of preperitoneal approach is longer operative time required in dissection and development of retromuscular plane for mesh placement. The aims of this study were to analyze and compare the outcomes of laparoscopic TAPP and IPOM repair of ventral hernia and to determine the benefits and effectiveness of one laparoscopic procedure over the other.
Patients and Methods
A total of 279 patients underwent laparoscopic repair of different types of ventral hernias between January 2005 and December 2009, of whom 68 underwent TAPP and 211 underwent IPOM repair. All procedures were done by a single surgical team headed by the second author at the Department of Minimal Access and Bariatric Surgery, ILS Hospital, Kolkata. For each patient demographic, preoperative and postoperative data were prospectively maintained on Microsoft Office Excel Sheet. Data were retrospectively reviewed and outcomes were recorded. Statistical analysis was performed by Student's t-test, Fisher exact test, and chi-square test of goodness of fit and independence. Student's t-tests were used to compare the mean to determine whether it is significantly different between two groups or not. Fisher exact test and chi-square tests were applied to compare the relationship among categorical variables. A P value of less than .05 was considered to be statistically significant.
Surgical technique
All operations were performed under general anesthesia with patients in supine position. Pneumoperitoneum was established with a Veress needle placed in a virgin area at least 10 cm from the defect margin, mostly in the left hypochondrium. A 5-mm port was placed at that site and a 5-mm 30° telescope was used for initial visualization of peritoneal cavity. Subsequent ports, one 10 mm and another 5 mm, were placed under vision following the principle of triangulation. The 10-mm port was positioned in between the two 5-mm ports and subsequently acted as the optical port. The positions of surgeon, assistant, scrub nurse, and monitor were according to the location of the hernia defects (Fig. 1).
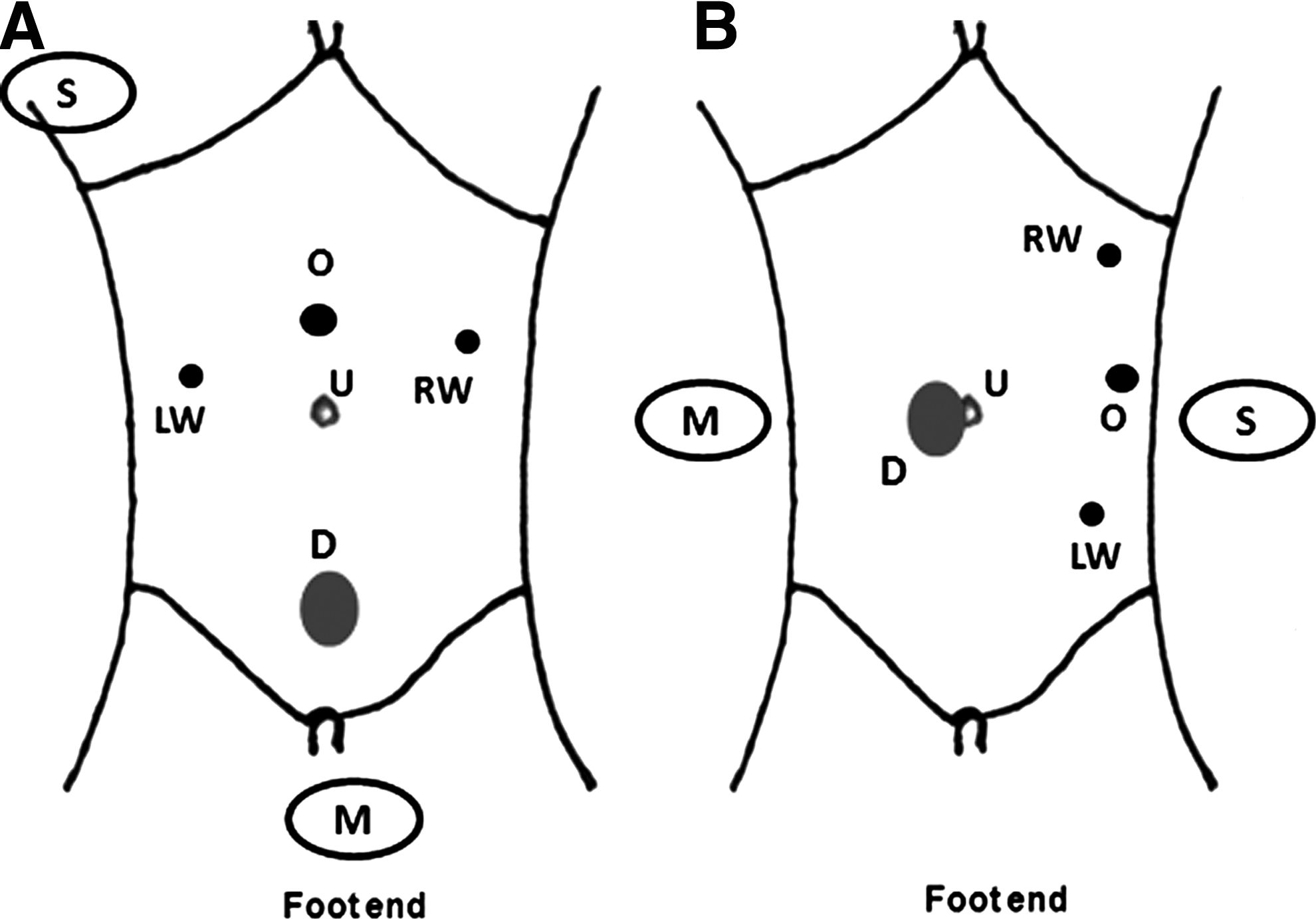
Port position and operation theater (OT) setup.
