
Abstract
Abstract
Robotic-assisted ureteral reimplantations were performed on 3 patients at a single institution, 2 with Boari flap and psoas hitch and 1 with psoas hitch alone. These were for urothelial carcinoma of the distal ureter, ureteral obstruction caused by distal ureteral endometriosis, and ureteral transaction during gynecologic surgery. We used intraoperative ureteroscopy to confirm tumor margins as well as a simple technique for retrograde placement of transvesicle wire prior to ureteral anastomosis. Surgery and recovery were uneventful. This illustrates that robotic-assisted ureteral reimplantation with Boari flap and psoas hitch is a safe and viable approach for ureterovesicle reconstruction.
Introduction
Patients and Methods
After institutional review board approval, patient data from robotic-assisted cases were prospectively collected. A single surgeon (L.A.D.) performed three robotic distal ureteral reimplantation procedures between October 2008 and December 2009.
Patient 1
A 71-year-old man with low-grade urothelial carcinoma localized to the distal left ureter as diagnosed on ureteroscopic resection was evaluated. After preoperative consultation regarding treatment options, the patient decided on robotic-assisted distal ureterectomy with ureteral reimplantation.
The procedure was performed under general anesthesia in the low lithotomy, steep Trendelenburg position. Cystoscopy was used to confirm the absence of bladder lesions, and a guidewire was placed through the left ureteral orifice into the renal pelvis. A 16-French Council catheter was placed to drain the bladder, alongside the ureteral guidewire.
The abdomen was inflated with CO2 using a Veress needle up to 20 mm Hg, prior to inserting a 5-mm Ternamian EndoTIP (Karl Storz, Tuttlingen, Germany) trocar in the right upper quadrant under direct vision with a 0-degree lens. Under direct vision, a 12-mm Endopath XL (Ethicon Endosurgery, Cincinnati, OH) trocar was placed into the umbilicus and two 8-mm da Vinci cannulae were placed 17 cm from the pubic symphysis and 10 cm lateral to midline. An additional 8-mm da Vinci cannula was placed in the left lateral aspect of the abdomen and a 12-mm Endopath XL assistant port was placed into right lower quadrant. The da Vinci S robot was docked (Fig. 1).
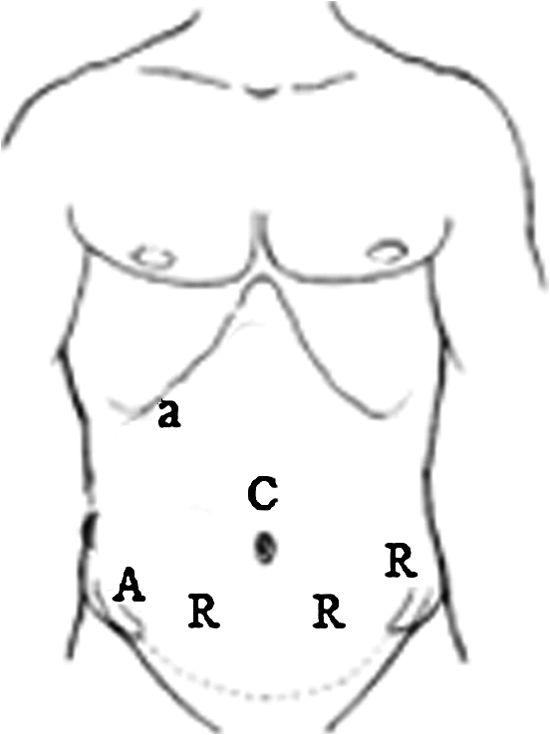
Port-site placement for robotic-assisted right or left distal ureterectomy with Boari flap and psoas hitch. A, 12-mm assistant port; a, 5-mm assistant port; R, 8-mm robot ports; C, 12-mm camera port.
Upon entering the abdomen, the line of Toldt on the left was incised to allow for medial reflection of the sigmoid. The left ureter was easily identified and mobilized from the ureterovesical junction to the level of the iliac vessels. The bladder was filled with 200 mL saline to allow for lateral mobilization of the bladder, involving transecting the urachus and incising the peritoneum lateral to each median umbilical ligament.
