
Abstract
Abstract
Aim:
Single-incision laparoscopic colectomy (SILC) often requires steeper Trendelenburg positioning to displace or keep the small intestine away from the operative site. We have developed hybrid SILC in which we make a transumbilical incision to extract the specimen first and utilize a multiflap gate (MFG).
Methods:
MFG was inserted through a 4.0-cm transumbilical incision, and a surgical towel was inserted via MFG and displaced the small intestine away from the operative site. Three 5-mm ports were placed in the converter sheet. Almost all the operative procedures were the same as usual laparoscopic sigmoidectomy. In the course of laparoscopic procedures, whenever we felt stress, we used the techniques of open surgery via MFG.
Results:
In 3 patients, the procedure was successfully completed without any complications.
Conclusions:
Our procedure can be easily performed, which enables surgeons to achieve SILC safe and easy compared with conventional technique.
Introduction
In colorectal surgery, one of the first steps in the operation is the effective displacement of the small intestine away from the operative site. In open surgery, surgical towels, sponges, and intestinal bags have been used to displace the small intestine away from the operative site. In conventional laparoscopic approach, these devices cannot be used, and optimal surgical exposure remains a serious challenge especially in the field of SILC. SILC often requires steeper Trendelenburg positioning and longer operative times when compared with traditional laparoscopic surgery, which may lead to any complications.4,5 We have developed hybrid SILC (H-SILC) in which we can insert the surgical towel and displace small intestine atraumatically through the small incision. Moreover, in H-SILC, we can perform some procedures using the techniques of open surgery through a small incision when we feel difficulty to achieve. This is the report on H-SILC performed for sigmoidectomy in advanced colon cancer with lymph node dissection.
Methods
Surgical technique
Under general anesthesia, the patients were placed in the modified lithotomy position. First, a multiflap gate (MFG; Sumitomo Bakelite, Tokyo, Japan) was inserted through a 4-cm transumbilical incision, the wound was protected, and the operative field was secured (Fig. 1). Next, a sterilized cotton surgical towel, measuring approximately 40×40 cm when unfolded, is soaked with warm saline and inserted into the peritoneal cavity with the surgeon's hand via the MFG. The towel is placed over the small intestinal loops under direct visualization. The loops of bowel can then be gently housed inside the towel and carefully displaced away from the operative site (Fig. 2). Three 5-mm ports were placed in the converter sheet of the MFG (Fig. 3). Almost all the procedures were performed with usual laparoscopic instruments such as the Harmonic ACE (Ethicon Endo-Surgery, Cincinnati, OH), and the operative procedures were much the same as in usual laparoscopic surgery using a flexible 5-mm scope. The laparoscopic instruments and operative procedures were much the same as in usual laparoscopic sigmoidectomy but using a flexible 5-mm scope. The sigmoid colon was mobilized using a medial approach. All of the soft tissue anterior to the inferior mesenteric artery was completely removed (D3 lymph node dissection). Then the root of the superior rectal artery and inferior mesenteric vein were divided. In the course of these procedures, whenever we felt stress including the unfavorable visual field, the low tension under the tissue to be dissected, and the conflictions among laparoscopic instruments, we performed some procedures using the techniques of open surgery through a small incision with MFG. The specimen was extracted through the small incision. Resection was achieved after extracorporealization, and the anastomosis was extracorporeally performed using staplers.
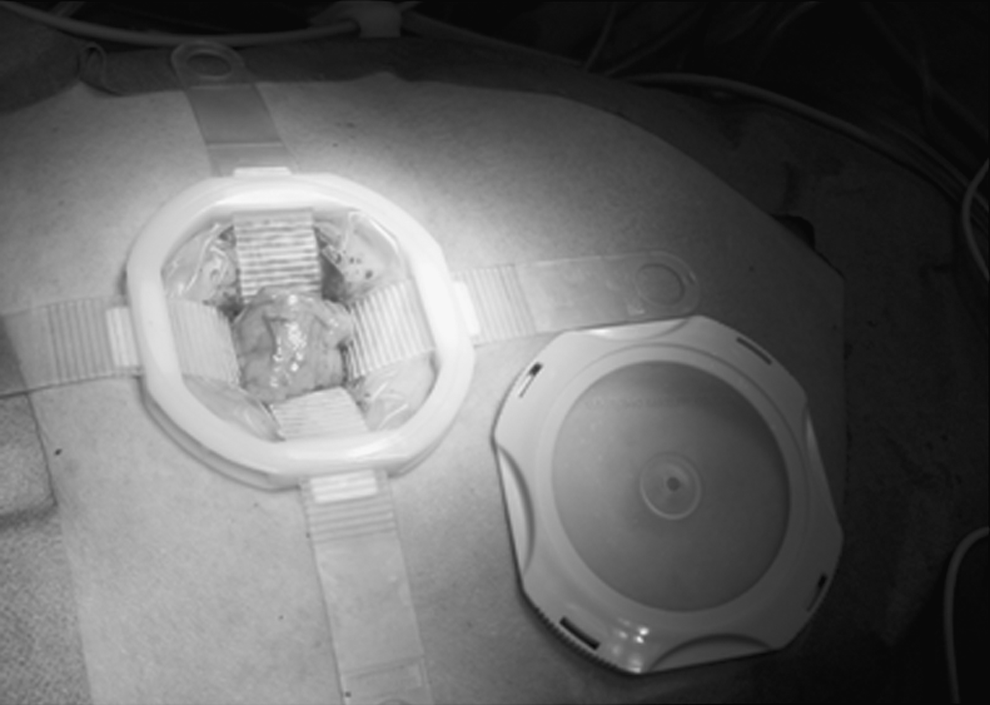
A multiflap gate (MFG; Sumitomo Bakelite, Tokyo, Japan) was inserted through a 4.0-cm transumbilical incision, the wound was protected, and the operative field was secured.