All abdominal wall adhesions were divided with an ultracision scalpel and contents of hernial sac were reduced. Fascial defect was measured by introducing a sterile plastic tape into peritoneal cavity through the 10-mm port and transverse and cranio-caudal dimensions were recorded. It helped in proper selection of a suitable size mesh, so that the fascial defect was overlapped for 5 cm in all sides. Patients who had lateral and lower midline defects were selected for TAPP repair. Some midline central and upper midline defects were approached by TAPP, especially when it was found easier to raise the flap. However, majority of midline central defects and recurrent midline central defects were repaired with IPOM.
TAPP procedure
A curvilinear incision was made over peritoneum at least 5–6 cm away from the margin of the fascial defect. For midline periumbilical defects, true preperitoneal dissection carries a substantial risk of perforation of peritoneum. So, for these defects, the incision was deepened upto retrorectus level and a retromuscular plane anterior to posterior rectus sheath was developed.
Sac was carefully freed by sharp dissection from adhesions at the fascial defect margin. When complete reduction of the sac was not possible, an incision was made over the neck of hernia, leaving a circular opening in the peritoneum that was subsequently closed by intracorporeal polyglactin suture. The dissection was carried out till 5–6 cm beyond the margin of hernial defect. In case of big midline defects, dissection was continued lateral to rectus sheath and inferiorly beyond arcuate line to apply an appropriate size mesh, and in this situation, some part of mesh was left preperitoneally.
The polypropylene mesh 10 cm bigger than the defect diameter was folded exactly half on itself and a stay suture was put in the center of the mesh so as to coincide it with the center of the hernial defect. Mesh was rolled along its long axis and introduced through the 10-mm port. It was unrolled in preperitoneal space and fixed onto the abdominal wall with helical tacks (Protack; Autosuture, Tyco Health Care, United States Surgical, Norwalk, CT) as well as with intracorporeal 2-0 polypropylene sutures. Reperitonealization was done by intracorporeal continuous suturing of peritoneal flaps with 2-0 polyglactin suture (Fig. 2).