An assistant then placed a flexible ureteroscope over the existing ureteral guidewire to identify the proximal and distal borders of the tumor. This was identified on the extramural ureter by turning off the light source to the robotic camera and identifying the position of the ureteroscope light through the ureter. These borders were marked using robotic cautery, leaving an extra 1 cm margin (Fig. 2). Hem-o-Lok (Teleflex Medical, Research Triangle Park, NC) clips were distally (to prevent spillage) and proximally placed, and the ureteral tumor was removed en bloc with a cuff of bladder. Frozen sections of the margins were negative.
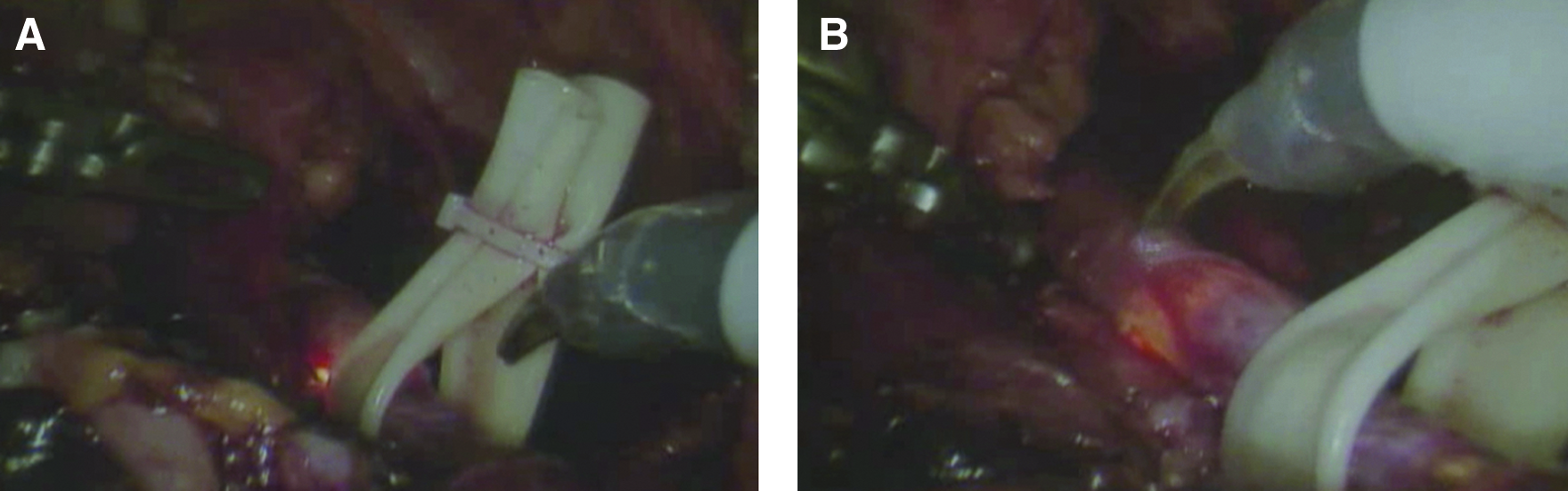
Flexible ureteroscopy during robotic distal ureterectomy to identify borders of tumor.
A broad-based flap of bladder was opened with scissors to form the Boari flap (∼7 cm in length with a 4 cm base and 2.5 cm tip) and the distal ureter was spatulated with Potts scissors. A psoas hitch was performed to the left psoas muscle with a 2-0 Vicryl suture in the direction of the muscle fibers. The posterior aspect of the Boari flap was anastomosed to the distal ureter with running 4-0 Monocryl. A new guidewire was passed through the anastomosis by first introducing the proximal end through the Council catheter into the bladder and out through the opened bladder (Fig. 3). This was proximally guided up the ureter with the aid of the robotic arms. The anterior aspect of the anastomosis was closed with 4-0 Monocryl, and the flap was tubularized in two layers with 3-0 Monocryl. The bladder was checked for leaks by instilling saline. After the robot was undocked, a 6-French ureteral stent was placed under fluoroscopic guidance over the guidewire.