Displacement of the small intestine away from the operative site was achieved by a surgical towel.

Three 5-mm ports were placed in the converter sheet of the MFG.
Results
We underwent H-SILC sigmoidectomy with lymph node dissection in 3 patients. There were 2 women and a man with a mean age of 65 years (range: 38–85 years). Body mass index (BMI) was 18.8–20.7 (mean: 19.6). Two patients of the 3 underwent D3 lymph node dissection. In these 3 patients, all procedures were successfully completed without any perioperative complications. In all cases, there was no need to extend the skin incision. Average operative time was 149.0 minutes. In all cases, intraoperative blood loss was less than 20 mL. The numbers of harvested lymph nodes in patients with adenocarcinoma were 15 and 17 in patients with colon cancer. Postoperatively, pathologic findings revealed adenocarcinoma in 2 cases and adenoma in 1 case. The UICC 7th edition (TNM) stages of the two cancers were I and IIA. Patients were discharged between postoperative days 9 and 11. Postoperative follow-up did not reveal any umbilical wound complications or recurrences.
Discussion
Many surgeons have attempted to reduce the number and size of ports in laparoscopic surgery to decrease parietal trauma and improve cosmetic results, and recently, single-incision laparoscopic surgery (SILS) has been developed, 6 leading to laparoscopic procedures performed with trocars located at one umbilical incision.
In SILS, needless to say, the basic principles in the management of surgical patients, however, have not changed: adequate optimal exposure of the operative site and good lighting remain important and may become more important with this unique laparoscopic technique. In colorectal surgery, the effective displacement of the small intestine away from the operative site is the key to success, because it normally spills into all quadrants of the abdomen. We generally use surgical towels, sponges, and intestinal bags to displace the small intestine away from the operative site in open surgery. In conventional laparoscopic approach, however, these devices cannot be used, and optimal surgical exposure remains a serious challenge. Laparoscopic colectomy, therefore, requires steep Trendelenburg positioning to acquire the proper surgical field or to prevent the remigration of the small intestine after displacement.
Generally, SILC requires steeper Trendelenburg positioning to keep proper surgical site and longer operative time than conventional laparoscopic surgery. Trendelenburg positioning and pneumoperitoneum for many hours cause elevations in the stress hormones and concurrently cause a decrease in hemodynamic parameters.4,5 A healthy patient may tolerate these changes but a patient with cardiovascular disease or pulmonary problems may not be able to compensate as efficiently. In H-SILC, we can insert the surgical towel via MFG and displace small intestine atraumatically in a short time under direct visualization. This technique proves easy optimal exposure of the operative site and keeps this without steep Trendelenburg positioning, minimizing the risk of complications. Only H-SILC can benefit from this technique, because it is extremely challenging to insert and handle large surgical towels inside the peritoneal cavity with standard SILC techniques. There is only one technical report that refers to the usefulness of the MFG in laparoscopically assisted distal gastrectomy, but no reports that mention the use of MFG in SILC have been described.
In this study, the BMIs of our patients were extremely low. Generally, in laparoscopic procedures, patients with high BMI require steeper Trendelenburg positioning than patients with low BMI to acquire proper surgical field in a fatty intra-abdominal space. Therefore, we believe that the insertion of the surgical towel via MFG may offer more advantages in patients with high BMI.
In H-SILC, we can perform some procedures using the techniques of open surgery through a small incision. We can acquire not only proper understanding of anatomic structure or assistance of procedures with the dynamic development of surgical field or the sense of touch from the open procedures, but also delicate procedures under the magnified visualization from laparoscopy.
Concerning about hospitalization, our patients stayed in our hospital for 9–11 days after operation. This is mainly owing to the healthcare system in Japan. There are not many welfare institutions, and the healthcare expenditure is inexpensive in our country. However, we believe our technique raises the safety and quality of the operation and might offer benefits to the patients in short-hospitalization systems such as the United States.
We presented initial experience of hybrid single-incision laparoscopic sigmoidectomy for colon cancer. This procedure is a promising alternative method as minimally invasive abdominal surgery for the treatment of some patients with colorectal disease.
Footnotes
Disclosure Statement
No competing financial interests exist.