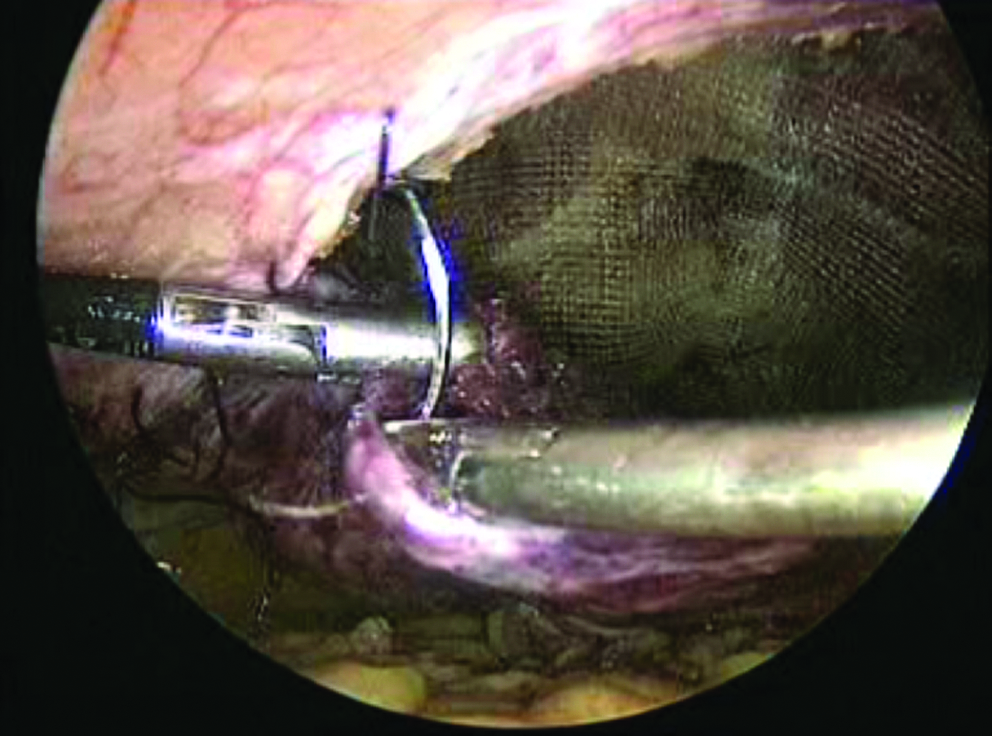
Reperitonealization using 2-0 polyglactin continuous suture in transabdominal preperitoneal repair.
IPOM procedure
Bladder and falciform ligament if found in the field of mesh placement were dissected. Fascial defects of size ≤5 cm were intracorporeally sutured using 2-0 polypropylene continuous suture in two layers. The mesh was folded, introduced, and deployed exactly in the same manner as in TAPP procedure. Care was taken to keep the parietal surface of the mesh toward abdominal wall.
Once the mesh was inside the abdomen, the intra-abdominal pressure was reduced to 6–8 mmHg. The mesh was unrolled and fixed with transfascial sutures with the help of a suture loop created on a sheath of a 20-gauge spinal needle. A total of 6–8 transfascial sutures were placed at the periphery of the mesh. The mesh was further fixed by helical tacks and/or intracorporeal polypropylene sutures placed 1–2 cm apart. Fixations were also placed in the central part of the mesh in a double-crown manner (Fig. 3).
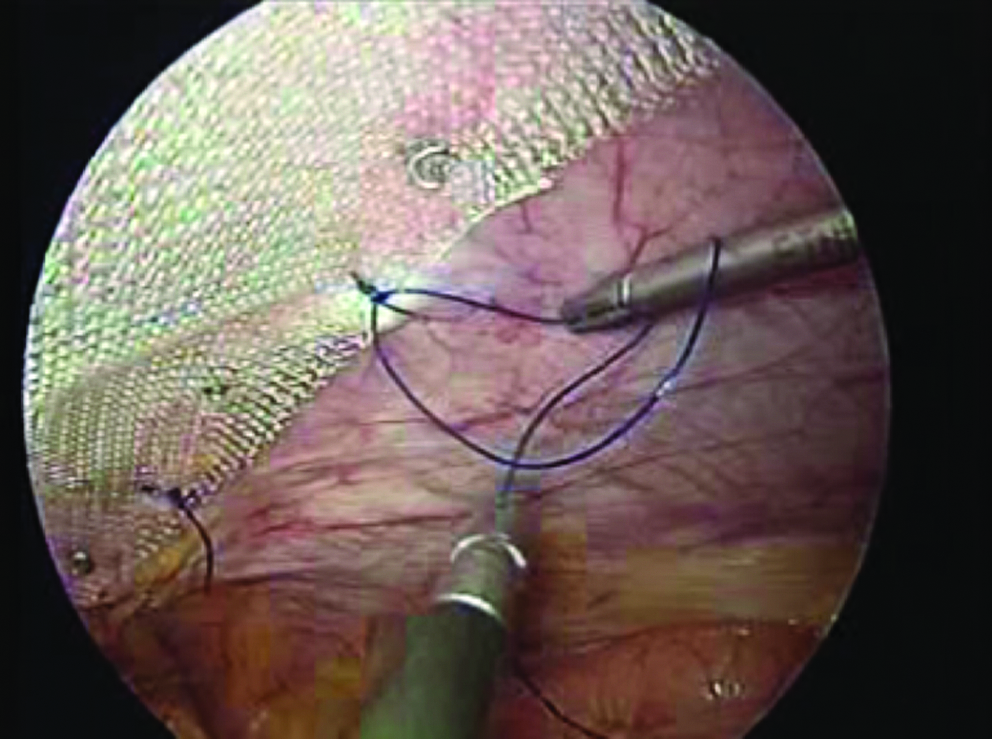
Composite mesh fixation to abdominal wall by tacks and intracorporeal polypropylene sutures in intraperitoneal onlay mesh repair.