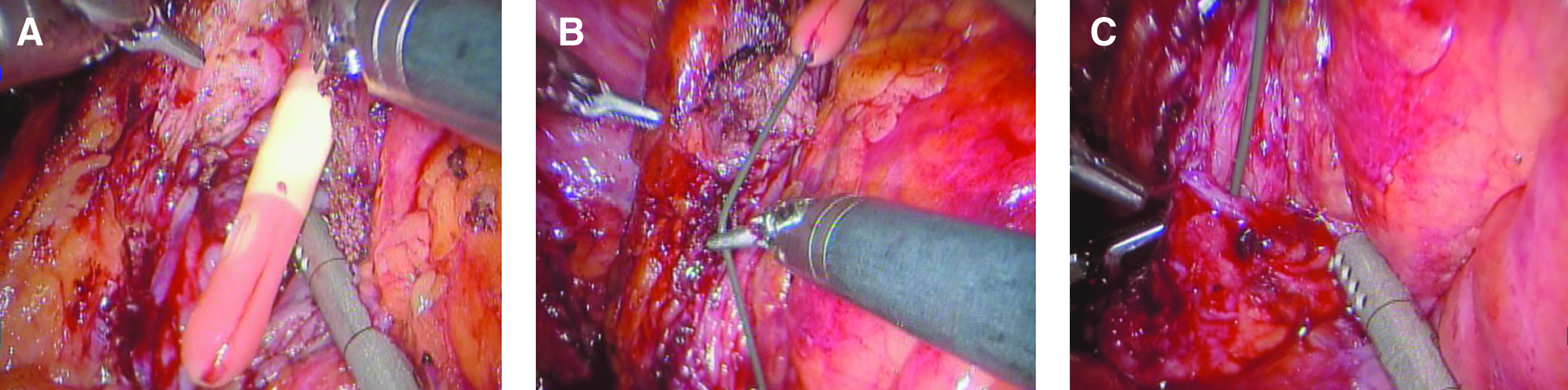
Transvesical ureteral wire placement during robotic distal ureterectomy with Boari flap.
Patient 2
A 28-year-old woman with bilateral hydronephrosis discovered during the workup of chronic renal insufficiency was evaluated. Bilateral ureteral stents were placed to relieve ureteral obstruction, and nuclear renal scan showed nonfunction of the left kidney. Ureteroscopy revealed a polyp extending 3 cm within the distal right ureter, and biopsy confirmed nonmalignant etiology. The patient decided on robotic distal ureterectomy because of the length of ureter involved.
Surgery proceeded similar to Patient 1, including positioning and placement of ports. The cecum was mobilized as the right ureter was involved. Ureteroscopy was intraoperatively utilized to delineate the margins of the polyp. After excision of the diseased segment, the distal ureter was able to reach the bladder with only a psoas hitch. After spatulation of the ureter and posterior anastomosis, a guidewire was once again passed through the Council catheter through the bladder and past the anastomosis. The anastomosis was completed, and bladder was confirmed to be watertight. A 6-French ureteral stent was fluoroscopically placed at the end of the case.
Patient 3
A 44-year-old woman who had transection of the right ureter during a gynecologic procedure, discovered 3 weeks later because of flank pain and hydronephrosis, was evaluated. She had a percutaneous nephrostomy tube placed and a retroperitoneal drain for a large urinoma. Antegrade and retrograde imaging studies showed extravasation of contrast from a complete transection of the midureter, 6 cm gap between the distal aspect of the proximal ureter and the proximal aspect of the distal ureter (Fig. 4). After several months of decompression, she decided on robotic ureteral reimplantation. Because of the anticipated length of ureteral defect, the patient was consented for a psoas hitch, Boari flap, and possible ileal ureter.