At the end of both procedures, the 10-mm port was closed by fascial suture using No. 1-0 polyglactin suture, and a pressure dressing was applied over the operated area and kept for 5 days.
Oral intake was started on postoperative day 1. Postoperatively, patients were followed up after 1 week, 1 month, 3 months, 6 months, and 1 year of operation. Follow-up of all the patients was also attempted on telephonic conversation during the course of data compilation.
Results
A total of 279 patients underwent laparoscopic hernia repair between January 2005 and December 2009, of whom 68 underwent TAPP procedure and 211 underwent IPOM procedure. Both the groups were comparable in age, sex, body mass index, and American Society of Anesthesiologists score (Table 1). There were 26 (38.2%) comorbidity in TAPP group and 71 (33.6%) in IPOM group but of no statistical significance. The different types of hernias and their locations are described in Table 1. Lateral hernias irrespective of them being incisional or primary ventral were repaired with TAPP technique. There was no difference in mean fascial defect size (30.8±24.4 versus 29.9±22.0 cm2, P=.78) and the mean size of mesh (237.8±66.8 versus 240.3±98.2 cm2, P=.84) used in both groups. The mean operating time was significantly more in TAPP group than in IPOM group (96.7±16.7 versus 87.4±15.5 minutes, P=.001). Only prolene mesh (Polypropylene–Ethicon; Johnson&Johnson Ltd., Waley, Aurangabad, India) was used in TAPP procedure. Composite meshes/dual-side meshes were used in IPOM repair except in 1 patient who had intraoperative enterotomy that was closed by intracorporeal 3-0 polyglactin sutures, and in that case, Surgisis mesh (collagen-glycosaminoglycan from porcine intestinal submucosa; Surgisis Gold; Cook Surgical, Bloomington, IL) was used. Different types of composite/dual-side meshes used in IPOM procedure were ePTFE (Dual mesh; WL Gore & Associate, Flagstaff, AZ), Parietex™ (polyester with absorbable collagen; Sofradim, villefranche-Sur-Saone, France), and Proceed (polypropylene, polydiaxonone, and oxidized regenerated cellulose; Ethicon, Somerville, NJ) (Table 2). There was neither conversion from TAPP to IPOM nor from primary laparoscopic to an open approach of hernia repair in this series.
Student's t-test.
Fisher exact test.
Chi-square test of goodness of fit and independence.
ASA, American Society of Anesthesiologists; BMI, body mass index; IPOM, intraperitoneal onlay mesh; TAPP, transabdominal preperitoneal.
Student's t-test.
Chi-square test of goodness of fit and independence.
Use of expensive composite/dual-side meshes ($1034.0±340.8) in IPOM group significantly increased the cost of surgery than the inexpensive polypropylene mesh ($111.7±28.3) used for TAPP group (P<.0001). Although the operating time was longer in TAPP group than IPOM group, the overall cost of surgery in IPOM group ($1752.3±355.7) was significantly much higher than TAPP group ($903.6±28.0) (P<.0001). The overall cost of surgery was calculated by the sum of the costs of mesh, fixating devices, anesthesia, per hour operation theater charge, and hospital stay.
The Visual Analog Scale scores for pain were similar in both the groups on postoperative day 1 (5.1±0.9 versus 5.0±1.1, P=.59) and postoperative day 30 (1.7±0.7 versus 1.6±0.8, P=.37). Prolonged pain persisting for more than 12 weeks was more common in IPOM group at the site of transfascial sutures than in TAPP group (2.3% versus 1.4%) and was managed conservatively but was not statistically significant.
There were a total of 9 recurrences, 2 (2.9%) in TAPP group and 7 (3.3%) in IPOM group, noticed within first 6–18 months of surgery. Only 2 patients from IPOM group opted surgery for recurrence in our hospital. On laparoscopy in these patients, extensive adhesions were found over previously applied composite mesh. One of the recurrences was at the transfascial fixation site, which we believe was due to abdominal muscle ischemia caused by transfascial suture.
Recently the meshes were fixed to abdominal wall with only helical tacks and intracorporeal polypropylene sutures in IPOM group in view of transfascial suture complications (Table 3).
HT, helical tacks; PPS, polypropylene sutures; NTS, nonabsorbable transfascial sutures.
Intraoperative and postoperative complications are mentioned in Tables 2 and 4, respectively. One patient in TAPP group was detected to have hematoma on ultrasound examination anterior to mesh and was managed by sterile needle aspiration and compression bandage. Seroma formation was more common in IPOM group than TAPP group (8.5% versus 5.8%). There was no instance of mesh infection in either group. Mean postoperative hospital stay (1.5±0.6 versus 1.4±0.7 days, P=.35) and mean follow-up (22.7±13.4 versus 22.5±11.9 months, P=.90) were similar in both groups of patients.
Student's t-test.
Fisher exact test.
Chi-square test of goodness of fit and independence.
VAS, visual analog scale.
Discussion
Ventral hernia is a frequent long-term morbidity of open surgery, as they usually develop within the first 5 years of laparotomy.13,14 Hernia surgery has travelled a long journey from suture repair and tension-free mesh repair to recently developed laparoscopic repair. Usher in 1958 was the first who described the use of prosthetic mesh composed of polypropylene to cover the hernial defect 15 and revolutionized the field of hernia surgery with the concept of a tension-free repair. The recurrence rate of tension-free mesh repair of ventral hernia came down to 10%–24%7,16,17 from 24% to 54%16–19 of open suture repair. Rives and Stoppa were the first who used prosthetic mesh preperitoneally for incisional hernia repair. The drawback of this technique is that it requires a wide fascial dissection with flap creation and increases the risk of infection and wound-related complications.7,20 To overcome the complications associated with open tension-free mesh repair, LeBlank and Booth in 1993 developed minimal invasive technique of ventral hernia repair. Laparoscopic ventral hernia repair uses prosthetic meshes, which is placed either intraperitoneally (IPOM) or in preperitoneal/retromuscular space (TAPP). Because of low recurrence rate and all the benefits of minimal access surgery, laparoscopic ventral hernia repair is evolving rapidly to become a standard procedure worldwide. Despite the excellent outcomes of laparoscopic ventral hernia repair, several experimental and clinical studies have reported complications arising from the intraperitoneal placement of prosthetic mesh.
Leber et al. reported that compared with ePTFE, polypropylene mesh had a statistically significant increased rate of adhesion formation, small bowel obstruction, and fistula formation 7 when the mesh was placed intra-abdominally.
Franklin et al. suggested that omental interposition can reduce or eliminate adhesion of viscera to polypropylene mesh. However, in their reoperative case series, they found that one-third of the patients had severe adhesion to polypropylene mesh. 21
The inherent complications related to these meshes led to development of new-generation composite/dual-side meshes. They are characterized by dual surfaces having different properties to promote tissue ingrowth on parietal side and to protect abdominal organ on visceral side. Still, adhesion formation with these meshes is a major concern. 22
Luijendijk et al. reported that neither experimental nor clinical studies provide conclusive information on the efficacy of interposition of polyglactin mesh in preventing adhesion, bowel obstruction, and fistula formation. 17
Based on experimental and clinical studies, it is shown that intra-abdominal preperitoneal/retromuscular (TAPP) placement of polypropylene mesh is a cost-effective feasible option and has minimal postoperative adhesion formation.23–25 It also reduces the risk of complication related to intra-abdominal position of mesh 23 and fixating devices.14,26 Our study shows that TAPP procedure is cheaper compared with IPOM procedure (P<.0001). The operating time is longer in TAPP group than IPOM group (P=.001), because it requires creation of peritoneal flap/retromuscular space and resuturing of flap after mesh fixation. Despite higher operating time, TAPP procedure is economical as IPOM procedure involves use of expensive composite/dual-side meshes.