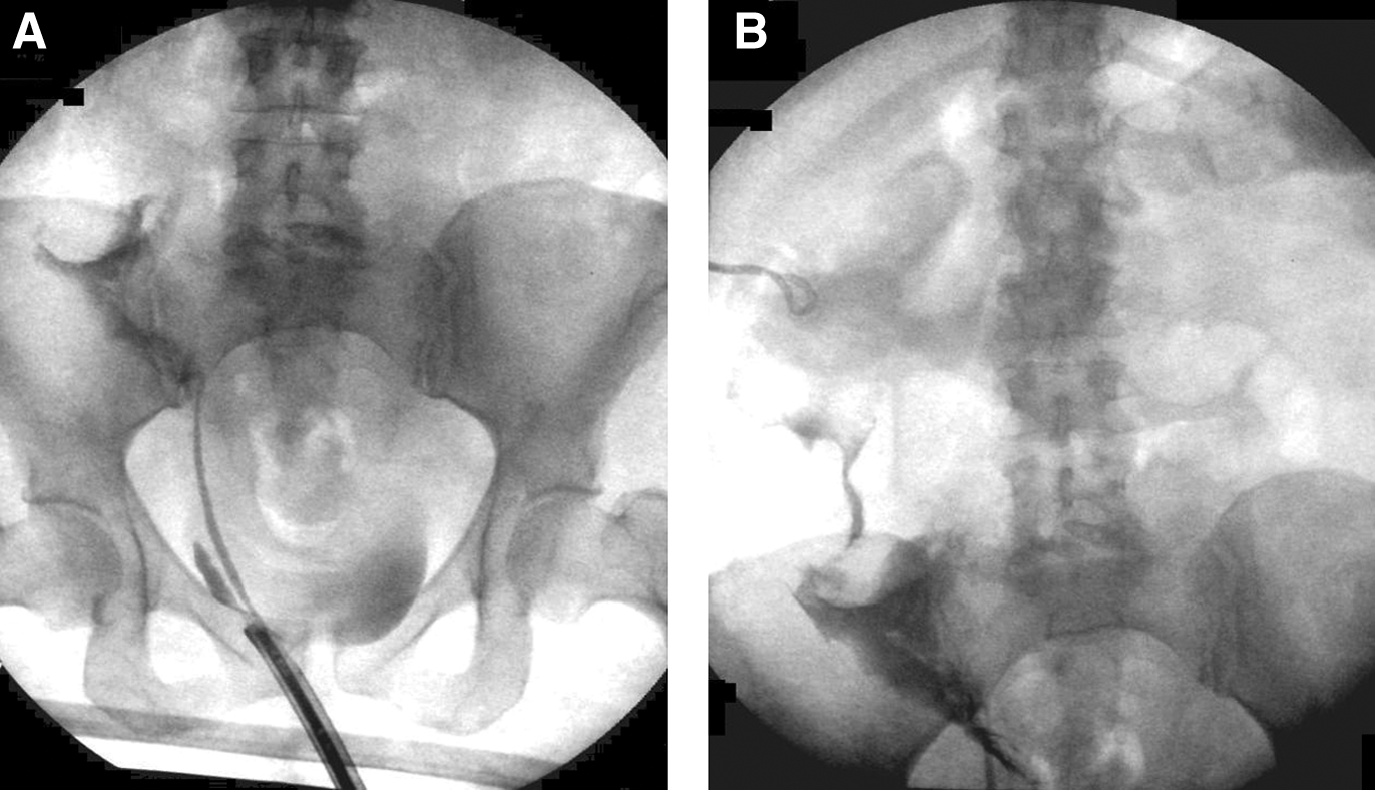
Patient with ureteral transection.
Surgery proceeded similar to the first 2 patients. The existing right percutaneous nephrostomy tube was capped at the beginning of the procedure to allow for distension of the blind-ending ureter. Port placement was identical, and there were extensive adhesions surrounding the cecum. The distal aspect of the proximal ureter was identified at the level of the external iliac vessels and mobilized. The nephrostomy tube was uncapped and distal ureter was transected and spatulated with Potts scissors. The bladder was mobilized as described earlier, and a Boari flap of 5 cm at the base and 7 cm long was created. Once again, placement of the ureteral guidewire was achieved through the Council catheter in the bladder with the assistance of robotic arms, and the anastomosis between the ureter and flap was performed with a running 4-0 Monocryl suture. After closure of the bladder, it was confirmed to be watertight by flushing saline through the catheter. A 6-French ureteral stent was placed at the end of the case, and the right percutaneous nephrostomy tube was kept in place.
Results
Table 1 gives a full description of the results. The median estimated blood loss was 100 mL (range, 50–200 mL). There were no urologic complications of any of the cases, although Patient 1 developed paroxysmal atrial flutter that was medically managed and did not delay his discharge. The median hospital stay was 4 days (range, 4–6 days).
The patients' bladders were kept decompressed with catheter drainage for a median of 17 days (range, 10–19 days), with radiographic absence of extravasation prior to catheter removal for the 2 patients with Boari flaps. The ureteral stents were endoscopically removed through a separate procedure between 1 and 3 months postoperatively.
Final pathology for Patient 1 showed no residual urothelial carcinoma, for a surgical pathologic stage of pT0NxMx. He was lost to follow-up after removal of the ureteral stent.
Final pathology for Patient 2 showed endometriosis, with margins free of disease. Renal ultrasound for Patient 2 at 2 years postoperatively showed no ipisilateral hydronephrosis (Fig. 5).
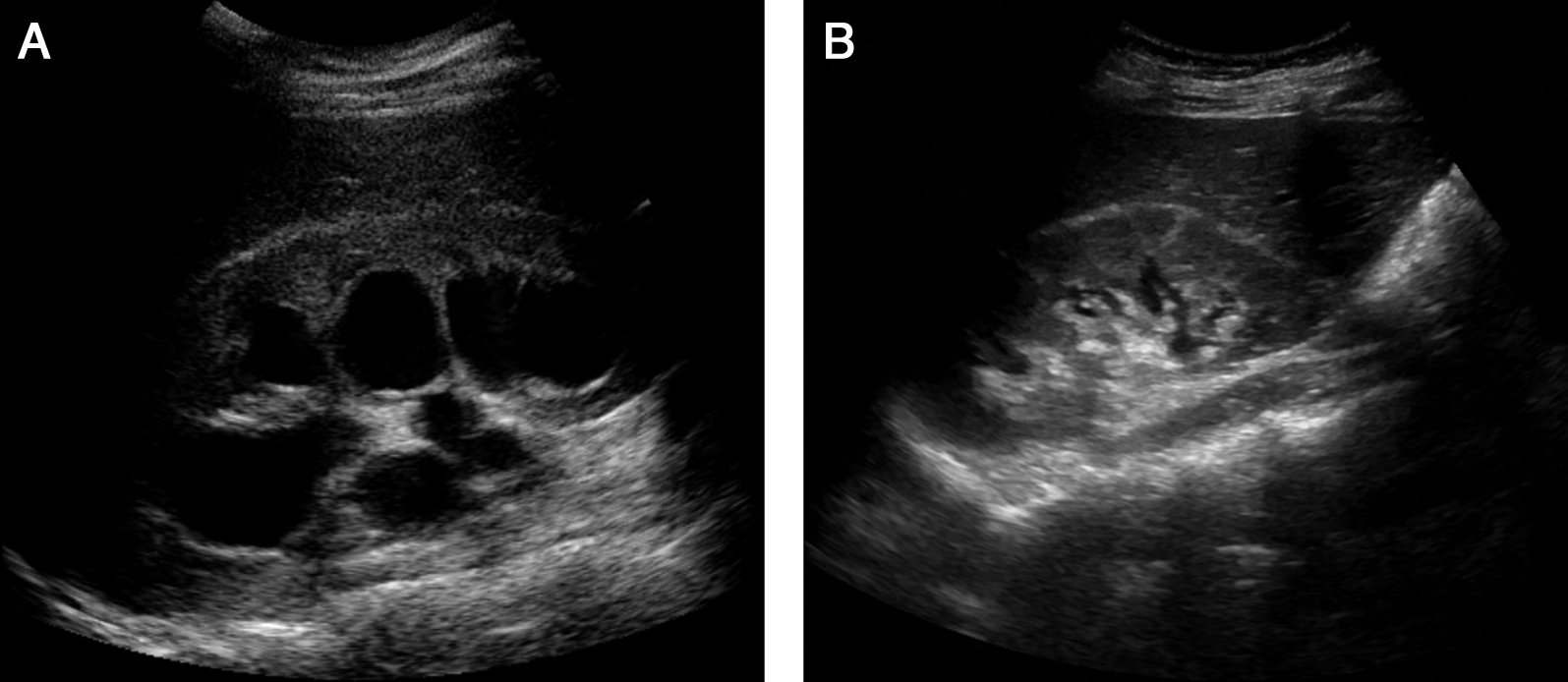
Ultrasound images of right kidney for patient with endometriosis of right distal ureter.