The method of mesh fixation in laparoscopic surgery is not yet standardized. Many authors advise to use transfascial sutures, because it has higher holding strength compared to tacks and results in low recurrence rate.27,28 Other authors argue to use tacks contrary to transfascial sutures, because it reduces operating time and postoperative pain and maintains similar recurrence rate.28–30 Recently, Nguyen et al. 31 and Wassenaar et al. 32 reported that patients undergoing laparoscopic ventral hernia repair with transfascial sutures or tacks experience similar overall postoperative pain. In our study, prolonged pain was more common at the site of transfascial sutures compared to tacks (2.3% versus 1.4%).
Transfascial suture has the potential to cause abdominal wall ischemia leading to recurrence, as found in one of our patients. Because of this observation and of prolonged pain, we have recently changed our practice of using only spiral tacks and 2-0 intracorporeal polypropylene sutures for mesh fixation.
The most important and tedious part of laparoscopic ventral hernia repair is adhesiolysis, which can lead to serosal tear, enterotomy, and injury to omental vessels. Reported overall incidence of bowel injury is 1%–5%.33,34 Our study has eight (2.8%) bowel injuries (seven serosal tears and one enterotomy). This is in conjunction with reported literature.
There is a possibility of inferior epigastric artery injury during development of preperitoneal/retromuscular planes, and hence, the rate of postoperative hematoma formation is slightly higher in TAPP procedure. In our series, 1 patient (1.44%) developed hematoma postoperatively in TAPP group and was managed conservatively. Reported incidence of postoperative hematoma in IPOM repair series is 1%–15%28,35; however, in our series, no such complication was seen.
Most frequently reported complication of laparoscopic ventral hernia repair is seroma formation. Most of the seromas develop anterior to the mesh and within retained hernial sac. The mean incidence of seroma at 4–8 weeks is 11.4% in a large reported series. 19 In the largest multi-institutional trial, seroma that were clinically apparent after more than 8 weeks postoperatively were considered a complication and occurred in 2.6% of the patients. 20
In this series, 4 patients (5.8%) had seroma formation in TAPP group and 18 patients (8.5%) in IPOM group in early postoperative period and resolved after 8–12 weeks with conservative management. During the dissection of preperitoneal (retromuscular) space in TAPP group, most of the hernial sacs were totally dissected down, or in cases wherein the sac was tethered to scarred tissue, partial dissection of sac was done. We believe that low seroma formation in TAPP group was probably due to hernial sac excision and this reason of low seroma formation after sac excision is also supported by literature. 36
In our series, the recurrence rate in IPOM group (3.3%) is higher than in TAPP group (2.9%). The overall reported recurrence rate of laparoscopic hernia repair (IPOM) is 3.8%–5.6%.19,37 Similar recurrence rate as shown in our TAPP group was reported by Chowbey et al. in their series of 34 patients who underwent ventral hernia repair with extraperitoneal mesh. 24
In this series, the mean postoperative hospital stay was 1.5±0.6 days in TAPP group and 1.4±0.7 days in IPOM group. This finding is well supported by other studies in which mean hospital stay was between 1.25 and 1.5 days.28,38
Conclusion
Laparoscopic technique of ventral hernia repair is evolving rapidly and becoming a standard procedure worldwide because of its low recurrence rate and all the benefits of minimal access surgery. Except longer operating time, TAPP procedure has several advantages over IPOM repair. Our study shows that TAPP procedure is cheaper and has low complication rate compared with IPOM procedure. The less-expensive mesh used in TAPP procedure is within the reach of general population. Besides the cost-effectiveness of TAPP procedure, it reduces the risk of complication related to intraperitoneal position of mesh and fixating devices. A comparative multicentric prospective trial with IPOM repair is warranted to further substantiate these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.