Patient 3 did not initially follow up as instructed postoperatively. Three months after her procedure, she returned to clinic where we scheduled her ureteral stent removal. We performed this endoscopically and performed an antegrade ureterogram through her percutaneous nephrostomy tube showing a patent ureter without extravasation of contrast, with free drainage to the bladder. The percutaneous nephrotomy tube was then removed.
Discussion
We had similar early success as previous authors with our Boari flap reconstructions.1,2 The three-dimensional visualization, ease of intracorporal suturing, and improved degrees and freedom of movement offered by the da Vinci robot aided in the pelvic dissection, creation of the Boari flap, and ureteroneocystostomy. We used the same port placement in both right- and left-sided procedures and did not experience difficulty in reaching the left pelvic wall with the assistant instruments.
During a robotic2–8 or laparoscopic9–14 ureteral reimplantation, the most common method to place a stent into the ureter has been by feeding a wire transcorporally through a trocar into the proximal ureter, guiding the proximal portion of the stent over the wire into the ureter, removing the wire, and then using instruments (robotic or laparoscopic) to guide the distal part of the stent into the bladder. This can be challenging because of loss of insufflation during trocar manipulation, need to manipulate the curls of the stent, or a sharp angle between the insertion of the wire and course of the ureter. Others have accomplished wire/stent placement through a separate needlescopic port15,16 or cystoscopically.17,18
Here, we describe a simple method using a Council catheter for retrograde transvesical ureteral wire placement during laparoscopic or robotic distal ureteral reimplantation. At the time of wire placement, the bladder already has a large opening for the Boari flap. Thus, it is easy to manipulate the wire into this opening. Assistance of the robotic arms makes it simple to guide the wire into the ureter. We complete the ureter-flap anastomosis over the bare wire, although placement of a ureteral stent prior to the anastomosis, if desired, would be possible as well.
We also describe use of intraoperative ureteroscopy with simultaneous laparoscopy to visually define ureteral tumor margins and ensure transection at a site where there is no visible tumor. 19 We keep the ureteroscope light at maximum brightness and hold it aligned with the distal or proximal margin of the tumor. Then, by turning off the robotic light, we are able to identify each margin and superficially mark the ureter using electrocautery. It is also possible to project the ureteroscopic images onto the da Vinci console screen using the TilePro feature, although we did not use this feature in these cases. Although this adds time to the procedure, this gives us visual confirmation of a grossly negative margin, which was subsequently microscopically confirmed.
Conclusions
This case series supports the use of robotic assistance for distal ureterecotomy with ureteral reimplantation using Boari flap and/or psoas hitch techniques. Using a Council catheter may aid in retrograde transvesical wire access to the ureter prior to ureteral reanastomosis. Intraoperative ureteroscopy can give visual confirmation of ureteral tumor margins prior to excision.
Footnotes
Disclosure Statement
No competing financial interests exist.